










Friday, May 06, 2022 1:51:30 PM
Disclosures: English is not my native language, so sorry if you find mistakes in wording or redaction. This is not investment advice, I am sharing my analysis and opinion based on public information.
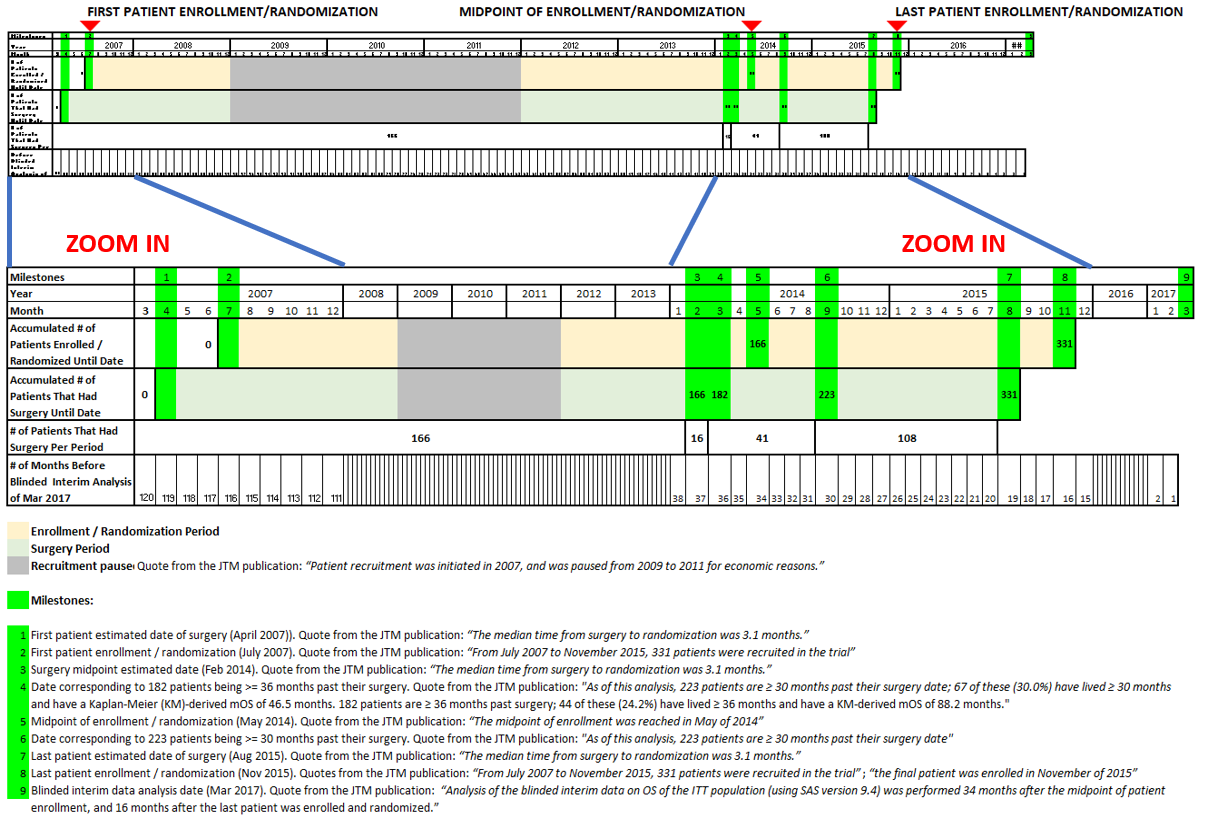
1. First of all, based on the 2018 JTM publication with the interim trial analysis, I prepared the following timeline:
Link to JTM publication:
https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-018-1507-6#Fig1
To start, it is important to emphasize the imbalance between the number of patients enrolled towards the beginning of the trial vs. the number enrolled towards the end. In the top of the chart you can see that 50% of the patients were enrolled from July 2007 to May 2014 (almost 7 years) and the last 50%, from May 2014 to November 2015 (just last one year and a half).
2. The last 50% of patients in the trial did much better than the first 50% and this is going to result in much better final trial results as compared to the 2017 interim analysis published in 2018. Why did I come to that conclusion?
From the JTM publication we know that at the time of the analysis, 182 patients were>=36 months past their surgery date and 44 of these (24.2%) have lived>=36 months (see comment corresponding to milestone number 4 of the timeline above). Also, the intent to treat population is composed of 331 patients. This means that 149 (331 – 182) patients were<36 months past their surgery.
