 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.


Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
No what I’m saying at all DD
He gave multiple impressive historical examples showing the opposite.
My first purchase of $nwbo was at $.18 it that that mark today. Memories.
Wrong. Most stocks walk up before a catalyst as investors know something is coming. It is just the junk stocks that you buy that go lower and you justify it with an excuse 🤷🏼♂️
That goes against "buy the rumor, sell the news" theory
He would argue, that showed the logical oppositional corollary.
The market has not tanked for NWBO because of canceling ASCO come on.
" but BasinStreetBlues (is he posting here still?) often reminded us of pps dips before massive events. "
SP went to 2.00$ just before TLD release.
"Ohhh, I see... so bashing management equates to supporting the science!!!???"
no, bashing mngmt equates to frustration SP is at .20
Not selling equates to supporting science
I'm just glad it didn't get announced today in this bloodbath. Be great to see a recovery day w announcement
Aggressive short-sellers often intentionally drive the price down before a major catalyst.
They create artificial downward pressure to induce panic selling, depress market sentiment, and gain favorable cover prices.The tactic is to “shake the tree” before the fruit drops.
Just before positive news or a potential breakout, these players exploit low liquidity and investor anxiety to accumulate or cover positions silently.
Approval next week then!!
Im all for it!!
Posted on: NorthWest Biotherapeutics Inc
learningcurve2020
RE: learningcurve2020 Post # 758635
04/02/2025 08:15 PM
Post
# of 759048
…Or maybe you just consider me “Not invested” because management lost the last decade’s retail shareholders all their investment?
Posted on: NorthWest Biotherapeutics Inc
learningcurve2020
RE: LTR Post # 758629
04/02/2025 07:59 PM
Post
# of 759048
How do you know I’m not invested? This is a narrative the disciples have been pushing here since the beginning even as I constantly fight for legacy shareholders.
Toucan will scoop up NWBO for nothing
In other words the market is down 30% since the last 10K because it didn't like the immense burden of cost and investment obligation NWBO has taken upon its self without cash in the bank and low market cap to carry that. The market didn't like that one bit, And for no other reason and again I agree with the market on that one.
I do however worry that if we are heading into a global fiscal crisis.
a country like the UK which already suffers from economic problems
Make it simple friend... you can control your concerns or worries. ... Think about yourself.
Toucan will scoop up NWBO for nothing and keep all the patents which is perhaps LP's plan all along
I missed that, link?
When the trial began, the cross over was mandated,
Investor082,
Sure looking like this was all set up to have an artisan start but Flaskworks in range. For an artisan start the money from set asides must be READILY available and sufficient self pay interest to get rolling or the economic model won’t work. The demand is already in place. It’s the supply end that has always needed the most attention and supply takes readily available funding that creates steady and reliable cash flow. That part is on the U.K. if they want to lead. Artisan has been ready for quite some time. UCLA, Cognate (now Charles River Labs) and Advent have been making L for going on 3 decades and MHRA can’t approve? Give me a break! Has to be a timing issue related to U.K. economics or artisan approval should have been in hand by now because safety is of almost no concern at all. Even U.K. politicians are griping about a lack of movement by MHRA and NHS with regard to cell therapy and other treatments for GBM. Best wishes.
The more probable reality is that they are focused very little on the MAA. They are way more focused on other products, years from commercialization, and that is troubling.
One alternative, which I neither subscribe to nor dismiss: DennisDave and maybe a couple others were convinced about the time frame of six to eight weeks after last inspection. If the last relevant inspection was on a Friday (January 31), and let’s say Monday February 3 started that last sprint, that would place an eight week decision sometime possibly right after the supposed blase’ 10K, which came out four days ago. (It would place a six week decision from February 20, 2025 about yesterday)
I’m not saying they are right, but BasinStreetBlues (is he posting here still?) often reminded us of pps dips before massive events. Not necessarily based on rumor, but perhaps sometimes based on better due diligence and head fakes to cover and scoop.
Anyway, there is a gap between decisions and announcements to align messaging. (The gap is not supposed to be too long, according to people like the SEC, to prevent untoward leaks.)
