







Friday, May 27, 2022 8:53:49 PM
PUTTING TO REST THE LIES SPREAD ABOUT NWBO PHASE III TRIAL - PART 5
Continuing with the analysis of the Phase 3 final results presentation, I observed additional things that I would like to share.
Let’s start remembering 2 definitions:
- Left censored patients: Patients that were lost to follow at the time of a survival analysis.
- Right censored patients: Patients that were in the trial and alive at the time of a survival analysis and will continue in the trial. We don't know how long they are going to live and at the time of the analysis they have been in the trial the time shown as a censor (small vertical line in the JTM publication charts).
Now, after that, let’s start with the things observed.
1. An important reason why interim blended results showed a higher mOS than nGBM DCVax-L arm final results did is that in the latter there were no censored patients included at least for the first 19 months and in the former there were 13. Also, all these 13 were left censored (lost to follow), so the ones corresponding to the treatment arm should have been included also in the final results in order to make them comparable. And more important, not including them resulted in obtaining a lower mOS.
2. DCVax-L treatment arm showed statistically significant benefits vs. external control arms in a situation were DCVax-L results were punished taking left censored (lost to follow) patients out for at least the first 19 months, while in the external controls arm they were not taken out. This is true because censored patients help to get better survival results, as I will explain below.
3. With the conclusions 1 and 2 above and analyses from my previous posts, I think that the group of 35 non crossover patients is composed of the 22 non crossover patients with unknown MGMT methylation calculated before and the 13 lost to follow patients (censored left) that were not included in the DCVax-L arm. Not even the ones that started in the original treatment arm.
Now these are the reasons why I came to these conclusions:
a. Why am I saying that there were 13 censored patients at the time of the JTM analysis?
From the Figure below taken from the JTM publication we can count 13 censored patients between 0 and 19 months from surgery.
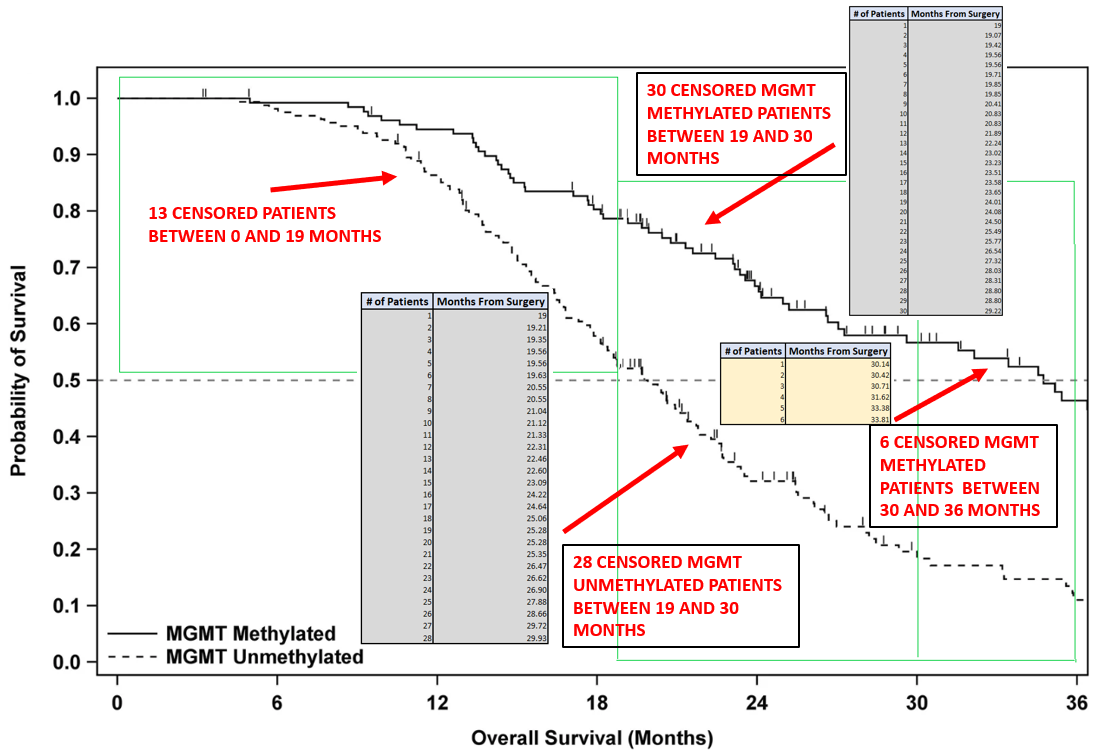
b. Why am I saying that these 13 patients were left censored (lost to follow)?