Also, from the JTM publication, “At the time of this analysis, 108 [of] the 331 patients (32.6%) were still alive.” If we put this statement and the previous together, 64 (108 – 44) of the patients that were <36 months past their surgery were still alive. So 43.0% ( 64 / 149 ) of the last 149 patients of the trial that were < 36 months past surgery were alive.
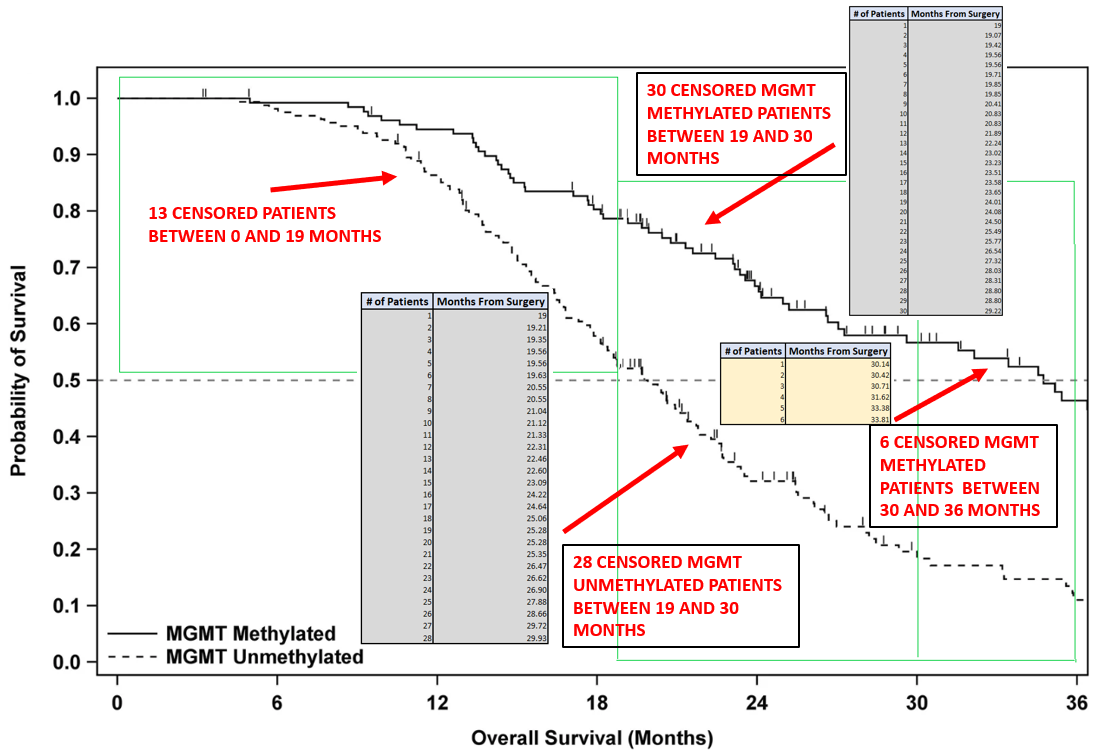
3. As shown in the chart above, the last 149 patients mentioned were between 19 and 36 months from surgery at the time of the interim analysis and from the paragraph above, 64 of them were alive. If we count the number of censored patients between these 19 and 36 months looking at the overall survival curves in the JTM publication, we obtain exactly the same 64, composed of:
+ 30 MGMT Methylated between 19 and 30 months
+ 28 MGMT Unmethylated between 19 and 30 months
+ 6 MGMT Methylated between 30 and 36 months
The detail is shown in the Figure below (the count was done using the chart that separates MGMT Methylated and Unmethylated in the JTM publication because they were easier to count and locate).
With this number being the same 64 and knowing that the last patients 149 patients were between 19 and 36 months from surgery at the time of the analysis we can conclude that all of them were right censored, meaning that they were all alive at the time of the analysis.
4. From the chart above, it can be noted that there were 6 patients censored between 30 and 36 months. With this and what was explained above, we can conclude that from the last patients, the count of alive and already in the study at 30 months after surgery, was 6 less than at 36 months after surgery: 58 (64 – 6).
Also, from the JTM publication we know that at the time of the analysis, 223 patients were>=30 months past their surgery date and 67 of these (30.0%) have lived>=30 months (see comment for milestone number 4 of the timeline above). This means that 108 (331 – 223) patients were<30 months past their surgery. So 53.7% ( 58 / 108 ) of the last 108 patients of the trial that were < 36 months past surgery were alive.
