 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.






GermanCol
![]()
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Sluicebox. what you are mentioning that Doctor Ashkan said that less than 10% of the patients didn't crossover would help in a theory I have that I mention in this post:
https://investorshub.advfn.com/boards/read_msg.aspx?message_id=169301316
Can you let me know in what part of the conference he says that and what exact words does he use? English is not my native language, so I don't understand some of the words I heard from the conference.
Thanks a lot in advance.
I agree with Flipper that we could have around 40 or even more beating hearts at 5 years. The reasons are the following.
First of all, from the rGBM arm there could perfectly be more than the 2 patients shown at 5 years on slide 39 of the final presentation, because those 2 are counted from recurrence, not from randomization.
On the other hand I'm starting to think that part of the 35 people not included in the trial arms of the final presentation (nGBM arm and rGBM arm) were patients in the initial control arm of the trial (part of the 99) that at some point, after the study started, were thought to be progressors, but then it was realized they were pseudoprogressors.
If this is the case, because of being initially thought to be progressors, they received DCVax after pseudoprogression. As a consequence of that, these patients could not be part of any of the two trial arms. They were not progressors when they received DCVax, so don't correspond to the rGBM arm and they didn't receive DCVax at the beginning of the trial, so they also could not be part of the nGBM arm.
That would explain why we had 13 left censored patients (lost to follow) in the JTM interim publication for the first 19 months from surgery and now we have zero in the treatment arm for nGBM from the final presentation.
I was wondering what happened with these pseudoprogressors from the control arm that recieved DCVax at pseudoporgression. This theory kind of solves that question for me as not being included in the rGBM arm, that I think is the correct thing to do. But I could be wrong.
Sluicebox mentioned in his/her reply to you that Doctor Ashkan said that less than 10% of the patients didn't crossover. That would reinforce my theory because we know that at least 89% received DCVax-L ( (232+64)/331 = 89%). So maximum 11% didn't receive it. If the number is less than 10%, that would mean that part of the 35 patients received DCvax at some point and could correspond to the group of pseudopregressors that received DCVax at progression.
Other thing that could be in agreement with my theory is that in slide 11 of the final presentation there are 81 PFS events coming from the 99 placebo arm patients. So there are 17 patients (81 - 64 ) that were clasiffied as PFS (not as cPFS (confirmed progression-free survival)) but not included in the 64 rGBM arm. So they could correspond to the pseudoprogressors initailly thought to be progressors.
In a previous post I mentioned that according to my numbers, part of the 35 patients could be living longer. In the Table below are these calculations. The rows in yellow correspond to the 2 trial arms from the final presentation, the dark gray corresponds to the interim JTM publication and the light gray is calculated from all the other infomation in order to obtain the same mOS of the interim publication