Thus we returned to the age old bottom gap today, a Friday, an hour after opening bell, perhaps just due diligence described above to cover and/or scoop. Showing how clever some traders are, or are not, I guess.
Just an alternative hypothesis.
Flip, I've always enjoy your post. However, why do you keep defending yourself with these clowns? Let them dig their own grave.
Me also
It is so attractive at 17 cents by may have to risk her wrath
Now find A post that says that I actually sold share for profit . So unless u do nt know there are very few ways of realizing gains
Agree it may not be a rejection, but maybe there are unanswered question from the regulator/inspectors. W-T-F else could it be.?
Typo should be 20 k.
If January 31 was pragmatically the end of the relevant MAA
inspections, we have been waiting since then more than 2 months for the
MAA decision. This seems to me to be a super long time.
I welcome any logical explanations with the emphasis on logical
because I don't believe for a minute that the delay signals an MHRA
rejection of the MAA.
It's laughable that all the paid bashers accuse longs of being paid pumpers ..
Longs naturally want the stock price to go higher ..
But the unusually large contingent who comes here daily to create false innuendos and outright bash management .. you guys need to find a new purpose in life .. crazy that all u uninvested BASHERS care so much about OUR INVESTMENTS ..
I could buy about 20000k at this such a blessing in disguise time every month.
This would make a great Dos Equis commercial!
But again, my thesis has truly changed here. I would have happily recommended anyone I chatted with to buy NWBO up until that 10K. No chance in hell I'd recommend NWBO now. The pumpers don't realize just how bad it was. The market does.
sukus, you still have money to buy? I am impressed!
Perhaps an algorithm created the gap so that it could be revisited at a later date?
I just bought more less than a minute ago @ .2007.
Well, we learned recently that LC is invested. Which other “bears” are invested?
Link doesn’t work.
well, maybe investors believe in the science and also want to support a company fighting cancer.
They are buying too Chiugray in such an opportune time. They are the smartest. But I don’t want to be outsmarted by them.
And speaking of charts.
Pull up a one year chart of the S&P 500.
Bleeding orange.
Did it ever cross your mind that DD trades?
But how can that be?
Danish Dude "proved" that the cert was for Eden.
Why should I believe your completely rational explanation vs DDs proof that they approved Eden devices that they have not yet even been ordered?
We were all LIED TO by the stinking POS linda grifter.
NWBO might beat my 720-day decision! This old management needs to retire. Absolute ignorant people who doesn't even know how to operate a damn cellphone.
Thank you. Which makes me wonder if January 31 wasn’t pragmatically the end of relevant MAA inspections.
AngeloFoca - Bingo. I think your post is one of the best I've heard here in years. Should be required reading for newbies.
So, if management is so pitiful here... what does that say about the investors here???
I was able to communicate and confirmed that this was just a required yearly recertification. They are required yearly to have this recertified. That said, it is very important for the import export provisions, which will be very necessary in the future.
I still don’t get it.
I sill don’t get it. Why do traders need to go back and fill opening day gaps, even sometimes waiting a year to fill the gap?
AIGemeni tries to explain
It's a common observation in trading that price often returns to "fill" opening day price per share (PPS) gaps, and it can indeed seem mysterious why this happens, sometimes even after a significant amount of time. While there's no absolute guarantee that every gap will be filled, and the reasons aren't always perfectly clear-cut, here are the main psychological and market dynamics that contribute to this phenomenon:
1. Psychological Factors and Market Memory:
Unfinished Business: Gaps represent a period where there was a significant imbalance between buyers and sellers at certain price levels. It can feel like "unfinished business" to the market. Traders who missed the initial move or feel like certain price levels weren't adequately traded through may anticipate a return to those levels.
Reference Points: Opening prices, especially after significant news or events, can act as strong psychological reference points for traders. They remember the price where the market opened and may expect it to be revisited.
Regret and Opportunity: Traders who were on the wrong side of the gap might look for an opportunity to get out closer to their initial entry point. Conversely, those who missed the move might see the gap fill as a second chance to enter at a favorable price.
