I wouldn’t call this an outright misstatement, but rather sloppy wording. I’m almost certain he meant that the two prodrugs resolve to the same monophosphate nucleotide. From that point forward, the monophosphate nuke gets converted to a triphosphate nuke in vivo, and hence the two prodrugs eventually produce the same triphosphate.
From a practical standpoint, it wouldn’t make much sense to have the prodrugs resolve to a triphosphate. This would weigh down the parent drugs with extra baggage and would gain little or nothing in terms of PK/PD.
[Updated for VRUS’ PSI-879/PSI-938; clarified that new-generation nucleotide prodrugs resolve to the monophosphate nucleotide.]
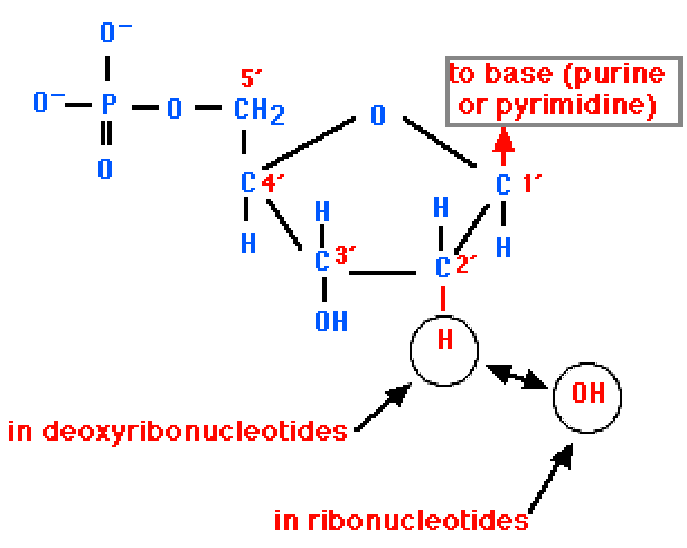
A nucleotide (right) consists of a nucleoside (left) and 1-3 attached phosphate groups. The nucleotide depicted below right is a monophosphate.
Why does the distinction between a nucleoside and a nucleotide matter?
The active agent for all nucleoside/nucleotide antiviral drugs is the triphosphate nucleotide, which is three phosphorylation steps removed from the nucleoside.
IDIX found that a major reason for the failure of NM283, a first-generation nucleoside, was the in vivo inefficiency and patient-to-patient variability of the first phosphorylation step, which converts a nucleoside into a monophosphate nucleotide.
IDIX’s IDX184 and VRUS’ PSI-7851, PSI-879, and PSI-938 are prodrugs of the monophosphate nucleotide; these drugs thus sidestep the problem encountered with NM283 by performing the first phosphorylation step ex vivo.
(The new-generation drugs mentioned above perform the second and third phosphorylation steps in vivo, but these steps do not present a practical problem because they are more efficient and less prone to variability than in vivo performance of the first phosphorylation step.)
 Market Data
Market Data  Markets
Markets