With all this in mind I expect even better results that what we have seen until now. I think this trial is a total success. We just need to be patient.
Thanks a lot Lykiri, for this and all your support to this board.
Likiri, before the final results, the only information I saw where I was able to read or find the number of censors, was the JTM publication. In that one I concluded there were 13 left censored patients between 0 and 19 months. Can you please share with me a link to that update flipper mentions? I don't think I have seen it. I remember a PR with an update and a presentation at ASCO in 2018, but with no information about censors.
Thanks
Before the final results, the only information I saw where I was able to read or find the number of censors, was the JTM publication. In that one I concluded there were 13 left censored between 0 and 19 months. Can you please share with me a link to that update you mention? I don't think I have seen it. I remember a PR with an update and a presentation at ASCO in 2018, but with no information about censors.
Thanks
You're very welcome Senti. I am trying to think why those lost to follow could have been taken out of the study. Could it be something a regulatory agency or somebody else (peer reviewer, consultant, etc.) asked them to do for being part of the earliest time of the trial and as such, having problems with other recruitment and initial information also?
Thanks Flipper44 for your words and feedback. I agree with you that the lost to follow could have been found afterwards or distributed. It's just that I think is more probable that the majority were not found after all that time. And because of that, my theory is that they were just taken out of the study. I also think that, because apparently we don't have censors in the DCVax-L arm final results for the first 2 years.
I think I should have written a little bit different and it is that the 13 could have been part of the crossovers or of the non crossovers, but then just taken out of the study because they were lost to follow and maybe from the earliest part of the trial. What I don't know is why those lost to follow could have been taken out of the study, could it be something a RA asked them to do that for being part of the earliest time of the trial?
PUTTING TO REST THE LIES SPREAD ABOUT NWBO PHASE III TRIAL - PART 5
Continuing with the analysis of the Phase 3 final results presentation, I observed additional things that I would like to share.
Let’s start remembering 2 definitions:
- Left censored patients: Patients that were lost to follow at the time of a survival analysis.
- Right censored patients: Patients that were in the trial and alive at the time of a survival analysis and will continue in the trial. We don't know how long they are going to live and at the time of the analysis they have been in the trial the time shown as a censor (small vertical line in the JTM publication charts).
Now, after that, let’s start with the things observed.
1. An important reason why interim blended results showed a higher mOS than nGBM DCVax-L arm final results did is that in the latter there were no censored patients included at least for the first 19 months and in the former there were 13. Also, all these 13 were left censored (lost to follow), so the ones corresponding to the treatment arm should have been included also in the final results in order to make them comparable. And more important, not including them resulted in obtaining a lower mOS.
2. DCVax-L treatment arm showed statistically significant benefits vs. external control arms in a situation were DCVax-L results were punished taking left censored (lost to follow) patients out for at least the first 19 months, while in the external controls arm they were not taken out. This is true because censored patients help to get better survival results, as I will explain below.
3. With the conclusions 1 and 2 above and analyses from my previous posts, I think that the group of 35 non crossover patients is composed of the 22 non crossover patients with unknown MGMT methylation calculated before and the 13 lost to follow patients (censored left) that were not included in the DCVax-L arm. Not even the ones that started in the original treatment arm.
Now these are the reasons why I came to these conclusions:
a. Why am I saying that there were 13 censored patients at the time of the JTM analysis?
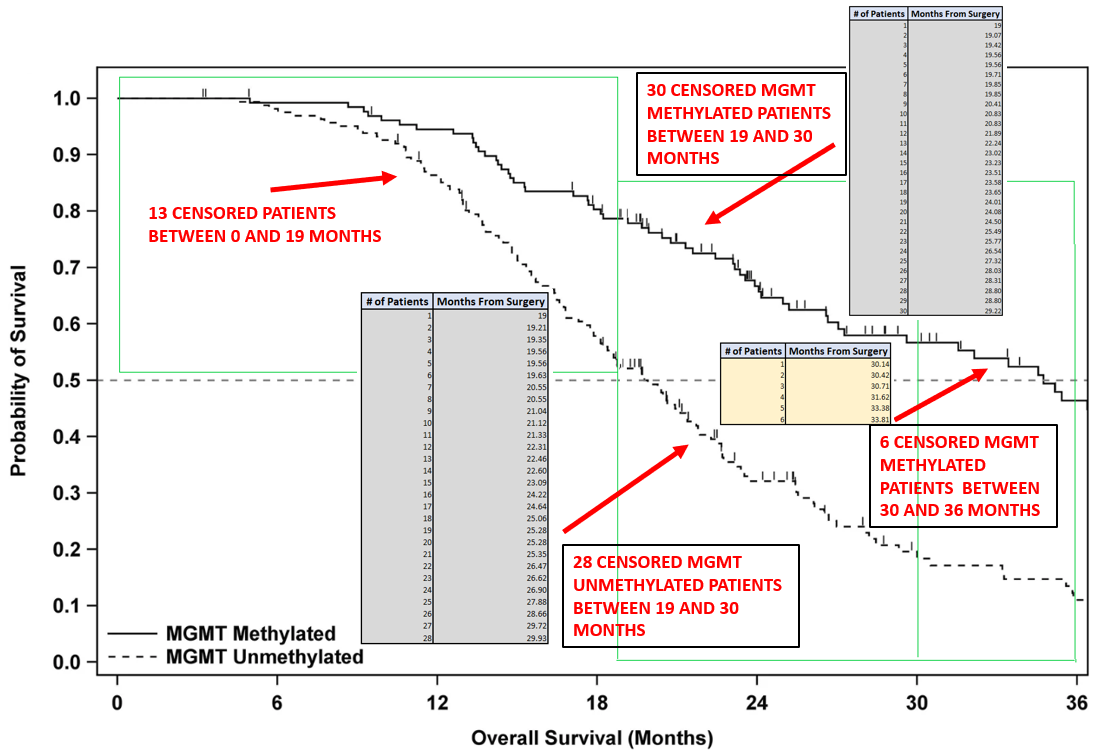
From the Figure below taken from the JTM publication we can count 13 censored patients between 0 and 19 months from surgery.
b. Why am I saying that these 13 patients were left censored (lost to follow)?
At the time of the JTM interim analysis all patients in the trial had 19 months or more from surgery. This can be seen in the timeline below.
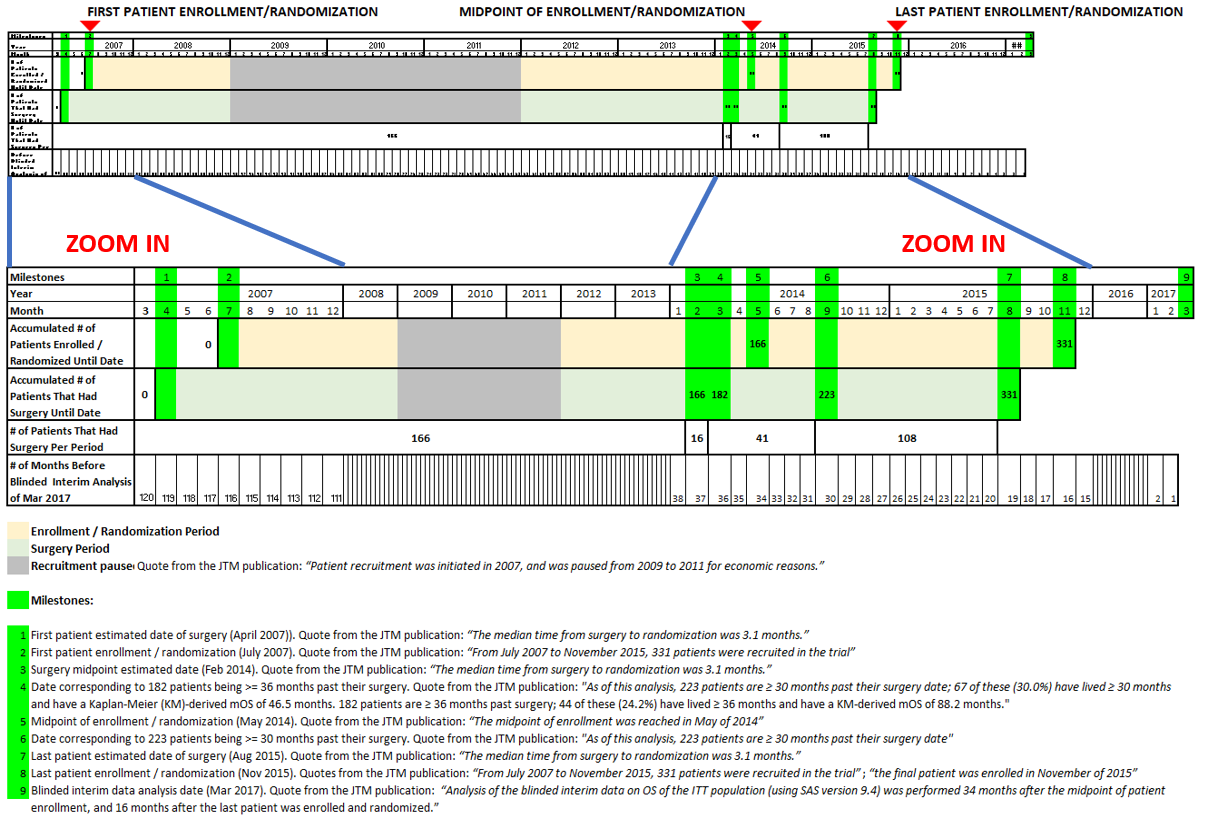
With this in mind and the definitions above for right and left censored patients, we can conclude that for the range of time between 0 and 19 months from surgery, all the censored patients in the interim analysis were left censored (lost to follow). There’s no way we can have a right censored patient in that time period because all patients had 19 or more months in the trial at that time.
c. Why am I saying that in the nGBM DCVax-L arm of the final results there were no censored patients included at least for the first 19 months, as opposed to the external control arms, where censored patients were included?
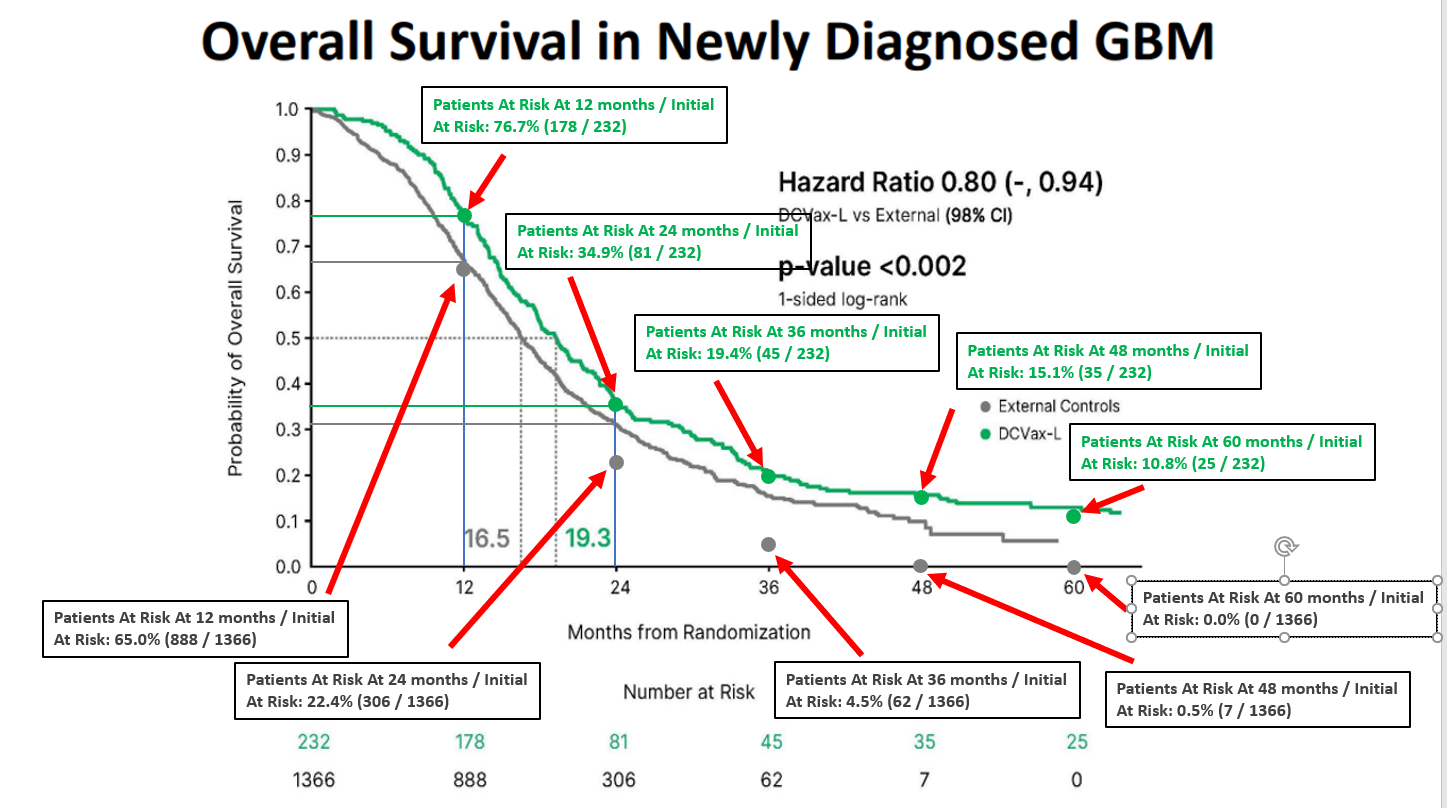
If we look at the following figure taken from slide 29 of 48 of final results
Together with the following Table I prepared
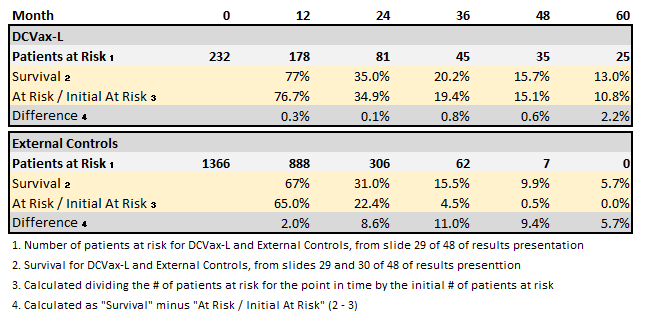
We can note that for the DCVaxL treatment arm the values for “Survival” and “At Risk / Initial At Risk” are the same for 12 (77% vs. 76.7%) and 24 (35.0% vs. 34.9%) months. The small differences (0.3% and 0.1%) correspond to the fact that the “Survival” values were read directly from the chart. This means that there were zero patients censored for the first 24 months in the DCVax-L arm. And because of this, there were zero censored patients for the first 19 months.
For the External Controls arm, on the other hand, the values for “Survival” and “At Risk / Initial At Risk” are different for 12 (67.0% vs. 65.0%) and 24 (31.0% vs. 22.4%) months. The differences are considerable (2.0% and 8.6%). This means that there were patients censored for the first 24 months in the DCVa-L arm. And because of this, there were censored patients for the first 19 months.
Some said there were mistakes in the charts or numbers at risk presented, but that is not true, there are no mistakes. The differences between “Survival” and “At Risk / Initial At Risk” are the effect of censored patients.
d. Why am I saying that censored patients help to get better survival results?
Below is an example of a hypothetical trial in which in in one case the censors were included to calculate the mOS and in the other they were not included. What can be seen is that in the one with censors the mOS is 10 months and in the one without it is 8. This is just an example, but anyone can look for literature to expand on this if wanted.
With this in mind it’s really positive that even taking out its left censored (lost to follow) patients for at least the first 19 months, DCVax-L treatment arm showed statistically significant benefits vs. external control arms where censored patients were not taken out.
Anybody else think the early vanguard group is the one that primarily makes up the 24 unidentified mgmt in the noncrossover group?
The MGMT gene promoter was methylated in 39.6% of patients (n=131) and unmethylated in 48.9% (n=162), with information not available for 11.5% (n=38; the missing data relates to the early patients enrolled a decade ago)
What Ex is saying:
No, it shows 25 actually lived 5 years. That is only 10.8%. To get to 13% they estimated the survival of the LTFU's, many who had been on study only a year or so before being lost.
they estimated the survival of the LTFU's
I first misunderstood your question.
I'm also trying to understand why. The only thing I can say about that for now is:
- I found the following statemet in the JTM article:
The MGMT gene promoter was methylated in 39.6% of patients (n=131) and unmethylated in 48.9% (n=162), with information not available for 11.5% (n=38; the missing data relates to the early patients enrolled a decade ago)
Thanks a lot BSB. I'm interested. Just saw your post now, don't know if you already had the meeting.
PUTTING TO REST THE LIES SPREAD ABOUT NWBO PHASE III TRIAL - PART 4
Ex, thanks for challenging my post. I'm sure that was not you motive, but thank you anyway, because to answer your post I did another analysis that helped me to be even more bullish. And the must important part, to understand one of the possible reasons why some are thinking results were negative when they were positive. And this is because the situation with the group of 35 non crossovers and 64 rGBM treatment arm can be counter intuitive and some take advantage of that to spread FUD and scare shareholders.
About your first point:
"2" is the number that fixes your math. Why only 2? Why not 5? Why not 10?