2. Technical Analysis and Support/Resistance:
Areas of Inefficiency: Gaps are often seen as areas of price inefficiency. There were no trades executed within the gap range. Technical analysts believe that markets tend to fill these inefficiencies over time as supply and demand forces reassert themselves.
Potential Support or Resistance: The edges of a gap can act as potential support (for an upward gap) or resistance (for a downward gap) levels. When price approaches these levels, there can be increased buying or selling pressure, respectively, potentially leading to the gap being filled.
Pattern Completion: Gap fills can sometimes be part of larger technical chart patterns. For example, a gap might occur within a trend, and the subsequent fill could represent a temporary pullback before the trend resumes.
3. Fundamental Reasons (Delayed Reaction or Information Catch-Up):
Initial Overreaction: Sometimes, the initial reaction to news or events can be an overreaction. As more information becomes available and the market has time to digest it, the price might retrace to more accurately reflect the fundamental value, potentially filling the gap.
Institutional Buying/Selling: Large institutional investors might have specific price targets or strategies that involve filling gaps. They might gradually accumulate or distribute shares within the gap area, eventually leading to its closure.
4. Algorithmic Trading:
Pre-programmed Strategies: Algorithmic trading systems are often programmed to identify and trade based on technical patterns, including gaps. These algorithms can contribute to the filling of gaps by automatically placing buy or sell orders as price approaches the gap area.
Why the Delay (Sometimes a Year or More)?
Market Sentiment and Trend: The prevailing market sentiment and the overall trend of the stock or the broader market play a significant role. A strong uptrend might prevent a downward gap from filling for a long time, and vice versa.
Lack of Catalyst: There might not be a specific catalyst or event that drives the price back to the gap area for an extended period.
Shifting Focus: The market's attention might shift to other factors and news, leaving the gap as an unaddressed anomaly for a while.
Strength of the Initial Move: A very strong and fundamentally driven gap might take longer to fill because the underlying reasons for the gap remain valid for a longer period.
Important Considerations:
Not All Gaps Fill: It's crucial to remember that not all gaps get filled. Some gaps, known as "runaway gaps" or "measuring gaps," can indicate strong momentum and may not be revisited for a very long time, if ever.
Context Matters: The significance of a gap and the likelihood of it being filled depend on the context, including the volume during the gap, the reason for the gap, and the overall market conditions.
Trading Strategy: While gap filling can be a part of some trading strategies, it shouldn't be the sole basis for trading decisions. It's essential to consider other technical and fundamental factors.
In summary, the tendency for gaps to be filled is a result of a combination of psychological factors (market memory, regret, opportunity), technical analysis principles (inefficiency, support/resistance), fundamental adjustments (overreaction, information catch-up), and the influence of algorithmic trading. The time it takes for a gap to fill can vary greatly depending on the strength of the initial move, overall market conditions, and the presence of catalysts.
|
Followers
|
1718
|
Posters
|
|
|
Posts (Today)
|
257
|
Posts (Total)
|
759062
|
|
Created
|
02/02/05
|
Type
|
Free
|
| Moderators skitahoe Steady_T sentiment_stocks CaptainObvious Doc logic JerryCampbell | |||
![]()
“Now this is not the end. It is not even the beginning of the end. But it is, perhaps, the end of the beginning.”
