 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.






changes_iv
![]()
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
No, no special information other than the following PR, among other positive PRs we've read in recent past:
December 9, 2013...
The Company’s drug development programs continue to progress satisfactorily. The broad-spectrum injectable FluCide™ anti-influenza drug is our most advanced drug candidate. Recently, the Company has announced that FluCide was found to be safe and well tolerated in a small non-GLP safety-toxicology study, even at the maximum feasible dosage level. In addition, the Company has successfully performed studies on the scale up of synthesis of FluCide.
Echo20, just celebrating forthcoming news onTox studies at BASi (West Lafayette, IN) northwest of a small town, Seymour, Indiana.
Tox studies north of Seymour, IN USA
Our small company, NanoViricides, Inc., is very frugal...
Hear, hear, robi-1-kenobi...
By the way, if NNVC was afraid of FluCide toxicity in the larger upcoming Regulatory Toxicity Study, they would not have risked a comprehensive Range-Finding Toxicity Study that showed safety with no toxicity with the Maximum Feasible Dose (MFD) which is ~100x the anticipated therapeutic dose that saved 100% of mice injected with a lethal dose of Flu that killed 100% of untreated control mice.
The Company is scaling up the production of FluCide from gram scale to several hundred grams scale. The Company believes that the scale up and reproducibility of product batches can be effectively controlled.
The Company’s drug development programs continue to progress satisfactorily. The broad-spectrum injectable FluCide™ anti-influenza drug is our most advanced drug candidate. Recently, the Company has announced that FluCide was found to be safe and well tolerated in a small non-GLP safety-toxicology study, even at the maximum feasible dosage level. In addition, the Company has successfully performed studies on the scale up of synthesis of FluCide.
The Company has already successfully scaled up the synthesis to multi-gram scale, sufficient for animal testing, and can easily scale the processes to make kilogram quantities for widespread application in human patients...
"...He [Dr. E.Seymour] presented an extremely bullish picture, answered many questions - and so I bought some more, of course! It was hard not to become more excited due to his great enthusiasm, especially when he talks about cures and predicts this year's progress [2014] will "blow away" last year's impressive work..."~ KMBJN
Excellent discussion of nanoviricides facts!
We will succeed FN, and FAST!
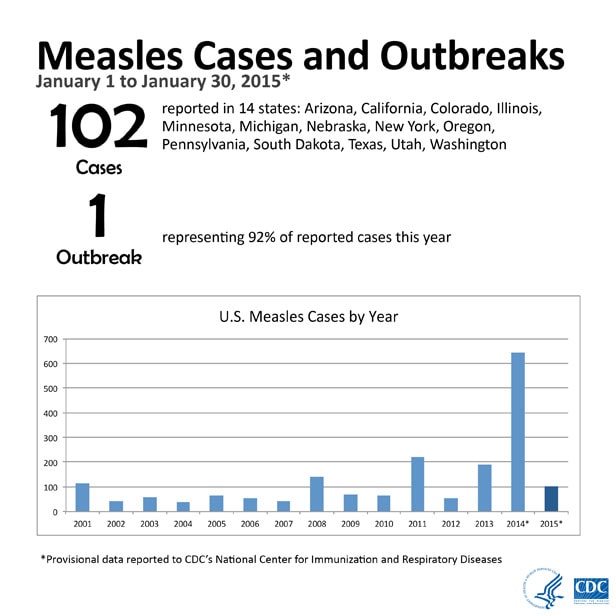
Measles is a respiratory disease caused by a virus. The disease of measles and the virus that causes it share the same name. The disease is also called rubeola. Measles virus normally grows in the cells that line the back of the throat and lungs.
Because nanoviricides operate in a biological/mechanical fashion, we don't need to worry that they will not work in humans. They work anywhere they are encountered by their target viruses. They have virtually no toxicity. They are cheap and have enormously long shelf lives. I would not hesitate to accept an injection right now. When the next pandemic inevitably arrives, I hope to do just that. ~ Patrick Cox
"The rapid development and deployment capability of our platform technology was demonstrated by how quickly we were able to create these drug candidates," said Dr. Eugene Seymour, MD, MPH, Chief Executive Officer of the Company, explaining, "The design of a set of viable ligands was completed [for MERS] in merely three weeks, and the initial syntheses took another four weeks."
Onward drkazmd65, ignition sequence start...!!!
“By 2011, when Dr. Diwan went all out and bought the Controls Drive property, we had spent several years searching for a third party contract manufacturer, capable of producing our drug candidates under the rigorous standards required for clinical trials, without success,” said Eugene Seymour, MD, MPH, adding, “NanoViricides continued to search for available contract manufacturing capability even after Diwan’s purchase of the Controls Drive property. Most facilities we interviewed could not manufacture our novel polymer molecules without extensive renovations. The cost of such custom renovations and equipment would be passed on to us, as is customary. In addition, we would have to train their technicians and scientists and transfer important know how and other aspects of our intellectual property.”
The Company has already successfully scaled up the synthesis to multi-gram scale, sufficient for animal testing, and can easily scale the processes to make kilogram quantities for widespread application in human patients if they are found to be effective and safe.
Why You Should Consider Automated In Vivo Sampling Systems - Automating Sampling
In automated systems, the animals wear harnesses that secure sampling, drug delivery catheters, and data-generating devices. For example, in BASi’s Culex Automated In Vivo Sampling System, the harnesses are connected to sensors that track the animal’s movements. These drive motors that rotate the floor to counter the animal’s movement, allowing the animals to move freely without tangling the lines. Because of this rotational movement, the Culex small animal system is sometimes (affectionately) referred to as the “Raturn,” and the large animal version the “Pigturn.”
“The animals recover quickly from surgery to implant the catheters, and the behavior of the animals connected to the Culex system seems the same as ‘normal’ animals. They just don’t seem aware of anything unusual,” says David Hopper, director of toxicology at BASi.
The key advantage of the automated systems is that they reduce the stress, as technicians do not need to handle animals to take any samples, and even the best socialized and trained animals will become stressed with repeated sampling. “Stress can make major differences to results of trials,” says Robyn McCain, manager and biopharmaceutics technician at Purdue Translational Pharmacology Facility, Purdue University. “We have assessed this by administering the same compound via an automated system with a gastric catheter vs. traditional oral gavage [introduction of material into the stomach by a tube] in rodents. We looked at the differences in drug absorption using blood samples. The plasma levels showed a difference in the rate of absorption, and we theorize this is due to the blood supply to the gut becoming altered because of the ‘fight-or-flight’ response during oral gavage. This could have had a major impact on the outcome of an oral metabolism study.”
“By 2011, when Dr. Diwan went all out and bought the Controls Drive property, we had spent several years searching for a third party contract manufacturer, capable of producing our drug candidates under the rigorous standards required for clinical trials, without success,” said Eugene Seymour, MD, MPH, adding, “NanoViricides continued to search for available contract manufacturing capability even after Diwan’s purchase of the Controls Drive property. Most facilities we interviewed could not manufacture our novel polymer molecules without extensive renovations. The cost of such custom renovations and equipment would be passed on to us, as is customary. In addition, we would have to train their technicians and scientists and transfer important know how and other aspects of our intellectual property.”
The Company has already successfully scaled up the synthesis to multi-gram scale, sufficient for animal testing, and can easily scale the processes to make kilogram quantities for widespread application in human patients if they are found to be effective and safe.
Why You Should Consider Automated In Vivo Sampling Systems - Automating Sampling
In automated systems, the animals wear harnesses that secure sampling, drug delivery catheters, and data-generating devices. For example, in BASi’s Culex Automated In Vivo Sampling System, the harnesses are connected to sensors that track the animal’s movements. These drive motors that rotate the floor to counter the animal’s movement, allowing the animals to move freely without tangling the lines. Because of this rotational movement, the Culex small animal system is sometimes (affectionately) referred to as the “Raturn,” and the large animal version the “Pigturn.”