The core argument fails worse though. You have 99 patients that lived longer than the 232 treatment patients (per LL at SNO 2018). You can take subsets and slices all you want. The 99 did not change.


Actually, the number of IDH mutations was, I think, seven patients out of 331, which is lower than what you saw in the comparator groups
As follows:
- The nGBM arm has 4.7% ( 11 / 232 ) MGMT unidentified
- The rGBM arm has 4.7% ( 3 / 64 ) MGMT unidentified
- The small group of non crossover has 63% ( 22 / 35 ) MGMT unidentified
So the total unidentified is 36 ( 11+3+22 ), corresponding to 11% ( 36 / 331) of the ITT population.
Information comes from the following tables:
FINAL RESULTS NEWLY DIAGNOSED GBM PATIENTS

FINAL RESULTS RECURRENT GBM PATIENTS

FINAL RESULTS - NON CROSSOVER PATIENTS

More details on the calcualtions are on the origial post:
https://investorshub.advfn.com/boards/read_msg.aspx?message_id=168899638
I wasn't going to answer anymore, but thought it over and just don't want to leave it like this. In your reply to my post you wrote:
Your post is simply speculation.
What I think this shows is that most of the 24 unidentified mgmt amongst the non-crossovers probably came from early in the trial, before satisfactory mgmt methylation tests were developed. 2008
Thanks a lot hoffmann6383 for your words about this and my previous posts. Also for the great contribution you give to this board. I hope detailed information comes out as soon as possible and we get the journal publication finally. Great having you here.
No, you didn't. Incredible you say no supporting data, when is all around the post. And you don't even have any of that. But I don't mind what you think, will not answer you anymore and will wait to see the data to get conclusions about my analysis being right or wrong. And by the way I didn't say they were all methylated, I said most of them if not all and I think there will be some unmethylated but a minimal amount.
You are the one speculating here. Go ahead and refute my numbers with numbers and facts as the facts and calculations I included in my post. Did you even read the whole post and followed the calculations and sources to say this is speculation? I respect you and your analyses, but you are not the only one that can support this board and cannot come and make this kind of claims without the required support.
If we compare the results with the latest data that you mention, the conclusion of my post doesn´t change:
And the reason for this is actually good news because this can be explained as follows. At the beginning, the treatment arm started to do better because of DCVaxL, then as progression and pseudo progression (confounding factor) started, patients were taken out of the treatment arm and of the “placebo arm” to start going into the recurrent GBM treatment arm. So the already dead patients started to have higher effect in the treatment arm because there were less patients at risk. Also, important to take into account when analyzing this effect that recurrent GBM treatment arm is measured from recurrence, not from randomization or surgery. Then, after that, with the long term positive effect of DCVax, which is higher for patients that started earlier with the treatment, the treatment arm patients continued doing better and not only counteracted the effect mentioned of having less at risk (that is just a mathematical effect), but also continued doing better and better than what was shown in the interim blended blinded results.
I will accept your 26% read of the NYAS K/M over my 25% (old man eyes here). But that still leaves the 99 patient arm at 33.3% [28.2+2.2*232/99]. That is a decent improvement over 26%.
PUTTING TO REST THE LIES SPREAD ABOUT NWBO PHASE III TRIAL - PART 3
Here is another analysis that makes me even happier and convinced of the success of NWBO Phase III Trial, that I want to share with you. This is part of the analyses developed to put to rest the lies spread about NWBO Phase 3 Trial, saying first that the results were going to be bad or not reported, that the delays were associated with bad results and then saying that the trail failed, that the “placebo” arm did better than the treatment arm and that interim results were better than the final.
As mentioned, none of this is true and actually the trial was a success as predicted.
Let me start with the following two tables I prepared based on the final results presentation just shared by the company. One is for Newly Diagnosed GBM Patients and the other for Recurrent GBM Patients
TABLE 1 - FINAL RESULTS NEWLY DIAGNOSED GBM PATIENTS
1. From slide 29 of 48 (Overall Survival in Newly Diagnosed GBM ). Total patients shown at the left bottom
2. From slide 36 of 48 (Newly Diagnosed GBM: MGMT Methylated). Total patients shown at the left bottom
3. From slide 37 of 48 (Newly Diagnosed GBM: MGMT Unmethylated). Total patients shown at the left bottom
4. Calculated as follows: 1 – 2 - 3 (232 minus 90 minus 131)
TABLE 2 - FINAL RESULTS RECURRENT GBM PATIENTS
1. From slide 39 of 48 (Overall Survival in Recurrent GBM) Total patients shown at the left bottom
2. Calculated from the numbers highlighted in yellow in the final row of the Figure below, taken from slide 21 of 48 (External Controls for rGBM – Patient Demographics and Prognostic Factors). These numbers are the percentages of Methylated (44%), Unmethylated (52%) and Missing (5%), adjusted for rounding and multiplied by 64, that is the total recurrent GBM patients (number 1 above).