~ Winston Churchill

Stylized Dendritic Cell featured on NWBO board since 2015

- Dr. Linda Liau, PhD, MBA, Professor and Chair, Department of Neurosurgery, David Geffen School of Medicine at UCLA
Clinical Trials
DCVax®-L to Treat Newly Diagnosed GBM Brain Cancer (NCT00045968) - Phase III (Double Blind)
UK (MHRA): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
DE (Germany - PEI): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
Expanded Access Protocol for GBM Patients with Already Manufactured DCVax®-L Who Have Screen-Failed Protocol 020221 (NCT02146066) (Expanded Access)
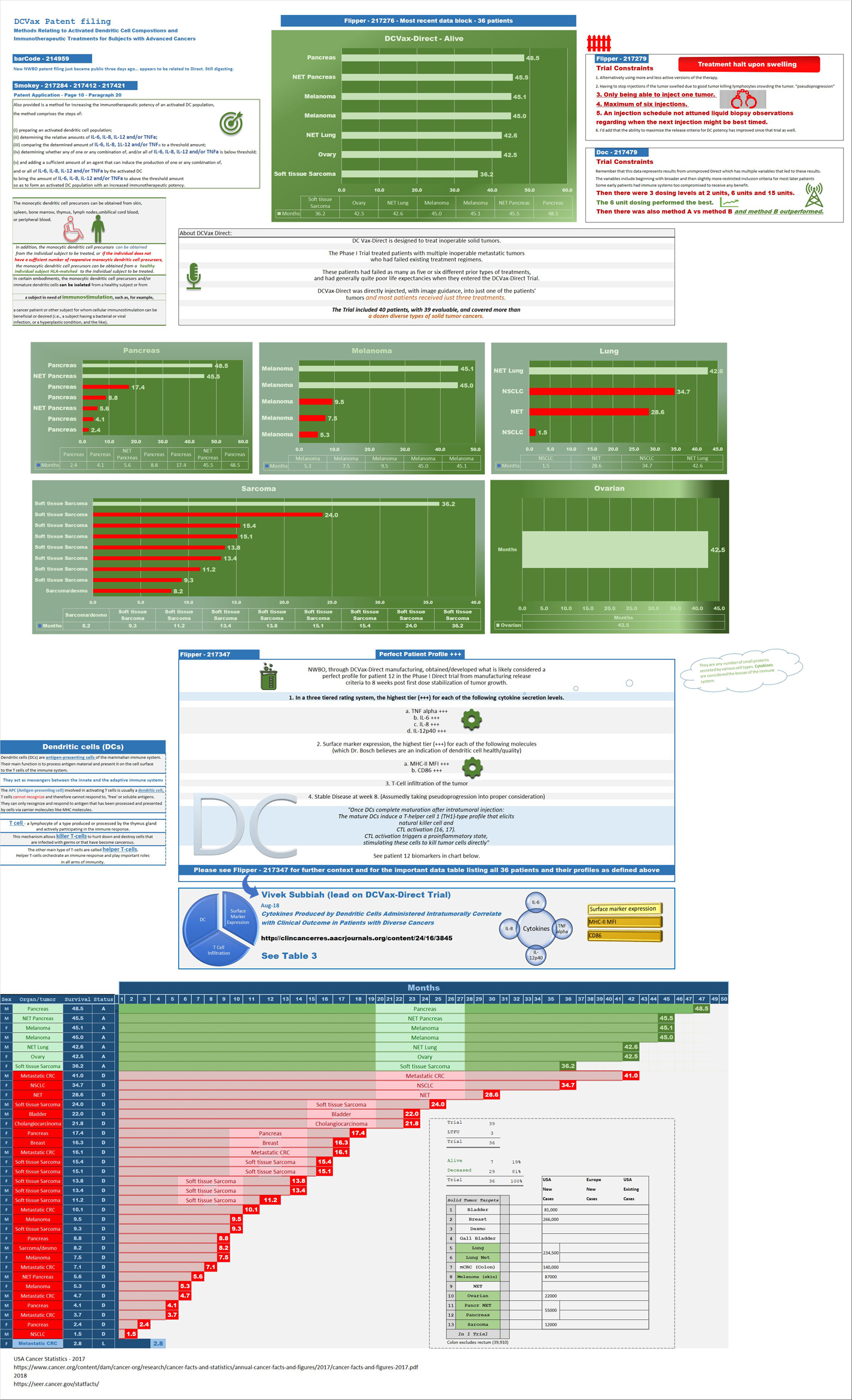
Safety and Efficacy Study of DCVax-Direct in Solid Tumors (NCT01882946) - Phase I/Phase II (Open Label)
UK Clinical Trials - Study of a Drug (DCVax®-L) to Treat Newly Diagnosed GBM Brain Cancer
EU Clinical Trials for DCVax-L - Phase III
Dendritic Cell Vaccine for Patients with Brain Tumors (NCT01204684) - Phase II - at UCLA - Randomized (Open Label) testing DCVaccine with Resiquimod and DC Vaccination with Adjuvant polyICLC
Pembrolizumab and a Vaccine (ATL-DC) for the treatment of Surgically Accessible Recurrent Glioblastoma - Phase 1 (NCT04201873)
Dendritic Cell-Autologous Lung Tumor Vaccine (DCVax-L) and Nivolumab in Treating Patients with Recurrent Glioblastoma - Phase 2 (NCT03014804)
Dendritic Cell Therapy for Brain Metastases From Breast or Lung Cancer (NCT0368765) - Phase 1 - Collaborator: Mayo Clinic
Announcement of DCVax-L and Anti-PD-1 Monoclonal Antibody (Pembrolizumab) for Patients with Liver Metastases of Primary Colorectal Carcinoma Phase 2 Trial - November 17, 2016 - University Medical Center (UMC) of the Johannes Gutenberg University of Mainz
Cognate Bioservices - Owned by Charles River Labs
Website
Company Contact Info
Investor Relations:
Les Goldman (Company) (202) 841-7909 lgoldman@nwbio.com
Sign up for Northwest email list here (hit the subscribe to email list button in the lower right)
Company Headquarters
4800 Montgomery Lane, Suite 800, Bethesda, MD 20814 (240) 497-9024
NW Bio is developing cancer vaccines designed to treat a broad range of solid tumor cancers more effectively than current treatments, and without the side effects of chemotherapy drugs. NW Bio’s proprietary manufacturing technology enables them to produce its personalized vaccine in an efficient, cost-effective manner. NW Bio has a broad platform technology for DCVax dendritic cell-based vaccines.