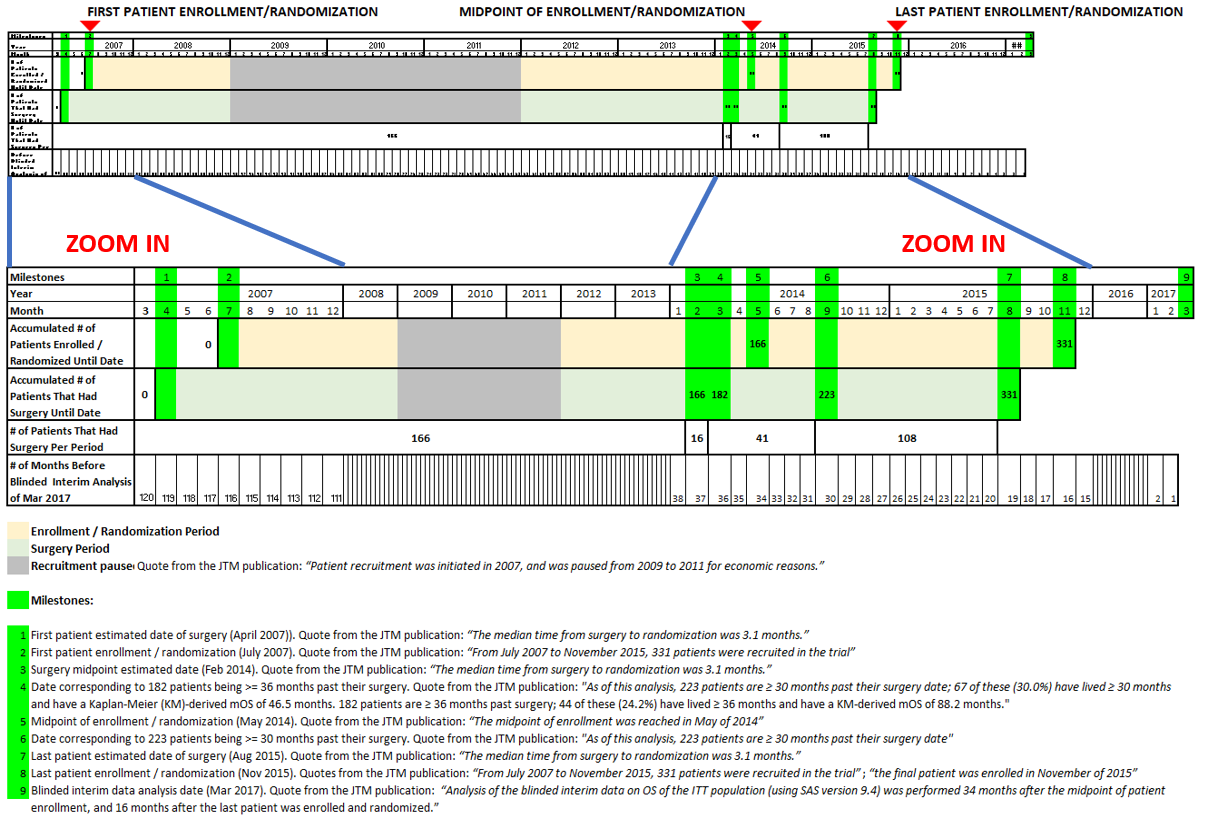
At the time of the JTM interim analysis all patients in the trial had 19 months or more from surgery. This can be seen in the timeline below.
With this in mind and the definitions above for right and left censored patients, we can conclude that for the range of time between 0 and 19 months from surgery, all the censored patients in the interim analysis were left censored (lost to follow). There’s no way we can have a right censored patient in that time period because all patients had 19 or more months in the trial at that time.
c. Why am I saying that in the nGBM DCVax-L arm of the final results there were no censored patients included at least for the first 19 months, as opposed to the external control arms, where censored patients were included?
If we look at the following figure taken from slide 29 of 48 of final results
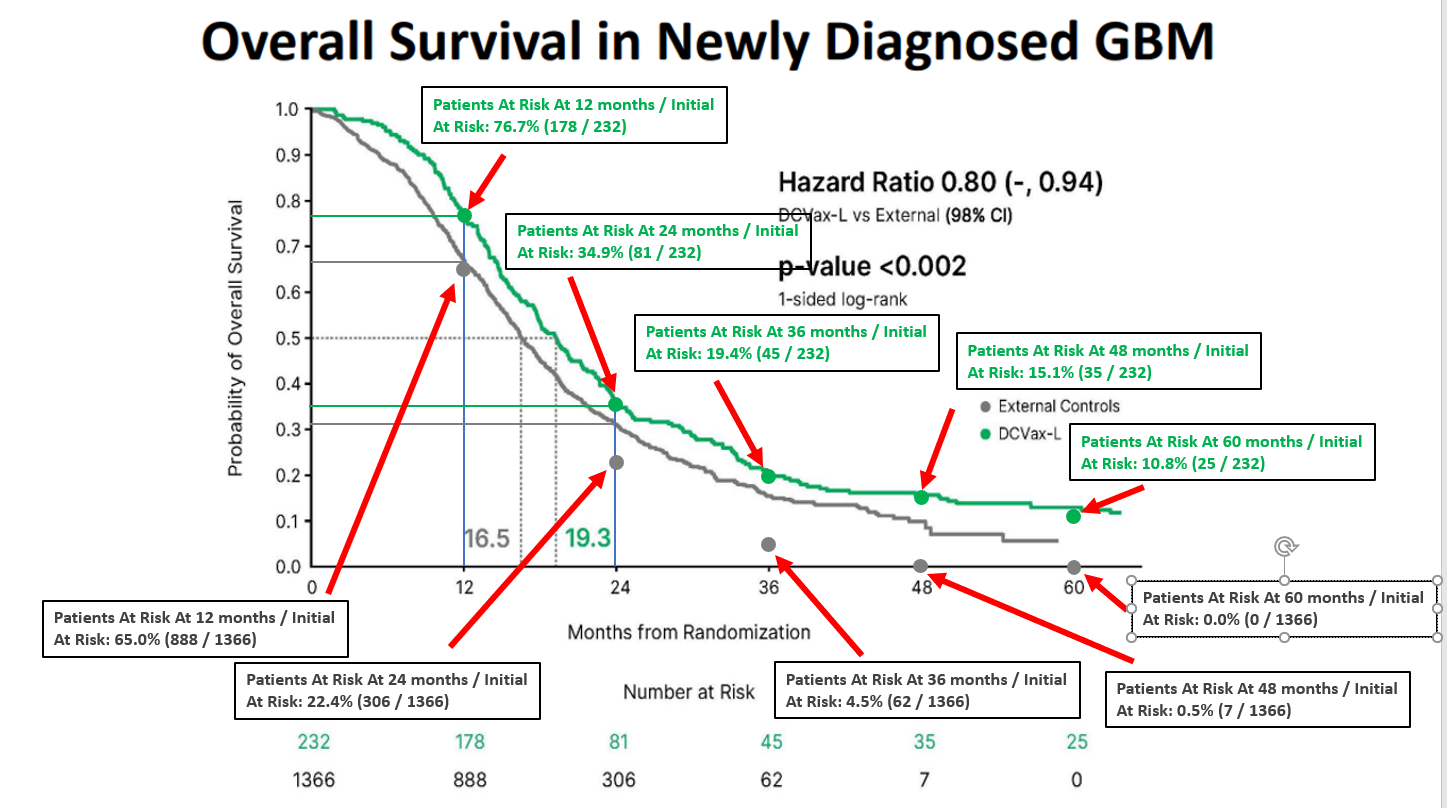
Together with the following Table I prepared
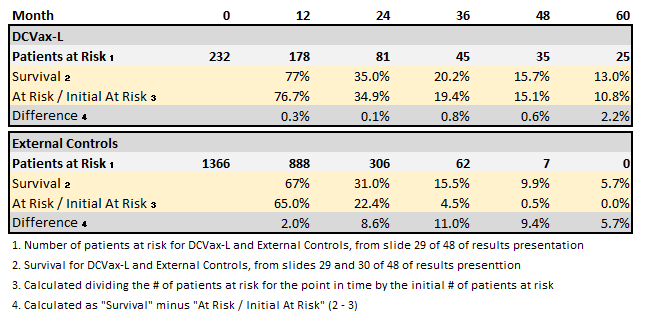
We can note that for the DCVaxL treatment arm the values for “Survival” and “At Risk / Initial At Risk” are the same for 12 (77% vs. 76.7%) and 24 (35.0% vs. 34.9%) months. The small differences (0.3% and 0.1%) correspond to the fact that the “Survival” values were read directly from the chart. This means that there were zero patients censored for the first 24 months in the DCVax-L arm. And because of this, there were zero censored patients for the first 19 months.
For the External Controls arm, on the other hand, the values for “Survival” and “At Risk / Initial At Risk” are different for 12 (67.0% vs. 65.0%) and 24 (31.0% vs. 22.4%) months. The differences are considerable (2.0% and 8.6%). This means that there were patients censored for the first 24 months in the DCVa-L arm. And because of this, there were censored patients for the first 19 months.
Some said there were mistakes in the charts or numbers at risk presented, but that is not true, there are no mistakes. The differences between “Survival” and “At Risk / Initial At Risk” are the effect of censored patients.
d. Why am I saying that censored patients help to get better survival results?
Below is an example of a hypothetical trial in which in in one case the censors were included to calculate the mOS and in the other they were not included. What can be seen is that in the one with censors the mOS is 10 months and in the one without it is 8. This is just an example, but anyone can look for literature to expand on this if wanted.
With this in mind it’s really positive that even taking out its left censored (lost to follow) patients for at least the first 19 months, DCVax-L treatment arm showed statistically significant benefits vs. external control arms where censored patients were not taken out.
Continuing with the analysis of the Phase 3 final results presentation, I observed additional things that I would like to share.
Let’s start remembering 2 definitions:
- Left censored patients: Patients that were lost to follow at the time of a survival analysis.
- Right censored patients: Patients that were in the trial and alive at the time of a survival analysis and will continue in the trial. We don't know how long they are going to live and at the time of the analysis they have been in the trial the time shown as a censor (small vertical line in the JTM publication charts).
Now, after that, let’s start with the things observed.
1. An important reason why interim blended results showed a higher mOS than nGBM DCVax-L arm final results did is that in the latter there were no censored patients included at least for the first 19 months and in the former there were 13. Also, all these 13 were left censored (lost to follow), so the ones corresponding to the treatment arm should have been included also in the final results in order to make them comparable. And more important, not including them resulted in obtaining a lower mOS.
2. DCVax-L treatment arm showed statistically significant benefits vs. external control arms in a situation were DCVax-L results were punished taking left censored (lost to follow) patients out for at least the first 19 months, while in the external controls arm they were not taken out. This is true because censored patients help to get better survival results, as I will explain below.
3. With the conclusions 1 and 2 above and analyses from my previous posts, I think that the group of 35 non crossover patients is composed of the 22 non crossover patients with unknown MGMT methylation calculated before and the 13 lost to follow patients (censored left) that were not included in the DCVax-L arm. Not even the ones that started in the original treatment arm.
Now these are the reasons why I came to these conclusions:
a. Why am I saying that there were 13 censored patients at the time of the JTM analysis?
From the Figure below taken from the JTM publication we can count 13 censored patients between 0 and 19 months from surgery.

b. Why am I saying that these 13 patients were left censored (lost to follow)?
At the time of the JTM interim analysis all patients in the trial had 19 months or more from surgery. This can be seen in the timeline below.

With this in mind and the definitions above for right and left censored patients, we can conclude that for the range of time between 0 and 19 months from surgery, all the censored patients in the interim analysis were left censored (lost to follow). There’s no way we can have a right censored patient in that time period because all patients had 19 or more months in the trial at that time.
c. Why am I saying that in the nGBM DCVax-L arm of the final results there were no censored patients included at least for the first 19 months, as opposed to the external control arms, where censored patients were included?
If we look at the following figure taken from slide 29 of 48 of final results

Together with the following Table I prepared

We can note that for the DCVaxL treatment arm the values for “Survival” and “At Risk / Initial At Risk” are the same for 12 (77% vs. 76.7%) and 24 (35.0% vs. 34.9%) months. The small differences (0.3% and 0.1%) correspond to the fact that the “Survival” values were read directly from the chart. This means that there were zero patients censored for the first 24 months in the DCVax-L arm. And because of this, there were zero censored patients for the first 19 months.
For the External Controls arm, on the other hand, the values for “Survival” and “At Risk / Initial At Risk” are different for 12 (67.0% vs. 65.0%) and 24 (31.0% vs. 22.4%) months. The differences are considerable (2.0% and 8.6%). This means that there were patients censored for the first 24 months in the DCVa-L arm. And because of this, there were censored patients for the first 19 months.
Some said there were mistakes in the charts or numbers at risk presented, but that is not true, there are no mistakes. The differences between “Survival” and “At Risk / Initial At Risk” are the effect of censored patients.