Now, let’s continue with the following Table with the number of patients and percentages of Methylated, Unmethylated and Missing from the JTM publication:
TABLE 3 - INTERIM BLINDED BLENDED ANALYSIS - ALL PATIENTS

Finally, with all this information we obtain the following Table for the patients that never crossed over, so never received DCVax L:
TABLE 4 - FINAL RESULTS - NON CROSSOVER PATIENTS

1. Obtained as follows: MGMT Methylated from Table 3 (INTERIM BLINDED BLENDED ANALYSIS - ALL PATIENTS) minus MGMT Methylated from Table 1 (FINAL RESULTS NEWLY DIAGNOSED GBM PATIENTS) minus MGMT Methylated from Table 2 (FINAL RESULTS RECURRENT GBM PATIENTS). 131 – 90 – 28 = 13
2. Obtained as follows: MGMT Unmethylated from Table 3 (INTERIM BLINDED BLENDED ANALYSIS - ALL PATIENTS) minus MGMT Unmethylated from Table 1 (FINAL RESULTS NEWLY DIAGNOSED GBM PATIENTS) minus MGMT Unmethylated from Table 2 (FINAL RESULTS RECURRENT GBM PATIENTS). 162 – 131 – 33 = -2
3. Obtained as follows: Unknown MGMT from Table 3 (INTERIM BLINDED BLENDED ANALYSIS - ALL PATIENTS) minus Unknown MGMT from Table 1 (FINAL RESULTS NEWLY DIAGNOSED GBM PATIENTS) minus Unknown MGMT from Table 2 (FINAL RESULTS RECURRENT GBM PATIENTS). 38 – 11 – 3 = 24
4. Obtained as follows: Total from Table 3 (INTERIM BLINDED BLENDED ANALYSIS - ALL PATIENTS) minus Total from Table 1 (FINAL RESULTS NEWLY DIAGNOSED GBM PATIENTS) minus Total from Table 2 (FINAL RESULTS RECURRENT GBM PATIENTS). 331 – 232 – 64 = 35. As a confirmation for calculations, this same number is obtained by adding the numbers above: 13 – 2 + 24 = 35.
But don’t worry about the -2 MGMT Unmethylated obtained. This detail can be fixed as follows. From TABLE 3 - INTERIM BLINDED BLENDED ANALYSIS - ALL PATIENTS if we substract 2 patients from the unknown MGMT and add them to the MGM Unmethylated, the percentage of distribution between MGMT Methylated, MGMT UnMethylated and Unknown continue to be very similar to the ones in the 2018 JTM publication and perfectly 2 patients MGMT status could have been identified after 2018 publication.
With this, we obtain the table bellow:
TABLE 5 - INTERIM BLINDED BLENDED ANALYSIS - ALL PATIENTS - UPDATED

And using the same formulas above and the updated values in Table 5, we obtain the following values:
TABLE 6 - FINAL RESULTS - NON CROSSOVER PATIENTS - UPDATED
So here is the conclusion of all this analysis that I consider is huge for the success of the trial:
All of the patients with known MGMT gene promoter methylation status in the group of these 35 patients that never crossed over are MGMT methylated and that explains why these patients did better. This also expains why they are not comparable to the treatment arms for newly diagnosed and recurrent GBM. Out of the patients with still unknown MGMT gene promoter methylation status, almost all if not all are MGMT Methylated. With any kind of correct math we do, for more patients with unknow MGMT gene promoter methylation status that may have been identified after 2018 JTM publication, the conclusion is the same.
Sources:
JTM publication
https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-018-1507-6
Final results presentation
https://virtualtrials.org/dcvax/dcvax.pdf
Disclosures:
English is not my native language, so sorry if you find mistakes in wording or redaction. This is not investment advice, I am sharing my analysis and opinion based on public information.
I think it's time to put to rest all the lies that have been spread, saying that the trail failed, that the “placebo” arm did better than the treatment arm and that interim results were better than the final. None of this is true and actually the trial was a success as predicted.
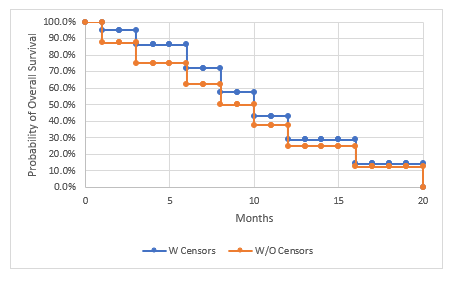
Based on the final results presentation shared this week by the company (https://virtualtrials.org/dcvax/dcvax.pdf) I prepared the following chart. In order to compare the final treatment arm results with the interim blended blinded data reported in 2018, the survival points for 12, 24, 36 and 46.5 months from surgery were located in this chart. These points were located at 8.9 (12 minus 3.1) months, 20.9 (24 minus 3.1) months, 32.9 (36 minus 3.1) months and 43.4 (46.5 minus 3.1) months because the 2018 interim blended results were measured from surgery, the final results were measured from randomization and the average time difference between surgery and randomization was 3.1 months.

The following table contains a comparison between the final results of the treatment arm for the newly diagnosed GBM (shown in the chart above) and the 2018 interim blended blinded results shared by the company:

* From:
- JTM interim results publication. https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-018-1507-6
- Press Release November 19, 2018 https://nwbio.com/updated-interim-data-from-phase-3-trial-of-dcvax-l-for-glioblastoma/
** Calculated from JTM interim results publication:
https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-018-1507-6
As of this analysis, 223 patients are>=30 months past their surgery date; 67 of these (30.0%) have lived>=30 months and have a Kaplan-Meier (KM)-derived mOS of 46.5 months.
dmb2, the main reason is that in the 2018 publication the 3 years were counted from surgery and in this presentation of final results the 3 years were counted from randomization / enrollment. You need to compare the data point at 36 months from 2018 publication with the data point at 33 months from this presentation, because the average time of enrollment / randomization after surgery was 3.1 months.
Totally agree Doc Logic. And I think we finally are very close to success.
Also, I always remember your comments about the last patients enrolled in the trial that were included in the treatment arm in a higher proportion than before or something like that. I would like to ask you to please let me know why is that you concluded that, because from an analysis I did, I think that the last patients in the trial did much better than the ones before, as I explain in the following link. And what you concluded would make the situation even better. Not sure if you saw it.
https://investorshub.advfn.com/boards/read_msg.aspx?message_id=168777187
Please let me know Doc.
Ex, let me make this clear for you, so you can see there are no serious math issues here, maybe some serious understanding issues in the post I'm replying to.
There are two types of censored patients:
- Left censored: Patients that were lost to follow at the time of the analysis.
- Right censored: Patients that were in the trial and alive at the time of the analysis (we don't know how long they are going to live).
Also, you need to remember that not all the patients entered the study at the same time, so at the time of the interim analysis, there were patients all the way between 19 and 120 months (10 years) from surgery, as can be seen in the following timeline I prepared:
With this in mind, we can state the following:
- For the range between 0 and 19 months from surgery, all the censored patients are left censored (lost to follow). This is true because at the time of the interim analysis all patients had 19 months or more from surgery. So, if we look at the definition above, there is no way a right censored patient would appear in that range.
- For the range between 19 and 36 months from surgery all the censored patients were right censored, meaning they were alive. This is because, even though there can be found right and left censored patients in that range of time, the number of 64 patients alive calculated in my pervious post (link below) is exactly the same number of 64 censors counted on the chart below. Each censor is a small vertical line located at the time the patient that was still alive had from surgery when the interim analysis was done. This also makes sense because is much more probable to find left censored patients (lost to follow) towards the beginning of the trial (first enrolled patients).
https://investorshub.advfn.com/boards/read_msg.aspx?message_id=168777187
Also from all this analysis, all the patients that were alive and in the trial at the time of the interim analysis and were past 36 months from surgery (first patients enrolled) are not part of the censored patients
Based on the exact same math, your sentence:
the number alive at 36 months was 64( 64--0). And the number alive at 19 months was 0 (64-64).
Now that it looks like we finally are going to see the trial results very soon, I want to share an analysis that for me, added to other analyses shared here by many posters and my own due diligence, makes this trial definitively a success.
Disclosures: English is not my native language, so sorry if you find mistakes in wording or redaction. This is not investment advice, I am sharing my analysis and opinion based on public information.
1. First of all, based on the 2018 JTM publication with the interim trial analysis, I prepared the following timeline:
Link to JTM publication:
https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-018-1507-6#Fig1
To start, it is important to emphasize the imbalance between the number of patients enrolled towards the beginning of the trial vs. the number enrolled towards the end. In the top of the chart you can see that 50% of the patients were enrolled from July 2007 to May 2014 (almost 7 years) and the last 50%, from May 2014 to November 2015 (just last one year and a half).
2. The last 50% of patients in the trial did much better than the first 50% and this is going to result in much better final trial results as compared to the 2017 interim analysis published in 2018. Why did I come to that conclusion?
From the JTM publication we know that at the time of the analysis, 182 patients were>=36 months past their surgery date and 44 of these (24.2%) have lived>=36 months (see comment corresponding to milestone number 4 of the timeline above). Also, the intent to treat population is composed of 331 patients. This means that 149 (331 – 182) patients were<36 months past their surgery.
Also, from the JTM publication, “At the time of this analysis, 108 [of] the 331 patients (32.6%) were still alive.” If we put this statement and the previous together, 64 (108 – 44) of the patients that were <36 months past their surgery were still alive. So 43.0% ( 64 / 149 ) of the last 149 patients of the trial that were < 36 months past surgery were alive.
3. As shown in the chart above, the last 149 patients mentioned were between 19 and 36 months from surgery at the time of the interim analysis and from the paragraph above, 64 of them were alive. If we count the number of censored patients between these 19 and 36 months looking at the overall survival curves in the JTM publication, we obtain exactly the same 64, composed of:
+ 30 MGMT Methylated between 19 and 30 months
+ 28 MGMT Unmethylated between 19 and 30 months
+ 6 MGMT Methylated between 30 and 36 months
The detail is shown in the Figure below (the count was done using the chart that separates MGMT Methylated and Unmethylated in the JTM publication because they were easier to count and locate).
With this number being the same 64 and knowing that the last patients 149 patients were between 19 and 36 months from surgery at the time of the analysis we can conclude that all of them were right censored, meaning that they were all alive at the time of the analysis.
4. From the chart above, it can be noted that there were 6 patients censored between 30 and 36 months. With this and what was explained above, we can conclude that from the last patients, the count of alive and already in the study at 30 months after surgery, was 6 less than at 36 months after surgery: 58 (64 – 6).
Also, from the JTM publication we know that at the time of the analysis, 223 patients were>=30 months past their surgery date and 67 of these (30.0%) have lived>=30 months (see comment for milestone number 4 of the timeline above). This means that 108 (331 – 223) patients were<30 months past their surgery. So 53.7% ( 58 / 108 ) of the last 108 patients of the trial that were < 36 months past surgery were alive.
In the chart below this data points are compared to the survival curve from the 2018 JTM publication

This is why I think last patients will do much better than the first ones and as a consequence of this, the final survival curve will move up and will end up being between were it was in the interim analysis and the curve obtained joining the points shown above for last patients.
5. Finally, to corroborate what I am mentioning, a few months after the interim analysis, the company published updated interim data in the press release linked above:
https://nwbio.com/updated-interim-data-from-phase-3-trial-of-dcvax-l-for-glioblastoma/
Below is a chart I prepared showing the comparison between the JTM publication curve and the updated interim data:

Here it can be seen that in just some months the curves start to separate to the upside in the area corresponding to 20 months after surgery. The curves can’t separate before 19 months, because at the time of the interim analysis the last patient had exactly 19 months from surgery, so the rest of the patients had more than that time.
With all that was mentioned we should expect further separation of the curves and the corresponding improvement of results. Finally, is very important to remember that this is still all related to blended blinded results, so treatment arm will be even better. And if what Doc logic have been mentioning, that the last patients were more loaded to the treatment arm, than before we can expect even more separation of the treatment curve and better results.
Reading comprehension issues?
Again, can you give me an example of a drug that was not approved after taking this long to get TLD out?
And again, can you give me an example of a drug that was not approved after taking this long to get TLD out? You haven't been able to find it.
Hahahaha. Good one. Al least you made me laugh. Time will tell. I think that one is going to be successful.
Can you give us one example of an unsuccessful trial that took 16+ months after data lock to release tld?
Excellent post biosectinvestor. Agree 100%.
Agree VikingInvest
No, they are not wrong, but for them (usually much bigger companies) there is not as important as it is for a small company like NWBO to have TLD together with the journal publication, so they can get the world to know them, get the word out to the doctors and RA’s and prevent malicious attacks. Also as mentioned by the company, waiting for the TLD announcement doesn’t affect the approval timeline. I think on the other hand, helps getting a faster approval, because of the priority given by the journals when the companies don’t start announcing partíal informaton vía press releases and others, as I shown in my previous post. The faster they have a pier reviewed journal publication, the faster the RA's will consider it for approval.
Thanks a lot Maverick0408 for you answer.
Poor Man, I think the reason is that recognized journals have restrictions about company use of media and press releases before publishing. If the company would have released TLD without taking this into account, publication may have not been approved or not prioritized by a prestigious journal.
I also strongly believe that trial outcome is positive, because otherwise the company would not be so interested in spending such amount of time and money in getting the journal publication and, on the other hand, they would be at risk of having legal consequences for not reporting earlier if results were bad.
Below are some extracts of the document Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals (updated December 2019) published by the International Committee of Medical Journal Editors (ICMJE) that support what I'm mentioning.
Link to the document mentioned: http://www.icmje.org/icmje-recommendations.pdf
Also take a look at the amount and prestigious names (NEJM and the Lancet among much others) of journals that follow ICMJE. They provide a list. Link to ICMJE webpage: http://www.icmje.org/
Quote:
2. Duplicate and Prior Publication
Duplicate publication is publication of a paper that overlaps substantially with one already published, without clear, visible reference to the previous publication. Prior publication may include release of information in the public domain.
Readers of medical journals deserve to be able to trust that what they are reading is original unless there is a clear statement that the author and editor are intentionally republishing an article (which might be considered for historic or landmark papers, for example). The bases of this position are international copyright laws, ethical conduct, and cost-effective use of resources. Duplicate publication of original research is particularly problematic because it can result in inadvertent double-counting of data or inappropriate weighting of the results of a single study, which distorts the available evidence.
When authors submit a manuscript reporting work that has already been reported in large part in a published article or is contained in or closely related to another paper that has been submitted or accepted for publication elsewhere, the letter of submission should clearly say so and the authors should provide copies of the related material to help the editor decide how to handle the submission. See also Section IV.B.
This recommendation does not prevent a journal from considering a complete report that follows publication of a preliminary report, such as a letter to the editor, a preprint, or an abstract or poster displayed at a scientific meeting. It also does not prevent journals from considering a paper that has been presented at a scientific meeting but was not published in full, or that is being considered for publication in proceedings or similar format. Press reports of scheduled meetings are not usually regarded as breaches of this rule, but they may be if additional data tables or figures enrich such reports. Authors should also consider how dissemination of their findings outside of scientific presentations at meetings may diminish the priority journal editors assign to their work.
Authors who choose to post their work on a preprint server should choose one that clearly identifies preprints as not peer-reviewed work and includes disclosures of authors’ relationships and activities. It is the author’s responsibility to inform a journal if the work has been previously posted on a preprint server. In addition, it is the author’s (and not the journal editors’) responsibility to ensure that preprints are amended to point readers to subsequent versions, including the final published article.
In the event of a public health emergency (as defined by public health officials), information with immediate implications for public health should be disseminated without concern that this will preclude subsequent consideration for publication in a journal. We encourage editors to give priority to authors who have made crucial data publicly available (e.g., in a gene bank) without delay.
Sharing with public media, government agencies, or manufacturers the scientific information described in a paper or a letter to the editor that has been accepted but not yet published violates the policies of many journals. Such reporting may be warranted when the paper or letter describes major therapeutic advances; reportable diseases; or public health hazards, such as serious adverse effects of drugs, vaccines, other biological products, medical devices. This reporting, whether in print or online, should not jeopardize publication, but should be discussed with and agreed upon by the editor in advance when possible.
The ICMJE will not consider as prior publication the posting of trial results in any registry that meets the criteria noted in Section III.L. if results are limited to a brief (500 word) structured abstract or tables (to include participants enrolled, key outcomes, and adverse events). The ICMJE encourages authors to include a statement with the registration that indicates that the results have not yet been published in a peer-reviewed journal, and to update the results registry with the full journal citation when the results are published.
Editors of different journals may together decide to simultaneously or jointly publish an article if they believe that doing so would be in the best interest of public health. However, the National Library of Medicine (NLM) indexes all such simultaneously published joint publications separately, so editors should include a statement making the simultaneous publication clear to readers.
Authors who attempt duplicate publication without such notification should expect at least prompt rejection of the submitted manuscript. If the editor was not aware of the violations and the article has already been published, then the article might warrant retraction with or without the author’s explanation or approval.
See COPE flowcharts for further guidance on handling duplicate publication.
Quote:
K. Journals and the Media
Journals’ interactions with media should balance competing priorities. The general public has a legitimate interest in all journal content and is entitled to important information within a reasonable amount of time, and editors have a responsibility to facilitate that. However media reports of scientific research before it has been peer-reviewed and fully vetted may lead to dissemination of inaccurate or premature conclusions, and doctors in practice need to have research reports available in full detail before they can advise patients about the reports’ conclusions.
An embargo system has been established in some countries and by some journals to assist this balance, and to prevent publication of stories in the general media before publication of the original research in the journal. For the media, the embargo creates a “level playing field,” which most reporters and writers appreciate since it minimizes the pressure on them to publish stories before competitors when they have not had time to prepare carefully. Consistency in the timing of public release of biomedical information is also important in minimizing economic chaos, since some articles contain information that has potential to influence financial markets. The ICMJE acknowledges criticisms of embargo systems as being selfserving of journals’ interests and an impediment to rapid dissemination of scientific information, but believe the benefits of the systems outweigh their harms.
The following principles apply equally to print and electronic publishing and may be useful to editors as they seek to establish policies on interactions with the media:
• Editors can foster the orderly transmission of medical information from researchers, through peer-reviewed journals, to the public. This can be accomplished by an agreement with authors that they will not publicize their work while their manuscript is under consideration or awaiting publication and an agreement with the media that they will not release stories before publication of the original research in the journal, in return for which the journal will cooperate with them in preparing accurate stories by issuing, for example, a press release.
• Editors need to keep in mind that an embargo system works on the honor system—no formal enforcement or policing mechanism exists. The decision of a significant number of media outlets or biomedical journals not to respect the embargo system would lead to its rapid dissolution.
• Notwithstanding authors’ belief in their work, very little medical research has such clear and urgently important clinical implications for the public’s health that the news must be released before full publication in a journal. When such exceptional circumstances occur, the appropriate authorities responsible for public health should decide whether to disseminate information to physicians and the media in advance and should be responsible for this decision. If the author and the appropriate authorities wish to have a manuscript considered by a particular journal, the editor should be consulted before any public release. If editors acknowledge the need for immediate release, they should waive their policies limiting prepublication publicity.
• Policies designed to limit prepublication publicity should not apply to accounts in the media of presentations at scientific meetings or to the abstracts from these meetings (see Duplicate Publication). Researchers who present their work at a scientific meeting should feel free to discuss their presentations with reporters but should be discouraged from offering more detail about their study than was presented in the talk, or should consider how giving such detail might diminish the priority journal editors assign to their work (see Duplicate Publication).
• When an article is close to being published, editors or journal staff should help the media prepare accurate reports by providing news releases, answering questions, supplying advance copies of the article, or referring reporters to appropriate experts. This assistance should be contingent on the media’s cooperation in timing the release of a story to coincide with publication of the article.
Maverick0408, I don't think LL alluded to this:
UK & EU accepted it last year. FDA has not been easy to convince one way or another and LL alluded to this last year
So here is the view from somebody that doesn't post too much, but follows this board and has been an NWBO investor for long time. From last 10Q:
On June 30, 2021, the Company entered into multiple four-month note agreements (the “Notes”) with various individual lenders (the “Holders”) with an aggregate principal amount of $1.9 million. The Notes contain a conditional piggy-back right to independently purchase shares from the Company, which provides a right for the Holders, contingent on the release of clinical trial data and a next private placement offering (“Next Offering”) after this release, to (a) purchase shares from the Company within seven days following such Next Offering at a 12% discount from the share price of the Next Offering for a variable number of shares equal to an amount up to 50% of the principal amount of the loan and (b) exchange some or all of the outstanding loan amount for a variable number of shares, within seven days after the Next Offering at a 12% discount, resulting in a reduced cash amount repayable under the loan agreement.
During July and August 2021, the Company entered into multiple four-month note agreements (the “Notes”) with various individual lenders (the “Holders”) with an aggregate principal amount of $0.97 million for net proceeds of $0.93 million. The Notes contain a conditional piggy-back right to independently purchase shares from the Company, which provides a right for the Holders, contingent on the release of clinical trial data and the next private placement offering (“Next Offering”) after this release, to (a) purchase shares from the Company within seven days following such Next Offering at a 12% discount from the share price of the Next Offering for a variable number of shares equal to an amount up to 50% of the principal amount of the loan and (b) exchange some or all of the outstanding loan amount for a variable number of shares, within seven days after the Next Offering at a 12% discount, resulting in a reduced cash amount repayable under the loan agreement.
I admit I sold part of my holdings Today at a loss after I saw what I shared in my previous post, but I also tell you that I'm sure I'm not responsible for the drop. The number of shares I sold is not even comparable to the volume Today and share price was already dropping when I sold. I just sold because I was anxious about keeping all my shares, but still keep part of them.
For the ones that are wondering why this price crash is happening after the supposed "good news", as a victim of his new lies I can tell you that I just realized with the OS update in the OTC Markets site that Anshu diluted 1 million more shares in 10 days, just after the pumping news, while in the other hand he was lying to us, telling us that he was paying debt and avoiding dilution. Also together with the 10Q, an amount of $709,250 of additional new notes was filed.
I'm not trying to be negative, I was burned hard with his other company and that is why I am looking very close here for my investment. Anshu doesn't have limits to his lying.
Link to the 10Q that has the new notes filing at the end:
https://www.otcmarkets.com/filing/conv_pdf?id=14729962&guid=j2daUWaAZZWSw3h
Comparison of Outstanding shares as of Feb 15 (reported with the 10Q) vs. Outstanding shares updated in OTC markets, as of last Friday (Feb 26, 2021). 1 million shares in 10 days while Anshu was stating the opposite. Facts don't lie:


Agreed Cdub3, I'll try to recover something and fly away.
Agree 100% Crozz. As usual, what an excellent post from you!!!
Something I don't know is if he is going to change his warrants for free shares as he did in his other company, instead of paying $18.5 million, as per the legal agreements (0.5 exercise price times 37 million warrants). He approved it for himself because he alone is the Board of Directors. Very dishonest and unethical by the way. He tried to make it look like as it was for the benefit of the company and shareholders as you can see below. He is definitely a shameless liar.
For VRUS the exercise price post RS is $3 per share (0.006 X 500). Let's see if he is going to do the same or not RS his shares or if he finally is going to be honest.
Here in VRUS he is in the same process of converting the Board of Directors.

https://www.otcmarkets.com/filing/html?id=14277338&guid=lZbKUq2e-NCnp3h