Their lead product, DCVax-L, is currently in a 331-patient Phase III trial for patients with newly diagnosed Glioblastoma multiforme (GBM), the most aggressive and lethal brain cancer. This trial is currently underway at 69 locations thoughout the United States, Germany and the United Kingdom. NW Bio has also conducted a Phase I/II trial with DCVax-L for late stage ovarian cancer together with the University of Pennsylvania.
Their second product, DCVax-Direct, is currently in a 60-patient Phase I/II trial for direct injection into all types of inoperable solid tumor cancers, with trials currently being conducted at both MD Anderson Cancer Center in Texas, as well as Orlando Health in Florida.
They previously received clearance from the FDA for a 612-patient Phase III trial with its third product, DCVax-Prostate, for late stage prostate cancer.
DCVAX Survival Stories & Testimonials
Alice - Metastic Merkel Cell patient from Florida - ASCO 2018
Brad Silver - GBM patient from Huntington Beach, California - ASCO 2018
Sarah Rigby - GBM patient from Hong Kong - ASCO 2018
Kristyn Power - daughter of GBM patient from Canada - ASCO 2018
Kat Charles - GBM patients from UK - ASCO 2018 - as related by her husband Jason (Kat's Cure)
Prospective patients may contact NW Bio at patients@nwbio.com
UCLA Jamil Newirth DCVax-Patient Video - 2015
Allan Butler Video - National Geographic Vice President - DCVax-Direct patient from Phase 1 Trial with Pancreatic Cancer
NWBO - Patients Sunday Dennis and Jami Newirth - Enrolled at UCLA - Vimeo, Uploaded approx. May 2015
NWBO - Vaccine Helps Keep Brain Cancer Patient Alive (Jennifer Sugioka) - NBC Channel 4, Southern California, February 24, 2015
NWBO - National Geographic's Allan Butler Stage IV Pancreatic Patient using DCVax-Direct at MD Anderson
NWBO GBM Brain Cancer Survival Story of Mark Pace

Presentations

UCLA Agreements
Prostrate
DCVax-Phase II
DCVax-Booster
Upcoming Events
Videos
Linda M. Liau, MD, PhD, MBA - April 24, 2019 at University of Washington, Neurosciences Institute
| Volume: | 4,611,335 |
| Day Range: | 0.16845 - 0.2142 |
| Last Trade Time: | 2:58:40 PM EDT |
| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |