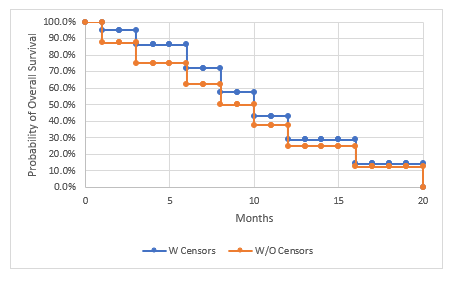
d. Why am I saying that censored patients help to get better survival results?
Below is an example of a hypothetical trial in which in in one case the censors were included to calculate the mOS and in the other they were not included. What can be seen is that in the one with censors the mOS is 10 months and in the one without it is 8. This is just an example, but anyone can look for literature to expand on this if wanted.

With this in mind it’s really positive that even taking out its left censored (lost to follow) patients for at least the first 19 months, DCVax-L treatment arm showed statistically significant benefits vs. external control arms where censored patients were not taken out.
Recent NWBO News
- CNS Drug Delivery Breakthroughs Unlock Significant Biotech Market Opportunities • InvestorsHub NewsWire • 05/11/2026 01:00:00 PM
- CNS Drug Delivery Breakthroughs Unlock Significant Biotech Market Opportunities • GlobeNewswire Inc. • 05/11/2026 12:30:00 PM
- Northwest Biotherapeutics Appoints Dr. Annalisa Jenkins As Strategic Adviser To Advance Dendritic Cell Cancer Vaccine Platform • PR Newswire (US) • 04/30/2026 04:38:00 PM
- Northwest Biotherapeutics Appoints Dr. Annalisa Jenkins As Strategic Adviser To Advance Dendritic Cell Cancer Vaccine Platform • PR Newswire (US) • 04/30/2026 04:30:00 PM
- Northwest Biotherapeutics Announces Establishment Of the Company's Own Dedicated Leukapheresis Clinic • PR Newswire (US) • 04/21/2026 01:30:00 PM
- Northwest Biotherapeutics Announces Establishment Of the Company's Own Dedicated Leukapheresis Clinic • PR Newswire (US) • 04/21/2026 01:30:00 PM
- Form EFFECT - Notice of Effectiveness • Edgar (US Regulatory) • 04/21/2026 04:15:08 AM
- Form POS AM - Post-Effective amendments for registration statement • Edgar (US Regulatory) • 04/16/2026 09:25:30 PM
- Form 8-K - Current report • Edgar (US Regulatory) • 04/07/2026 04:30:50 PM
- Form NT 10-K - Notification of inability to timely file Form 10-K 405, 10-K, 10-KSB 405, 10-KSB, 10-KT, or 10-KT405 • Edgar (US Regulatory) • 03/31/2026 09:04:37 PM
- Form 8-K - Current report • Edgar (US Regulatory) • 01/15/2026 10:06:20 PM
- Form 8-K - Current report • Edgar (US Regulatory) • 01/02/2026 10:14:59 PM
- Form DEF 14A - Other definitive proxy statements • Edgar (US Regulatory) • 11/28/2025 09:43:27 PM
- Form 424B5 - Prospectus [Rule 424(b)(5)] • Edgar (US Regulatory) • 11/25/2025 10:23:07 PM
- Form 8-K - Current report • Edgar (US Regulatory) • 11/20/2025 09:26:03 PM
- Form PRE 14A - Other preliminary proxy statements • Edgar (US Regulatory) • 11/19/2025 09:15:48 PM
- Form 10-Q - Quarterly report [Sections 13 or 15(d)] • Edgar (US Regulatory) • 11/14/2025 09:44:21 PM
- Form 8-K - Current report • Edgar (US Regulatory) • 10/31/2025 04:29:10 PM
- Form 8-K - Current report • Edgar (US Regulatory) • 10/30/2025 08:40:05 PM
- Form 8-K - Current report • Edgar (US Regulatory) • 10/24/2025 04:28:38 PM
- Form 8-K - Current report • Edgar (US Regulatory) • 10/14/2025 06:22:26 PM
- Form 10-Q - Quarterly report [Sections 13 or 15(d)] • Edgar (US Regulatory) • 08/14/2025 09:00:38 PM
- Form 424B5 - Prospectus [Rule 424(b)(5)] • Edgar (US Regulatory) • 07/01/2025 09:04:38 PM