In the chart below this data points are compared to the survival curve from the 2018 JTM publication

This is why I think last patients will do much better than the first ones and as a consequence of this, the final survival curve will move up and will end up being between were it was in the interim analysis and the curve obtained joining the points shown above for last patients.
5. Finally, to corroborate what I am mentioning, a few months after the interim analysis, the company published updated interim data in the press release linked above:
https://nwbio.com/updated-interim-data-from-phase-3-trial-of-dcvax-l-for-glioblastoma/
Below is a chart I prepared showing the comparison between the JTM publication curve and the updated interim data:

Here it can be seen that in just some months the curves start to separate to the upside in the area corresponding to 20 months after surgery. The curves can’t separate before 19 months, because at the time of the interim analysis the last patient had exactly 19 months from surgery, so the rest of the patients had more than that time.
With all that was mentioned we should expect further separation of the curves and the corresponding improvement of results. Finally, is very important to remember that this is still all related to blended blinded results, so treatment arm will be even better. And if what Doc logic have been mentioning, that the last patients were more loaded to the treatment arm, than before we can expect even more separation of the treatment curve and better results.
Recent NWBO News
- Biophma Announces Exclusive In License for Dendritic Cell Technology, Sending Shares Higher • AllPennyStocks.com • 06/17/2024 04:40:00 PM
- Form 8-K - Current report • Edgar (US Regulatory) • 06/04/2024 09:11:16 PM
- Form DEF 14A - Other definitive proxy statements • Edgar (US Regulatory) • 06/03/2024 09:22:55 PM
- Form PRE 14A - Other preliminary proxy statements • Edgar (US Regulatory) • 05/22/2024 08:13:36 PM
- Form 10-Q - Quarterly report [Sections 13 or 15(d)] • Edgar (US Regulatory) • 05/10/2024 09:04:57 PM
- Form NT 10-K - Notification of inability to timely file Form 10-K 405, 10-K, 10-KSB 405, 10-KSB, 10-KT, or 10-KT405 • Edgar (US Regulatory) • 03/01/2024 10:04:38 PM
- Form 4 - Statement of changes in beneficial ownership of securities • Edgar (US Regulatory) • 12/02/2023 01:31:35 AM
- Form 8-K - Current report • Edgar (US Regulatory) • 11/16/2023 10:11:54 PM
- Epazz, Inc. (OTC Pink: EPAZ) ZenaDrone Demonstration to Defense Departments of UAE and Saudi Arabia • InvestorsHub NewsWire • 11/15/2023 12:19:31 PM
- Form 10-Q - Quarterly report [Sections 13 or 15(d)] • Edgar (US Regulatory) • 11/09/2023 09:30:39 PM
- Epazz, Inc. (OTC Pink: EPAZ) US Navy Collaboration ZenaDrone 1000 • InvestorsHub NewsWire • 11/09/2023 01:00:34 PM
- Epazz, Inc. (OTC Pink: EPAZ) US Navy Collaboration ZenaDrone 1000 Extreme Weather Demo • InvestorsHub NewsWire • 11/07/2023 12:29:43 PM
- Form 10-Q - Quarterly report [Sections 13 or 15(d)] • Edgar (US Regulatory) • 08/09/2023 08:36:14 PM
Glidelogic Corp. Becomes TikTok Shop Partner, Opening a New Chapter in E-commerce Services • GDLG • Jul 5, 2024 7:09 AM
Freedom Holdings Corporate Update; Announces Management Has Signed Letter of Intent • FHLD • Jul 3, 2024 9:00 AM
EWRC's 21 Moves Gaming Studios Moves to SONY Pictures Studios and Green Lights Development of a Third Upcoming Game • EWRC • Jul 2, 2024 8:00 AM
BNCM and DELEX Healthcare Group Announce Strategic Merger to Drive Expansion and Growth • BNCM • Jul 2, 2024 7:19 AM
NUBURU Announces Upcoming TV Interview Featuring CEO Brian Knaley on Fox Business, Bloomberg TV, and Newsmax TV as Sponsored Programming • BURU • Jul 1, 2024 1:57 PM
Mass Megawatts Announces $220,500 Debt Cancellation Agreement to Improve Financing and Sales of a New Product to be Announced on July 11 • MMMW • Jun 28, 2024 7:30 AM

