Superfly15, re: your PPHM/Bavituximab commentary, “how many dollars in sales will the glorified placebo Bavi generate in the next 10 years? Answer: ZERO”.
You seem like a reasonable man, so let’s talk.
You either A) Don’t believe that Bavi is going to Double MOS of not only the ctl-arm (Doce), but All 4 currently-approved drugs (Taxotere Altima Tarceva Iressa - see below) in 2nd-Line NSCLC in a robustly-designed randomized, placebo-ctl’d n=121 Ph.2B trial,
or B) You disagree with me about the high unmet medical need of this indication and the large market that currently exists and is projected for it.
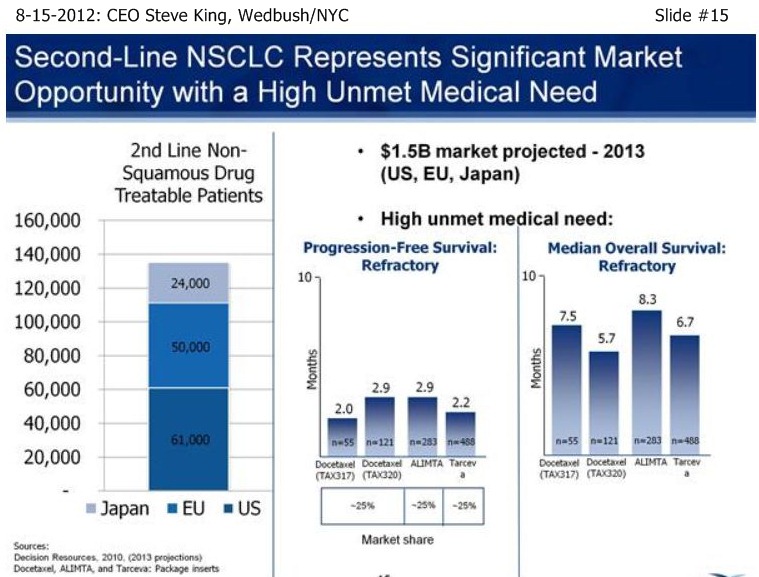
“B” is easy – per Data Resources 2010, $1.5B market projected (US EU Japan), ~125k treatable patients in 2nd-Line non-squamous NSCLC – see 8-15-12 Slide15 ( http://tinyurl.com/8mhrtld ) - screen image included at the end of this post.
Now, “A”. I sense you are skeptical that Bavi is going to show a major advancement in the treatment of 2nd-Line NSCLC. UNDERSTANDABLE - you should be. I only ask you one thing: hold your final judgement until you read about Dr. David Gerber’s late-breaker plenary talk on Sept. 7, 2012 at the ASCO/ASTRO “Chicago Symposium in Thoracic Oncology”:
Sept7 1:40-1:50pm Dr. David E. Gerber (UTSW) #LBPL2: “Randomized, Double-Blind, Placebo-Controlled Phase 2 Trial of Bavituximab + Docetaxel in Patients with Previously Treated [2nd-Line] Locally Advanced or Metastatic Non-Squamous NSCLC (Top-line Results)” => http://www.thoracicsymposium.org/MeetingProgram/Agenda.htm
Watch for the Peregrine Press Release on this ( http://www.peregrineinc.com ), and then the followup articles in the mainstream media (I assure you, I’m not talking BioMedReports, Chimera Research Group, Seeking-Alpha, TheStreet/AF, Motley-Fool, etal) and interviews with Key Opinion Leaders in cancer research that will be forthcoming quickly IMO.
Then, on Sept. 8th or 9th or 10th or so, come back and tell me if you still think Bavi has no future in NSCLC. That’s all I ask, Superfly15.
In the meantime, peruse the following overview of Bavituximab, which concentrates on the ongoing 2nd-Line Lung Cancer trial. But don’t worry, you don’t have to believe a thing there – just wait on Dr. Gerber to confirm & expand on Sept. 7th at ASCO/Chicago.
Take care, cjgaddy
= = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = This is regarding encouraging progress Peregrine’s ongoing Bavituximab vs. 2nd-Line Lung Cancer (NSCLC) in a randomized, placebo-ctl’d, registrational Ph.2B n=121 trial, designed as a “mini Ph.III” by ex-Genentech SVP Robert Garnick.
Storyline & Background:
• Dr. Philip Thorpe, UTSW/Dallas, invented PS-Targeting Therapy, including Bavituximab (Bavi) in early 2000’s. • Bavi targets phosphatidylserine (PS) which exposes on cancer cells & tumor vasculature, but not on normal cells. • As Bavi binds to PS, it triggers vascular disruption and enhances anti-tumor immune response. • Bavi is synergistic with chemo, which increases exposed PS and Bavi uptake. • Bavi is broad-based – works against all solid tumor types. • Bavi is safe, none of Avastin’s side-effects; 600+ pts treated with good safely in 16 trials. • Bavi presently in Ph2B trials & Ph1/2 IST’s for: NSCLC, Pancreatic, Liver, Prostate, Breast, Rectal • Robert Garnick joined Peregrine as Head/Regulatory in 10-2009. • Robert Garnick: 24yrs/Genentech, SVP/Regulatory, 17 approvals, incl. Rituxan, Herceptin, Avastin Lucentis. • Robert Garnick designed Bavi’s randomized trials with FDA in NSCLC & Pancreatic for ”fastest possible Bavi approval” • LEAD IND: 2nd-Line NSCLC Ph2B (Bavi+Doce vs. Doce) enrolled 6-2010 – 10/2011, 121 pts.
HONING IN ON THE ONGOING 2ND-LINE NSCLC “REGISTRATIONAL” TRIAL: http://clinicaltrials.gov/ct2/show/NCT01160601 • Ctl-arm MOS reached in early 2012 at “< 6 mos”. • As of 8-15-12, neither Bavi arm had yet reached MOS. Ie, both Bavi arms at MOS=12mos. and growing day-by-day. • …Curr-Approved 2nd-Line/NSCLC drug #1of4: Taxotere (docetaxel) MOS=6.3mos • …Curr-Approved 2nd-Line/NSCLC drug #2of4: Altima (pemetrexed) MOS=6.3mos • …Curr-Approved 2nd-Line/NSCLC drug #3of4: Tarceva (erlotinib) MOS=5.3mos • …Curr-Approved 2nd-Line/NSCLC drug #4of4: Iressa (gefitinib) “does not improve OS” • Bavi’s Lead Indication: 2nd-Line NSCLC (Lung), high unmet need; will file for AA if data=”home run scenario” • Robert Garnick 7-15-12, “the data is extremely compelling… I've seen a lot of Ph2 & Ph3 data, and this is as compelling Ph2 data as I've ever seen.” • CEO Steve King 8-15-12, “it's going to be a very positive MOS result, it's just a matter now of magnitude." • Dr. David Gerber (MD, UTSW) will present Late-Breaker Plenary talk on Sept. 7th at ASCO/ASTRO Thoracic Conf. in Chicago. • Per CEO SK 8-15-12, Dr. Gerber will update Bavi MOS (whether reached by then or not) and discuss Statistics of trial. • The extent of publicity beg. Sept. 8th re: Dr. Geber’s talking about Bavi Doubling MOS in 2nd-Line NSCLC => TBD.
END OF SUMMARY. . .
= = = = = = = = = = = = = = = = = = = = = = = = = MORE DETAIL OF THE BAVI’s 2nd-LINE NSCLC STORY (with links):
Recall, we learned that the Docetaxel ctl-arm had triggered MOS at “< 6 mos.” (in line with historical Doce data) in the 5-21-12 PR ( http://tinyurl.com/73aeyxj ), while both Bavi arms (low & high dose) had not yet reached MOS.
Given n=121 trial enrollment completed 10-6-2011 and 8-15-12 clarification by CEO Steve King (SK) at Wedbush/NYC that ctl-arm MOS had been already “well-surpassed” by the time of the 4-30-12 data cutoff, that means both Bavi arms were at a conservative minimum MOS of 9 mos. at 5-21-12.
Then on 7-12-12/JMP, SK announced, “the majority of patients are still alive (today) in both Bavi arms, and we expect that to continue for some period of time still.” ( http://tinyurl.com/csdclwb ) => that took Bavi MOS in both arms to min. 11 mos, and growing daily.
Then on 8-15-12/Wedbush, SK announced, “As we're sitting here today, we have still not reached the # of events for MOS in either of the Bavituximab arms - and, in fact, we still have patients that are on treatments… it's going to be a very positive MOS result, it's just a matter now of magnitude." ( http://tinyurl.com/8mhrtld ) => that took Bavi MOS in both arms to min. 12 mos, and still growing daily.
SK finished his 8-15-12 talk with this: “Basically, the longer, the better, obviously – it’s not just great for the program, it’s great for the patients, because, again, we do have patients that are out and still even on treatments as we speak.”
All of the above strongly suggests Bavi is going to Double MOS in 2nd-line adv. NSCLC, at-a-minimum, because each day that goes by Bavi’s MOS continues to grow, 12 mos. and counting as of 8-15-12.
Compare to MOS figures for the currently-approved 2nd-Line NSCLC drugs (per NCI’s Cancer.gov updated 8-15-12 http://tinyurl.com/8lfbrrs ): • Taxotere (docetaxel) => MOS=6.3mos (meta-analysis of 5 trials, 865 pts) • Altima (pemetrexed) => No diff. vs. Docetaxel (Ph.3 non-inferiority vs. Doce, 571 pts) • Tarceva (erlotinib) => MOS=5.3mos (TITAN Ph.III n=424 trial – see http://tinyurl.com/8w8lo93 ) • Iressa (gefitinib) => “Iressa does not improve OS” • Xalkori (crizotinib) => very limited, only for ALK-positive pts (2-7% of pop.) NOTE 10-8-08: “2nd-Line NSCLC: Avastin+Tarceva Improves PFS but Not Overall Survival vs. Tarceva” ( http://cancergrace.org/lung/2008/10/08/beta-neg-for-os )
All that lays the groundwork for this:
On Sept. 7, 2012, Univ-Texas/SW cancer professor Dr. David E. Gerber is going to give a Late-Breaker** Plenary talk on the status of the Bavi 2nd-Line NSCLC trial at the ASCO/ASTRO “Chicago Symposium in Thoracic Oncology”. As SK said 8-15-12, “Even though we haven’t reached MOS, and certainly may not have reached it by Sept. 7th, we still will be able to talk a little bit more about where we’re at in that process. We’ll also be able to talk more about how the statistics in the trial are trending, and how we put those kinds of events together into our thinking about a Phase III trial design.”
**Symposium rules about Late-Breakers: “must contain important late-breaking research results; limited to important new developments from Ph2 & Ph3 trials that will have an impact on practice or research; of high scientific priority” = = = = = = = = = = = = = Sept7 1:40-1:50pm Dr. David E. Gerber (UTSW), Late-breaker PLENARY talk #LBPL2: “Randomized, Double-Blind, Placebo-Controlled Phase 2 Trial of Bavituximab + Docetaxel in Patients with Previously Treated [2nd-Line] Locally Advanced or Metastatic Non-Squamous NSCLC (Top-line Results)” => http://www.thoracicsymposium.org/MeetingProgram/Agenda.htm
NOTE: If MOS still not reached by Sept. 7th, that’ll be a min. of 13 mos. We’ll see.
 Market Data
Market Data  Markets
Markets