“The animals recover quickly from surgery to implant the catheters, and the behavior of the animals connected to the Culex system seems the same as ‘normal’ animals. They just don’t seem aware of anything unusual,” says David Hopper, director of toxicology at BASi.
The key advantage of the automated systems is that they reduce the stress, as technicians do not need to handle animals to take any samples, and even the best socialized and trained animals will become stressed with repeated sampling. “Stress can make major differences to results of trials,” says Robyn McCain, manager and biopharmaceutics technician at Purdue Translational Pharmacology Facility, Purdue University. “We have assessed this by administering the same compound via an automated system with a gastric catheter vs. traditional oral gavage [introduction of material into the stomach by a tube] in rodents. We looked at the differences in drug absorption using blood samples. The plasma levels showed a difference in the rate of absorption, and we theorize this is due to the blood supply to the gut becoming altered because of the ‘fight-or-flight’ response during oral gavage. This could have had a major impact on the outcome of an oral metabolism study.”
From past e-mail exchanges from Dr. Seymour notice that they have been supplying Eva Harris - Berkley Lab with DengueCide candidate as well as busy with other projects and now they have stated in today's PR they have sufficient quantities ready for animal testing. Our small company did not PR tox studies have begun. What matter are results and preliminary news on tox results are forthcoming, IMO. Just speculating! The MM's are likely getting ready (quietly accumulating) for such news but are the short-interest coattails ready for such event? Time will tell, soon!
Middle East Respiratory Syndrome (MERS) is viral respiratory illness first reported in Saudi Arabia in 2012. It is caused by a coronavirus called MERS-CoV. Most people who have been confirmed to have MERS-CoV infection developed severe acute respiratory illness. They had fever, cough, and shortness of breath. About 30% of these people died.
So far, all the cases have been linked to six countries in or near the Arabian Peninsula. This virus has spread from ill people to others through close contact. However, the virus has not shown to spread in a sustained way in communities. The situation is still evolving.
CDC is working with partners to better understand the risks of this virus, including the source, how it spreads, and how infections might be prevented. CDC has provided information for travelers and is working with health departments, hospitals, and other partners to prepare for possible cases in the United States.
I'd say lets get ready to do whatever is necessary to get the ONLY DRUG that is low-toxicity and safe to the people in need, broad-spectrum FluCide.
Yes, there are camels in the Indy Zoo but that is not the problem.
I won’t comment on the health implications but with planes of people being tracked and isolated because of infected patients globally and most recently in the United States there could be short-term economic impacts with knock on effects to consumption and employment in the near future.
In the short term, flu-like diseases such as MERS impacts economic growth by reducing demand. Some detail:
- Consumer confidence decreases, (in the case of SARS quite dramatically) in impacted countries, leading to a reduction in private consumption spending. Much of the impact stems from the great uncertainty and fear generated by the disease. People prefer to stay at home (social distancing) to reduce the probability of infection.
- Service exports, in particular tourism but sometimes other sectors (such as education) are almost immediately impacted.
- Transport hubs in the impacted area are also impacted as people either cancel travel or take alternate routes. The Middle East in an important transport hub (as noted by Crawford Kilian on the 19th April).
- Investment is affected by reduced overall demand, heightened uncertainties, and increased risks. Excess capacity will emerge or increase.
- Foreign investment inflow may be delayed or reduced in reaction to a disease outbreak.
- While increased government spending will mitigate the impact, the ability of governments to revive economies facing widespread reductions in private spending is limited.
The Asian Development Bank did some modelling of SARS toward the end of the 2002-2003 outbreak which put the total cost at that time between $12.3 to $28.4-billion. It noted that:
“Of particular concern is the fact that SARS will not only induce hardship for many, but also intensify the problems faced by the poorest and most vulnerable groups in society due to their limited access to medical services. The weakening of demand will further reduce inflation and intensify deflationary pressure in some economies, including PRC; Hong Kong, China; and Taipei, China. Weakened demand will also cause the unemployment rate to rise. Although reduced service exports will lower foreign exchange receipts, imports may be lowered even more due to a significant weakening of domestic demand in the economies concerned.” (source: ADB)
So, in the end MERS is not SARS but if people continue to get infected and carry those infections across the world then from an economic and employment perspective, especially for the Middle East which relies heavily on migrant labour, it might feel like the same thing.
One case of MERS in the state of Indiana. CDC involved.
Will There Be a DengueCide(TM) and/or Dengue Vaccine in Time for the Brazil Olympics, 2016?
Prevalence of Dengue in Brazil
Brazil has the highest prevalence of dengue in the world, reports the World Health Organization. In 2013, reported cases of dengue rose nearly 300 percent, from 70,000 in a seven week period in 2012 to more than 200,000 during the same seven week period in 2013. Not only are native Brazilians at risk, but so are travelers coming to visit for sporting events such as the 2016 Summer Olympics and the 2014 World Cup.
The Potential Dengue Vaccine
Sanofi, a French vaccine research, development and manufacturing company, is in the late clinical trial stages of a dengue vaccine. Previous vaccine trials did not protect against all dengue sub-types, but the current Sanofi vaccine shows considerable promise. If the data show that the vaccine is successful, the first batches of vaccine available to the general public could be ready by late 2015, just in time for the 2016 Summer Olympic games to be held in Brazil.
source: http://www.passporthealthusa.com/2013/09/will-there-be-a-dengue-vaccine-in-time-for-the-brazil-olympics/
A nanoviricide, unlike current vaccines, is a manmade molecule engineered to replace the antibody in the immune system. The nanoviricide works similarly to the antibody, for both selectively tag the virus when it first presents itself; however, the nanoviricide attaches to the virus particle at several sites, using a sort of cluster mechanism, giving it the ability to grasp the virus while encapsulating it and destroying it. This is possible based on the two-part design of the nanoviricide.4 The first is the nanomicelle, or the casing of the nanoviricide. This casing opens up and encapsulates the virus, and by physical and chemical forces, breaks down the virus into harmless pieces. The second feature is the receptor molecule, which is ligand mimicking, meaning that it presents the same chemical features as a normal cell, and creates several binding sites for the virus. Hence we call the nanoviricide a “multisite target,” whereas the antibody attaches at one. The nanoviricide particle recognizes multiple sites and binds to them (currently binding to as many as three different sites) for a highly effective attack. How does the virus allow the binding if it is so specific? Like the surface of a cell, the nanoviricide does not change form, tricking the virus into assuming it has attached to a vulnerable cell. The nanoviricide, disguised as an injured cell, then coats the virus particle with degenerating chemicals, which ultimately renders the virus ineffective, prompting it to disintegrate.4 The nanoviricide dismantles the virus without any immune system assistance, avoiding many of aforementioned issues with current vaccine production mechanisms.
Fundamentally, the major difference between the present vaccine system and the nanoscale one is between the naturally-produced antibody and the manmade nanoviricide. Apart from replacing the immune system, nanoviricides are additionally advantageous as they are biodegradable within the body. This means that the remnants can be recycled or released safely through the blood stream and other body systems.5 Biodegradability results from using naturally occurring polymers to build the nanomicelle.5 Vaccines and nanoviricides differ still further in their applications. Nanoviricides do not necessarily require injection; they can also be topically applied or administered in the form of eye-drops, reducing discomfort and perhaps increasing the effectiveness of the vaccine. That nanoviricides are engineered by man enables rapid, targeted drug development against emerging viruses. It is possible, according to current research, to develop a research drug against a new life threatening viral disease within 3-6 weeks after the infection is found, compared to the years needed to come up with a vaccine from chicken eggs. Other advantages include the low cost of drug development, manufacturing and distribution.
source: http://www.bu.edu/synapse/2011/11/27/nanoviricides/
Good question. If Flucide shows low toxicity and completes Phase 1 and 2 studies, then the next type of nanoviricde should only require a bridge study to show that it processes out of the body in the same way. That bridge study might be a PK for both mice and humans, both very quick studies with minimal subjects, or just a dozen humans following submission of an INDA with only PoC in animals and histological results. By the 3rd or 4th version of nanoviricide the PK would probably be included in a Phase 2 protocol.
This is how salts of drugs already approved or in advanced trials are approved for human trials without full testing after PoC and efficacy animal studies. ~ BigKahuna
Brazil? Don't know much about them. But the WIPO/PCT process is a long and winding one for filings in foreign countries. First there is the filing in WIPO/PCT with all the countries named you want to get a patent in. Then there is a wait of about 12-18 months - followed by a publication of the application. Then there is the ISR - International Search Report - by the designated search authority which outlines your particular situation wrt the prior art. All this takes time. Then you must actually go through the process of asking for a patent in all the designated countries and prosecute your case in those places. More time passes. Sometimes you just get your patent in the USA and Europe and that's it. If you want worldwide coverage that is another route all taking time and money.
Bottom line - wait for 5+ years from first filing. And do NOT be in a hurry! ~ nanopatent
NanoViricides Signs Agreement with Viroclinics Biosciences BV for Testing of Various NanoViricides Against Specific Viruses of Current Concern
WEST HAVEN, Conn.--(BUSINESS WIRE)--February 04, 2014--
Tuesday, February 4th, 2014 - NanoViricides, Inc. (NYSE MKT: NNVC) (the "Company") reported today that it has signed a "confidential disclosure agreement" ("CDA") with Viroclinics Biosciences, BV ("Viroclinics"), a spinoff of the Department of Viroscience at the Erasmus Medical Centre ("Erasmus") in Rotterdam, the Netherlands. The agreement will allow the scientists at Viroclinics to develop a specific proposal for the testing of different nanoviricides(R) , such as FluCide(TM), against viruses of mutual interest to both organizations.
Viroclinics is a virology contract research organization serving the biopharmaceutical community (www.viroclinics.com/en-GB/). Viroclinics provides preclinical as well as clinical development services for vaccines and antivirals. The ongoing, intimate interaction between scientists at Erasmus and Viroclinics staff yields a strong, flourishing platform to create and implement assays at the forefront of viroscience. Viroclinics participated in the discovery and characterization of the Middle East Respiratory Syndrome (MERS) Coronavirus in 2013 and SARS Coronavirus in 2003, attesting to its leadership position in the field.
NanoViricides, Inc. anticipates that we will be able to test and develop our drug candidates against influenzas, dengue, MERS Coronavirus, as well as rabies, with the help of Viroclinics. In particular, NanoViricides is interested in the testing of its lead broad-spectrum anti-influenza drug candidate FluCide against various influenza A strains including the highly lethal H5N1 and H7N9 viruses that pose a strong global public health threat.
Testing of nanoviricides antiviral drug candidates will be performed in a BSL2 or BSL3 facility at Viroclinics, as applicable. These facilities are designed to contain and enable the safe handling of organisms that can pose a significant threat to health. Executives from NanoViricides plan to visit the Rotterdam facility later this month to conclude the final research agreement.
Successful scale up to me means they have done it in a reproducible manner or batches (GMP-like).
The Company also reported that it is producing Injectable FluCide™, our most advanced drug candidate, at its existing facilities, in the large quantity needed for the Safety and Toxicology ("Tox Package") study. The strong safety observed in preliminary safety studies resulted in requirement of a very large quantity for the Tox Package study. Notably, the drug candidate was found to be safe even at the maximum feasible dosage level in a small animal study. The Company reports that it has successfully scaled up the production of injectable FluCide at its current facility.
Detailed laboratory analyses of samples from this non-GLP safety and toxicology study showed no overall systemic effects and no direct effects on the primary organs. This includes liver and kidney tissues as well as liver and kidney function. This is important as the liver and kidneys are major organs involved in drug toxicity. In addition, FluCide showed no adverse effects on the lungs from the treated animals. This is very important because the respiratory system is a primary site of influenza virus infection and tissue damage. These strong safety findings were seen at all doses tested, even at the maximum feasible dose (MFD). MFD was much higher than the therapeutic dose range used to treat influenza virus infections in our animal model efficacy studies. FluCide was administered intravenously by tail-vein injections or by infusion in this study. The non-GLP safety/toxicology study was conducted at KARD Scientific in Massachusetts.
These results support the Company's positive findings in animals that were infected with different influenza A virus strains. In those studies, no safety or toxicology concerns were observed. The Company has previously reported that its FluCide candidate demonstrated extremely high anti-influenza activity in lethal infection animal models using multiple influenza A subtypes. The extremely high anti-influenza activity coupled with the strong safety data were the basis for the selection of this FluCide candidate for further drug development.
As previously reported, the results of this study will provide both the basis and focus for the GLP safety and toxicology studies of FluCide that are required for the IND submission to the U.S. FDA. These GLP studies will be performed on both large and small animals at the BASi facility in Indiana.
BASi Launches Culex NxT Next Generation In Vivo Automated Sampling System --- Dec 2012
...
Developed by BASi to collect pharmacokinetic and pharmacodynamic data, the Culex system can automatically collect blood, bile, metabolites, dialysates and more from awake and freely moving animals as small as mice and as large as swine. The system is used by nine of the world's top ten pharmaceutical companies, universities, and contract research organizations.
"Scientists choose Culex over manual sampling because it delivers better data, which leads to better decision-making," said Candace Rohde-Johnson, director of BASi's Instruments Division. "Incorporating innovative hardware and software improvements, the new Culex NxT has the same small footprint, robust design and ease of use of the original, providing its users peace of mind when away from the lab. Culex's ability to run experiments around the clock versus just during business hours significantly increases our clients' efficiency and productivity in the early stages of drug discovery, including safety pharmacology."
Pre-clinical development: GLP vs. GMP
In drug development, pre-clinical development, also named preclinical studies and nonclinical studies, is a stage of research that begins before clinical trials (testing in humans) can begin, and during which important feasibility, iterative testing and drug safety data is collected.
The main goals of pre-clinical studies are to determine a product's ultimate safety profile. Products may include new or iterated or like-kind medical devices, drugs, gene therapy solutions, etc.
source: http://en.wikipedia.org/wiki/Pre-clinical_development
About two years ago NanoViricides, Inc. started firming out contracts and non-disclosure agreements with different expert organizations.
WEST HAVEN, Conn.--(BUSINESS WIRE)--Jul 23, 2012 - NanoViricides, Inc. (OTC BB: NNVC) (the "Company") announced today that it has retained Australian Biologics Pty. Ltd., a regulatory affairs consulting firm, to coordinate the regulatory review and approval to conduct the first human trials in Australia for Flucide™, the Company's broad-spectrum anti-influenza drug. Australian Biologics will also facilitate clinical trial site(s) selection and development of the clinical trials agreements.
AT-M Ad
Dr. Jim Ackland, the Manager of Australian Biologics Pty, Ltd, has extensive experience in this field. Prior to becoming managing director of this company, he was Vice-President, West Coast and Asia Pacific operations for the Biologics Consulting Group, the Company's US FDA regulatory affairs consulting group. In the 1990's, he was the Head of Regulatory Affairs, Vaccines, for the CSL Group in Australia. The CSL Group is a global, specialty biopharmaceutical company that researches, develops, manufactures and markets products to treat and prevent serious human medical conditions.
“We are very pleased to engage Jim and his staff because of their extensive experience in both the regulatory and operational aspects of the clinical trials landscape in Australia,” stated Eugene Seymour, MD, MPH, Chief Executive Officer of the Company.
We will only make drugs
We do no anti-viral testing on site
That's done by our collaborators
Our place will be absolutely beautiful, high-tech and state of the art for our specific needs in creating the nanoviricides
We anticipate that our facility will be the only anti-viral nanomedicine cGMP production facility in the world (or the US for sure)
I was there and was knocked over
The scientists can't wait to move in!
EUGENE SEYMOUR, MD, MPH
Chief Executive Officer
NANOVIRICIDES, INC
Nanotechnology-based targeted anti-viral therapeutics
NanoViricides, Inc. has assembled a marquee team of experienced personnel to help us with the design, architecture, and engineering of this facility. Mr. Andrew Hahn continues to provide overall stewardship for this project. He was formerly Senior Director of Engineering, Pharmaceutical Facilities, Global Engineering, at the Bristol-Myers-Squibb Company Worldwide Medicines Group (BMS). He has almost 30 years of experience in architecture, design and project management in the creation of new and refurbished facilities at Bristol-Myers Squibb Company. Mr. Phil Mader and his firm, MPH Engineering, LLC (“MPH”), continue to help with the overall project management and design engineering of the laboratory and cGMP pilot production facility. Prior to founding MPH, from 2000 to 2007, Phil Mader served as the Senior Capital Project Manager at Bristol-Myers Squibb Company in Wallingford, CT (“BMS”). He was involved in the design, implementation, and commissioning of various biology and chemistry laboratory projects within budget and in a timely manner. Ms. Kathyann Cowles of ID3A, LLC, serves as the Principal Architect. Ms. Cowles, co-founder of Id3A, has over thirty years of experience as a licensed Architect and Senior Project Manager for diverse and complex design and construction projects in the academic, science, technology, corporate and research sectors.
About two years ago posters here were saying it would be (5) to (7) years before our small company would reach clinical trials. Unless something catastrophic were to happen, we should be in the Clinical Trials within the year (2014-2015).
Eliminating Viruses the NanoViricides Way
By Dan Stanton+, 21-Aug-2013
NanoViricides' nanotech drug delivery platform has the potential to eliminate viruses, the firm says as construction began on a manufacturing facility to support upcoming clinical trials.
http://www.in-pharmatechnologist.com/Drug-Delivery/Elimiating-Viruses-the-NanoViricides-Way
Tamiflu suppresses the virus while broad-spectrum FluCide will eliminate/destroy the virus strains.
The company also believes that by moving away from a vaccine-type approach, treatment can also become far more cost efficient. In an extended trial, FluCide was shown to be 1,500 times more effective than TamiFlu in a lethal animal model.
To support the upcoming trials, construction of the 18,000 sq. ft. facility is expected to be completed by mid 2014. The plant was previously a printing plant and according to Dr. Seymour, "needed a complete renovation to make it a sterile pilot manufacturing facility."
And with the advent of 3D printing of human tissue and organs, who is to say that within the next five years, the new Pilot manufacturing Plant will not house a nanoviricides 3D printer? Possible? Just speculating!
The "bio-ink cartridges" for this 3D nanoviricide-printer???
FluCide is made up of PEG backbone, pendant fatty acids and ligands...~ robi-1-kenobi
Bioprinting refers to the technologies whereby living cells are layered by the additive process yielding highly complex three-dimensional human tissues or organs. The ink used for printing tissues/organs consists of live cells that are delivered from the nozzle of a print-head, building up layer after layer of cells to create a complex 3D structure of a human tissue or organ. Bioprinting is a promising alternative to narrow the gap of the growing demand for human tissue and organs.~ 3D printing: Cell Biology and Beyond! Written by Jay Bhatt
Zero profits!?!
A zero sales/profits condition will not keep a NanoViricides, Inc. pps from skyrocketing to $500pps or $800pps (or more) once it performs well during clinical trials. Before the Clinical trials?...we will climb to $30pps and/or $70pps.
Nanoviricides are currently binary: they either work in humans as they have in animals, or they don't. IMO, there is nothing in between. If they work in humans, then $10 billion will be leaving $40 billion on the table. Pharmassette went for $11 billion with one drug completing Phase 2 and ready for Phase 3. Do the math with that and 5 antiviral drugs plus 200 more in development.~ BigKahuna
Wendy Barclay, a flu expert at Imperial College London with no links to the Cochrane Review or the drugs, said she still felt the benefits were worthwhile, particularly in a pandemic.
"If another pandemic came tomorrow, and the government had no drug with which to treat thousands of influenza infected patients, I imagine there would be a public outcry," she said.
The Cochrane review found that compared with a placebo, or dummy pill, Tamiflu led to a quicker alleviation of flu-like symptoms of around half a day (down from 7 days to 6.3 days) in adults, but the effect in children was more uncertain.
There was no evidence of a reduction in hospitalizations or in flu complications like pneumonia, bronchitis, sinusitis or ear infections in either adults or children, Heneghan's team said, and Tamiflu also increased the risk of nausea and vomiting in adults by around 4 percent and in children by 5 percent.
"...we are a company...with the ability to rapidly create drugs, and when I say rapidly create drugs I'm talking about weeks instead of years..." ~ Dr. Eugene Seymour, CEO Nanoviricides, Inc.
"by the way, I'm sure that when you think human trials for drugs you think of hundreds of millions of dollars and years of time, well in this case because the disease only lasts a week, two weeks,...that it is possible to complete human trials in the space of a few short months...four parts to the human trials" ~ Dr. Eugene Seymour, CEO Nanoviricides, Inc.
thinking about it, short-interest and their toxic chemical compound "loaded mules" are all on the wrong side of the riveerrr!
Hear, hear, leifsmith!
Could anyone be that wrong? I don't doubt there are good people in the FDA (Dr. Tim Cote guided DengueCide to Orphan Drug status) but as Juan Enriquez accounts, there can also be the bad.
"That government is best which governs least", often attributed to Thomas Jefferson.
This is a road on which NanoViricides, Inc. must and is treading carefully! The road to the Clinical Trials (2014-2015).
The Traffic Jam That Kills Thousands of People Every Day
by Juan Enriquez. Posted Apr 22, 2014
...Yep.
Apparently, he didn’t approve a single drug — an absolutely unassailable record!
But the real question is by not approving drugs in the renal and cardiac unit, did he also kill people by not acting? Are there consequences to not acting? Because sometimes by not acting, by being too careful, by making it too expensive, maybe we’re killing more people than regulation is saving. And
how do we measure that? Are there consequences to not measuring some of these costs?
If regulation is killing more people than it is saving, then we’ve got a problem....
source: http://dailyreckoning.com/the-cost-of-not-acting/
What pandemic flu is, how to prepare for an outbreak, and how to prevent spreading the virus. NanoViricides Inc. FluCide is on a path to the market
Agree! The NNVC naysayers are shorting the stock because they've reached the conclusion they can make more money shorting stocks than otherwise. But, do they simply ignore that there is a silent war being waged in their individual bodies as it is being waged in the bodies of many others, friends, family, neighbors, etc.?
Types of viral transformation
There are three types of viral infections that can be considered under the topic of viral transformation. These are cytocidal, persistent, and transforming infections. Cytocidal infections can cause fusion of adjacent cells, disruption of transport pathways including ions and other cell signals, disruption of DNA, RNA and protein synthesis, and nearly always leads to cell death. Persistent infections involve viral material that lays dormant within a cell until activated by some stimulus. This type of infection usually causes few obvious changes within the cell but can lead to long chronic diseases. Transforming infections are also referred to as malignant transformations. This infection causes a host cell to become malignant and can be either cytocidal (usually in the case of RNA viruses) or persistent (usually in the case of DNA viruses). Cells with transforming infections undergo immortalization and inherit the genetic material to produce tumors. Specific changes in the cell are further discussed below.[1]
More: http://en.wikipedia.org/wiki/Viral_transformation
Our time is fleeting, invest in companies of today and tomorrow! Invest in NanoViricides, Inc. (NNVC), maker of low-toxicity, safe, effective and life-saving antiviral therapeutic drugs that will transform the lives of many, for the better.
Chronic Bacterial and Viral Infections in Neurodegenerative and Neurobehavioral Diseases
Garth L. Nicolson, PhD
Lab Med. 2008;39(5):291-299.
Often, patients with neurodegenerative or neurobehavioral diseases have chronic, neuropathic infections that could be important in disease inception, disease progression, or increasing the types or severities of signs and symptoms. Although controversial, the majority of patients with various neurodegenerative or neurobehavioral conditions, such as amyotrophic lateral sclerosis, multiple sclerosis, Alzheimer's disease, Parkinson's disease, and autistic spectrum disorders, show evidence of central nervous system or systemic bacterial and viral infections. For example, using serology or polymerase chain reaction evidence of Chlamydia pneumoniae, Borrelia burgdorferi, Mycoplasma species, human herpesvirus-1 and -6, and other bacterial and viral infections revealed high infection rates that were not found in control subjects. Although chronic infections were not found in some studies, and the specific role of chronic infections in neurological disease pathogenesis has not been determined or is inconclusive, the data suggest that chronic bacterial or viral infections could be common features of progressive neurodegenerative and neurobehavioral diseases.
Neurodegenerative diseases are chronic degenerative diseases of the central nervous system (CNS) that cause dementia. For the most part, the causes of these brain diseases remain largely unknown.[1] They are characterized by molecular and genetic changes in nerve cells that result in nerve cell degeneration and ultimately nerve dysfunction and death, resulting in neurological signs and symptoms and dementia.[1,2] In addition to neurodegenerative diseases, there are also neurobehavioral diseases that mainly, but not exclusively, appear in the young, such as autistic spectrum disorders (ASD) that encompass autism, attention deficit disorder, Asperger's syndrome, and other disorders.[3]
There appear to be genetic links to neurodegenerative and neurobehavioral diseases, but the genetic changes that occur and the changes in gene expression that have been found in these diseases are complex and not directly related to simple genetic alterations.1,4 In addition, it is thought that nutritional deficiencies, environmental toxins, heavy metals, chronic bacterial and viral infections, autoimmune immunological responses, vascular diseases, head trauma and accumulation of fluid in the brain, changes in neurotransmitter concentrations, among others, are involved in the pathogenesis of various neurodegenerative and neurobehavioral diseases.[1-3,5-8] One of the biochemical changes found in essentially all neurological, neurodegenerative, and neurobehavioral diseases is the overexpression of oxidative free radical compounds (oxidative stress) that cause lipid, protein, and genetic structural changes.[5-9]
Oxidative stress can be caused by a variety of environmental toxic insults, and when combined with genetic factors, pathogenic processes could result.[10] An attractive hypothesis for the causation or promotion of neurological disease involves chronic bacterial or viral toxic products, which result in the presence of excess reactive oxygen species and culminate in pathologic changes.[11,12]
Infectious agents may enter the CNS within infected migratory macrophages, they may gain access by transcytosis across the blood-brain barrier, or enter by intraneuronal transfer from peripheral nerves.[11] Cell-wall-deficient bacteria, principally species of Chlamydia (Chlamydophila), Borrelia, Brucella (among others), bacteria without cell walls, such as Mycoplasma species, and various viruses are candidate infectious agents that may play important roles in neurodegenerative and neurobehavoral diseases.[12-14] Since they are usually systemic, such infections can affect the immune system and other organ systems, resulting in a variety of systemic signs and symptoms.[15-18]
Amyotrophic lateral sclerosis (ALS) is an adult-onset, idopathic, progressive neurodegenerative disease affecting both central and peripheral motor neurons. Patients with ALS show gradual progressive weakness and paralysis of muscles due to destruction of upper motor neurons in the motor cortex and lower motor neurons in the brain stem and spinal cord, ultimately resulting in death, usually by respiratory failure.[19,20] The overall clinical picture of ALS can vary, depending on the location and progression of pathological changes found in nervous tissue.[21]
In ALS, the role of chronic infections has attracted attention with the finding of enterovirus sequences in a majority of spinal cord samples by polymerase chain reaction (PCR).[22,23] This finding is not without controversy, since others failed to detect enterovirus sequences in spinal cord samples from patients with or without ALS.[24,25] Nonetheless, infectious agents that penetrate the CNS may play a role in the etiology of ALS, although evidence for a transmission of an infectious agent or transfer of an ALS-like disease from man-to-man or man-to-animal has not been demonstrated.[26]
The presence of systemic mycoplasmal infections in ALS patients has been investigated with PCR methods.[27,28] Our studies indicated that 100% of Gulf War veterans diagnosed with ALS (N=8 from 3 different nations) had systemic mycoplasmal infections.[27] All but 1 patient had Mycoplasma fermentans, and 1 veteran from Australia had a systemic M. genitalium infection. In approximately 80% of nonmilitary (unrelated to military patients) ALS patients from the United States, Canada, and Great Britain (N=28), blood mycoplasmal infections were also found.[27] Of the mycoplasma-positive civilian patients who were further tested for M. penetrans, M. fermentans, M. hominis, and M. pneumoniae, most were positive for M. fermentans (59%), but other Mycoplasma species, such as M. hominis (31%) and M. pneumoniae infections (9%), were also found. Some of the civilian ALS patients had multiple mycoplasmal infections; however, multiple mycoplasmal infections were not found in the military patients with ALS.[27] In another study in Mexico, 10 of 20 ALS patients showed evidence of systemic Mycoplasma species by analysis of their blood by PCR.[28]
Another chronic infection that is commonly found in ALS patients who live in certain areas is Borrelia burgdorferi, the principal etiologic agent of Lyme disease (LD). For example, ALS patients who live in New York, an LD-intense area, were examined for B. burgdorferi infections, and over one-half were found to be seropositive for Lyme Borrelia compared with 10% of matched controls.[29] In addition, some patients diagnosed with ALS were subsequently diagnosed with neuroborreliosis.[30] A survey of the literature indicates that spirochetal forms have been observed for some time in the CNS tissue of ALS and other neurodegenerative diseases.[31] Thus, a byproduct of LD may be progression to ALS, but this is probably only possible in some LD patients who have the genetic susceptibility genes for the neurodegenerative disease and who have other toxic exposures.[32,33]
Amyotrophic lateral sclerosis patients also have other chronic infections, including human herpesvirus-6 (HHV6), Chlamydia pneumoniae, and other infections.[34,35] A suggestion that retroviruses might be involved in ALS and other motorneuron diseases[36] prompted McCormick and colleagues[37] to look for reverse transcriptase activity in serum and cerebrospinal fluid (CSF) of ALS and non-ALS patients. They found reverse transcriptase serum activity in one-half of ALS cases but in only 7% of controls (P <0.008). Interestingly, only 1 of 25 ALS CSF samples contained reverse transcriptase activity.[37]
The exact role that infections play in the pathogenesis or progression of ALS is not known. They could be cofactors in ALS pathogenesis, or they could simply be opportunistic infections that cause morbidity in ALS patients, such as the respiratory and rheumatic symptoms and other problems often found in ALS patients. They could also be involved in the progression of ALS rather than in its inception. Although the exact cause of ALS remains unknown, there are several hypotheses on its pathogenesis: (a) accumulation of glutamate causing excitotoxicity; (b) autoimmune reactions against motor neurons; (c) deficiency of nerve growth factor; (d) dysfunction of superoxide dismutase due to mutations; and (e) chronic infection(s).[22-24,27-29,31-34] None of these hypotheses is exclusive, and ALS may have a complex pathogenesis involving multiple factors.[34] Future studies should determine more precisely the role of chronic bacterial and viral infections in the pathogenesis and progression of ALS.
Multiple sclerosis (MS) is the most common demyelinating disease of the CNS, and it can occur in young as well as older people. In MS, inflammation and the presence of autoimmune antibodies against myelin and other nerve cell antigens are thought to cause the myelin sheath to break down, resulting in decrease or loss of electrical impulses along the nerves.[38,39] In the progressive subset of MS, neurological damage occurs additionally by the deposition of plaques on the nerve cells to the point where nerve cell death occurs. In addition, breakdown of the blood-brain barrier in MS is associated with local inflammation caused by glial cells.[38,39] The clinical manifestations of demyelinization, plaque damage, and blood-brain barrier disruptions are variable but usually include impaired vision, alterations in motor, sensory, and coordination systems, and cognitive dysfunction. Often these are cyclic (relapsing-remitting subset) over time, but a substantial MS subset progresses without remitting.[39]
There is strong evidence for a genetic component in MS.[40,41] Although it has been established that there is a genetic susceptibility component to MS, epidemiological and twin studies suggest that MS is an acquired, rather than an inherited, disease.[42]
The possibility that MS is linked to chronic infections has attracted attention.[43,44] In fact, MS patients show immunological and cytokine elevations consistent with chronic infections.[44-46] A possible infectious cause for MS has been under investigation for approximately the last decade, and patients have been examined for various viral and bacterial infections.[44,47] One of the most common findings in MS patients is the presence of antibodies and DNA of C. pneumoniae in their CSF.[47-49] For example, Sriram and colleagues[48] examined relapsing-remitting (N=17) and progressive (N=20) MS patients for the presence of C. pneumoniae in CSF by culture, PCR, and immunoglobulin reactivity with C. pneumoniae elementary body antigens. They were able to isolate C. pneumoniae from 64% of MS patients' CSF versus 11% of patients with other neurological diseases. High rates of PCR-positive (MOMP gene) patients (97% MS-positive versus 18% with other neurological diseases) as well as serology-positive patients (86% MS-positive, confirmed by enzyme-linked immunosorbant assays [ELISA] and Western blot analysis) were found in MS.[48] Further examination of MS patients for oligoclonal antibodies against C. pneumoniae revealed that 14 of 17 patients were positive, whereas none of the control non-MS patients had antibodies that were absorbed by C. pneumoniae elemental body antigens.[49]
Other studies have also found evidence for the presence of C. pneumoniae in MS patients but at lower incidence. Fainardi and colleagues[50] used ELISA techniques and found that high-affinity antibodies against C. pneumoniae were present in the CSF of 17% of 71 MS cases compared with 2% of 52 patients with noninflammatory neurological disorders. They found that the majority of the progressive forms of MS were positive compared with patients with remitting-relapsing MS. The presence of C. pneumoniae antibodies were also found in other inflammatory neurological disorders (N=51), and thus it was not specific to MS.[50] Using immunohistochemistry, Sriram and colleagues[51] performed a study of formalin-fixed CNS tissue from MS and non-MS neurological disease controls and found that in a subset (7 of 20) of MS patients, chlamydial antigens were localized to ependymal surfaces and pariventricular regions. Staining was not found in 17 CNS tissue samples from other neurological diseases. Frozen tissues were available in some of these MS cases, and PCR amplification of C. pneumoniae genes was accomplished in 5 of 8 CNS tissue samples from MS patients but none in 17 frozen CNS tissues from other neurological diseases. In addition, they examined CSF sediment by immuno-gold-labeled staining for chlamydial antigens and found by electron microscopy that the electron-dense bodies resembling bacterial structures correlated with PCR-positive results in 10 of 11 MS cases.[51] The same group also used different nested PCR methods to examine additional C. pneumoniae gene sequences in the CSF of 72 MS patients and linked these results to MRI evidence of MS-associated lesions.[52] Similarly, Grimaldi and colleagues[53] linked the presence of C. pneumoniae infection with abnormal MRI results in 23 of 107 MS patients with more progressive disease. In addition, a higher rate of C. pneumoniae transcription was found by Dong-Si and colleagues[54] in the CSF of 84 MS patients. The above, among other data,[55-57] support the presence of C. pneumoniae in the CNS of MS patients, at least in a subset of more progressed patients that are most likely the progressive forms of MS.
Not all studies have obtained evidence, however, for the presence of C. pneumoniae [58,59] or other bacteria[60] in the CNS of MS patients. Hammerschlag and colleagues[61] used nested PCR and culture to examine 12 frozen brain samples from MS patients but could not find C. pneumoniae in any of the tissue samples. Alternatively, in one study, C. pneumoniae was found at similar incidence in MS and other neurological diseases, but only MS patients had C. pneumoniae in their CSF.[59] Swanborg and colleagues[62] have reviewed the evidence linking C. pneumoniae infection with MS and have concluded that they are equivocal due to negative reports, and they also speculated that specific genetic changes may be necessary to fulfill the role of such infections in the etiology of MS.
Another possible reason for the equivocal evidence linking MS etiology with infection, such as C. pneumoniae, is that multiple coinfections could be involved. In addition to C. pneumoniae found in most studies, MS patients could also have Mycoplasma species, B. burgdorferi, and other bacterial infections as well as viral infections.[63] When multiple infections are considered, it is likely that >80% of MS patients have obligate intracellular bacterial infections caused by Chlamydia (Chlamydophila) or other bacteria that can be intracellular, such as Mycoplasma, Borrelia, and other infections. These infections were found only singly and at very low incidence in age-matched subjects.[63] In spite of these findings, others did not find evidence of Mycoplasma species in brain tissue (N=30), CSF, or peripheral blood (N=57) of MS patients.[64]
Viruses have also been associated with MS. Certain viruses have been found in MS patients, such as HHV6, but these viruses have also been found at lower incidence in control samples.[62] Sanders and colleagues[65] used PCR to examine postmortem brain tissue (N=37) and controls (N=61) for the presence of neurotrophic viruses. They found that 57% of MS cases and 43% of non-MS neurological disease controls were positive for HHV6, whereas 37% and 28%, respectively, were positive for herpes simplex virus (HSV1 and HSV2) and 43% and 32%, respectively, were positive for varicella zoster virus; however, these differences did not achieve significance, and the authors concluded that "an etiologic association to the MS disease process [is] uncertain." They also found that 32% of the MS active plaques and 17% of the inactive plaque areas were positive for HHV6.[65] Challoner and colleagues[66] used sequence difference analysis to search for pathogens in 86 MS brain specimens. Using PCR, they found that >70% of the MS specimens were positive. They also used immunocytochemistry and found staining around MS plaques more frequently than around white matter; nuclear staining of oligodendrocytes was also seen in MS samples but not in controls.[66] Using immunofluorescent and PCR methods, HHV6 DNA has also been found in peripheral leukocytes in the systemic circulation of MS patients.[67,68] However, using PCR methods, others did not find herpesviruses in the peripheral blood or CSF of MS patients.[69,70]
Although significant information (reviewed in[43,44,70]) points to an infectious process in MS, this remains a controversial concept. As evidence emerges of new possible pathogens in MS, such as a new putative retrovirus,[71] these reports must be intensively examined and further studies initiated. Since most studies have found that the progressive form of MS, rather than relapsing-remitting forms of MS, were associated with chronic infections, infections might be more important in MS progression than in its inception. Various infections may also nonspecifically stimulate the immune system.[43] As in other neurodegenerative diseases, multiple factors appear to be involved in the pathogenesis of MS. Thus, like ALS, MS progression may turn out to be more likely linked to chronic infections, rather than its inception.
Alzheimer's disease (AD), the most common cause of dementia, is a collection of brain disorders usually found in aged patients. The disease is characterized by slow, progressive loss of brain function, especially notable by lapses in memory, disorientation, confusion, mood swings, changes in personality, language problems (such as difficulty in finding the right words for everyday objects), loss of behavioral inhibitions, loss of motivation, and paranoia. The prognosis and course of AD varies widely, and the duration of illness can range from a few years to over 20 years. During this time, the parts of the brain that control memory and thinking are among the first affected, followed by other brain changes that ultimately result in brain cell death.[72]
Alzheimer's disease is characterized by distinct neuropathological changes in the brain. Among the most notable are the appearance of plaques and tangles of neurofibrils within brain nerves that affect nerve synapses and nerve-nerve cell communication. Both of these structural alterations involve the deposition of altered amyloid (Aß) proteins.[73,74] Although the cause of AD is not known with any certainty, the formation of the amyloid plaques and neurofiber tangles may be due to genetic defects and resulting changes in the structure of Aß proteins, neurotox-icity caused by chemicals or other toxic events, inflammatory responses, oxidative stress and increases in reactive oxygen species, loss of nerve trophic factors important in nerve physiology, and loss of nerve cell transmission.[73-77]
Brain infections in AD have only recently become an important topic.[78-80] One pathogen that has attracted considerable attention is C. pneumoniae.[81,82] As mentioned above, this intracellular bacterium has a tropism for neural tissue,[81] and it has been found at high incidence in the brains of AD patients (17 of 19 patients in brain areas of typical AD-related pathology) by PCR and immunohistochemistry methods.[82] Chlamydia pneumoniae has also been found in nerve cells in close proximity to neurofibrillary tangles.[82,83] This microorganism can invade endothelial cells and promote the transmigration of monocytes through human brain endothelial cells into the brain parenchyma.[84] Although C. pneumoniae has been found in the brains of most AD patients studied,[77,81] and this infection results in amyloid beta (Aß) plaque formation in mice injected with C. pneumoniae,[85] some investigators have not found an association of C. pneumoniae infection with AD using PCR or immunohistochemistry.[86,87]
In addition to C. pneumoniae, evidence has been forthcoming that AD patients also have other bacterial infections, such as B. burgdorferi.[88] This infection has been examined in AD cases by serology, culture, Western blot, and immunofluorenscence;[89,90] however, others could not find evidence of B. burgdorferi in AD patients.[91,92] The presence of intracellular infections, like B. burgdorferi in AD patients, has been hypothesized to be a primary event in the formation of AD amyloid plaques by forming "congophilic cores" that attract amyloid materials.[93] Multiple reports show that AD nerve cells are often positive for B. burgdorferi.[88-90,93,94]
In addition to the hypothesis that intracellular microorganisms may provide "cores" for the attraction of amyloid materials, the induction of reactive oxygen species, lipid peroxidation, and the breakdown of the lysosomal membranes releasing lysosomal hydrolases are also thought to be important in amyloid deposition.[94] Although the possibility that infections may be important in AD pathogenesis is attractive, some negative reports where investigators have not confirmed the presence of infections, such as B. burgdorferi, in AD patients, indicate that this is still controversial (reviewed in[91,94]).
Herpes simplex virus infections have also been found in AD, and an interesting relationship has developed between the presence of HSV1 in AD.[95] It had been noted previously that HSV1 but not a related neurotrophic virus, varicella zoster virus, was found often in AD brains and may be linked to patients who have the AD risk factor ApoE e4 allele.[96,97] In AD, HSV1 is thought to be involved in the abnormal aggregation of beta amyloid or Aß fragments within the brain by reducing the amount of full length amyloid precursor protein and increasing the amount of the Aß fragment from this precursor.[98] Recently, Wozniak and colleagues[99] showed that HSV1 infection of cultured glial and neuronal cells results in a dramatic increase in the intracellular levels of beta amyloid forms, whereas the levels of native amyloid precursor protein decreased. This is similar to what has been found in mice infected with HSV1, indicating that HSV1 is probably involved directly in the development of senile-associated plaques. Another herpesvirus, HHV6, has also been found in AD patients, but it is thought that this virus is not directly involved in AD pathogenesis, but it may exacerbate the effects of HSV1 in ApoE e4 carriers.[100]
In spite of the evidence that AD has been associated with, for example, C. pneumoniae, HSV1, or other infections, Robinson and colleagues[101] have stressed caution in concluding that infections act as a trigger or cofactor in AD. In particular, there is a paucity of experimental evidence that pathogens can elicit the neuropathological changes and cognitive deficits that characterize AD. They also stress that there is a need for consideration of systemic infections as potential contributors to the pathogenesis of AD.
Read more: http://www.medscape.com/viewarticle/574944_4
nanopatent, about one to two years ago some people were saying that clinical trials were 5-7 years down the road...the sooner, the better...
what excites me is MONEY, bags and bags of money - sorry to be so crude but it just is
mdphd1, the waiting is trying to kill me as well but then I stop to think it is no longer 9 years wait to clinical trials but more like 12 months in a countdown. I then go and take care of other matters. NanoViricides, Inc. is not alone in this journey. It has collaborators. The good news that are coming our way we've seen before, but this time they attest to the small company's readiness for the clinical trials.
FN, from your email exchange with Dr. Seymour...
Look at what we're doing
I'm here in Europe to finish the H7N9, H5N1 and MERS contracts with both European groups. We're working with Eva Harris on Dengue, and finishing our herpes work at the medical school in Ohio! As soon as the genital herpes work us completed, we will do our confirmatory ophthalmic herpes studies.
The plant is almost done and the scale-up is well underway in the current labs
Preliminary tox studies showed absolutely no evidence of toxicity and we're preparing product for the large-scale tox studies at BASI.
I couldn't be more excited about our prospects, ~ Dr. Eugene Seymour, CEO NanoViricides, Inc.
The non-GLP safety and toxicology study was begun in late September at KARD Scientific in Massachusetts. The results of this study will provide the basis and focus for the IND-enabling GLP safety and toxicology studies of FluCide that are required for the IND submission to the U.S. FDA. These IND-enabling GLP safety and toxicology studies will be performed by BASi Toxicology Services in West Lafayette, IN. The Company has previously reported that its FluCide candidate was highly effective in animal models of different influenza A virus strains. In those efficacy studies of FluCide, no safety or toxicology concerns were observed. As a result, the required quantity estimated for GLP safety/tox study is much larger than our current synthesis capability. The Company has undertaken process development, scale-up, chemistry optimization and control program to enable large scale synthesis of FluCide in a reproducible manner. This work is currently in progress.
The GLPs are designed to protect scientific data integrity, and to provide EPA or FDA with a clear and auditable record of open-ended research studies. In contrast, the GMPs are intended to demonstrate to FDA whether or not individual batches of a regulated product are manufactured according to pre-defined manufacturing criteria.
"We are doing all of the preparatory pre-tox work now and the formal tox studies by BASI will start as soon as the pre-tox work is done and an [sic] sufficient amount of material is available from the existing lab
We're estimating a June start though that could go either way by 2-3 months depending on both BASI's schedule and ours." ~ Dr. E. Seymour, CEO NanoViricides, Inc.
Use of antiretrovirals for treatment and prevention of HIV infection
Standard antiretroviral therapy (ART) consists of the combination of at least three antiretroviral (ARV) drugs to maximally suppress the HIV virus and stop the progression of HIV disease. Huge reductions have been seen in rates of death and suffering when use is made of a potent ARV regimen, particularly in early stages of the disease.
Since 2013, WHO also recommends the ARV use for the prevention of HIV infection, particularly for pregnant women, young children, and key populations exposed to HIV risk. Countries are now following to adapt and implement these recommendations within own epidemiological settings.
WHO is also working to improve scaling up of ARV use in developing countries by optimizing drugs and diagnostics and enhancing community engagement.
source: http://www.who.int/hiv/topics/treatment/en/
related: A new era of antiretroviral drug toxicity -
http://www.ncbi.nlm.nih.gov/pubmed/19430091
NanoViricides Reports It Has Successfully Improved HIVCide Drug Candidate in Cell Culture Studies September 16, 2013 07:00 AM Eastern Daylight Time
WEST HAVEN, Conn.--(BUSINESS WIRE)--NanoViricides, Inc. (OTC BB:NNVCD) (the "Company") reports that it has successfully improved upon its previous lead anti-HIV drug candidate, based on cell culture studies. An improved broad-spectrum anti-HIV nanoviricide that inhibited two distinctly different types of HIV-1 viruses equally well has been identified. This drug candidate also exhibited a very large therapeutic index. The Company has previously reported that it is optimizing the anti-HIV drug candidate. These cell culture studies were conducted by Southern Research Institute, Frederick, MD.
The Company has previously reported unprecedented anti-HIV efficacy from our previous anti-HIV drug candidate, matching or exceeding the effectiveness level of a three drug HAART cocktail in the standard humanized mouse model studies.
With further optimization, the Company believes that it has now achieved extremely high efficacy levels for its lead and backup HIVCide candidates. Further optimization of the nanomicelle portion of the anti-HIV drug candidates is now in progress.
another_voice_2s, we read your posts loud and clear! On the NNVC board, fire away when ready...
noretreat,...Non-GLP toxicity studies
Obtaining high quality non-GLP toxicology data in the early stages of developing a new drug is a critical and cost-effective step in guiding a subsequent GLP toxicology program.
source: http://explorabiolabs.com/services/non-glp-toxicity-studies.html
Secret Science - from Tom’s Reading List...
The New York Times “For the first time ever, a government advisory board is asking scientific journals not to publish details of certain biomedical experiments, for fear that the information could be used by terrorists to create deadly viruses and touch off epidemics. ”
The Guardian “The chicken cull took place after the deadly H5N1 virus was discovered in birds at Hong Kong’s biggest poultry wholesale market. The virus was found in a dead chicken and in two wild birds. The Hong Kong government suspended trade in live chickens for 21 days and banned live imports from mainland China in a bid to prevent the disease from spreading.”
BBC “In a darkened conference room in Malta in September, a Dutch scientist announced to a virology meeting that he had created a mutated strain of H5N1 bird flu which had the potential to spread between humans.”

In this Friday, Feb. 18, 2011 file photo, Indian health workers carry killed ducks to burry them at the R.K. Nagar Government Duck Farm in Agartala in the remote northeastern state of Tripura, India. An official says around 4.000 birds have been culled at a government-run duck farm in the state after some poultry tested positive for a deadly strain of bird flu that can potentially be fatal for humans. (AP)
source: http://onpoint.wbur.org/2011/12/22/super-bird-flu
Ebola Outbreak Shakes West Africa

Health workers teach people about the Ebola virus and how to prevent infection, in Conakry, Guinea, Monday, March 31, 2014. Health authorities in Guinea are facing an “unprecedented epidemic” of Ebola, the international aid group Doctors Without Borders warned Monday as the death toll from the disease that causes severe bleeding reached 78. (AP)
If you feel like it, write to your U.S. Senator/U.S. Representative about a little known 'small company' in Connecticut with great science, a 'small company' we've all come to know as NanoViricides, Inc..
Puffer, like the idea that the "good doctors", employees, collaborators meet regularly to see where they are in their conservative plan with the idea to surprise the competition, knowing full well they've been given guidance by the FDA and that they can deliver fast, characteristic of NanoViricides, Inc.
A couple of years ago people were posting about NanoViricides, Inc. clinical trials in 5 - 7 years. Today we are on-track to deliver clinical trials Q1 2014.
"...we are a company...with the ability to rapidly create drugs, and when I say rapidly create drugs I'm talking about weeks instead of years..." ~ Dr. Eugene Seymour, CEO Nanoviricides, Inc.
"...by the way, I'm sure that when you think human trials for drugs you think of hundreds of millions of dollars and years of time, well in this case because the disease only lasts a week, two weeks,...that it is possible to complete human trials in the space of a few short months...four parts to the human trials..." ~ Dr. Eugene Seymour, CEO Nanoviricides, Inc.
Since Ebola and ERASMUS are linked in the news, I wonder if Dr S decided to dust off some of that 6-8 year old Ebolacide that our govt wasnt interested in, throw a couple of vials in his shaveing kit and demo with them this week??? If we got the 'cides and they have the credibility it might just lead to something big, unexpected, and soon. Wouldnt that be fun!
lousy engineer, not exactly what I had in mind. I think that the company that designs/produces cutting-edge nano-technology equipment/instruments for NanoViricides, Inc. are likely working/collaborating on a 3D-nano printer for NanoViricides, Inc.---Just speculating! The "ink cartridges" for this 3D nano-printer?
FluCide is made up of PEG backbone, pendant fatty acids and ligands...~ robi-1-kenobi
Yesterday is still a bit of a blur, but I can say that I did meet Donnie Liverman from the Virginia-based Old World Laboratories (OWL) and saw the OWL Nano™ in real life at CES. The OWL Nano is the newest stereolithography (SL) 3D printer on the market and what it boasts over its competitors, like the FSL3D Pegasus Touch or the FormLabs Form1, is its nanoscale resolution.
 source: http://3dprintingindustry.com/2014/01/10/owl-nano-stereolithography-1-microns/
source: http://3dprintingindustry.com/2014/01/10/owl-nano-stereolithography-1-microns/ Radical Abundance: How a Revolution in Nanotechnology Will Change Civilization by K. Eric Drexler
K. Eric Drexler is the founding father of nanotechnology—the science of engineering on a molecular level. In Radical Abundance, he shows how rapid scientific progress is about to change our world. Thanks to atomically precise manufacturing, we will soon have the power to produce radically more of what people want, and at a lower cost. The result will shake the very foundations of our economy and environment.
Already, scientists have constructed prototypes for circuit boards built of millions of precisely arranged atoms. The advent of this kind of atomic precision promises to change the way we make things—cleanly, inexpensively, and on a global scale. It allows us to imagine a world where solar arrays cost no more than cardboard and aluminum foil, and laptops cost about the same.
A provocative tour of cutting edge science and its implications by the field’s founder and master, Radical Abundance offers a mind-expanding vision of a world hurtling toward an unexpected future.
I read a post a few days ago (I should be bookmarking them, but I'm not) that contained an email/excerpt from Dr. Seymour with a list of the different entities the NanoViricides, Inc. (or TheraCour) R&D lab is currently supplying, with what I think is GLP material. Among several lab-supplied entities was Dr. Eva Harris/Berkley lab.
Dr. Harris is one of the world’s leading experts in dengue. This contract renewal will allow the Company to continue its drug development program for the treatment of dengue.
There is currently neither an effective drug treatment nor a vaccine for dengue virus infection. The FDA has recently awarded orphan drug status to DengueCide and the Company is pursuing similar status with the European Medicines Agency (EMA). The orphan designation enables the Company to undertake rapid drug development following its influenza drug candidates.
About Dr. Eva Harris’ Laboratory at the University of California, Berkeley
The Harris Laboratory in the Division of Infectious Diseases in the School of Public Health at the University of California, Berkeley (www.berkeley.edu) has developed a multidisciplinary approach to study the molecular virology, pathogenesis, immunology, and epidemiology of dengue, the most prevalent mosquito-borne viral disease in humans. Their work addresses viral and host factors that modulate disease severity as well as immune correlates of protection. One major research focus has been the development of a mouse model to study viral tropism and pathogenesis, investigate the immune response to dengue virus infection, and evaluate candidate anti-viral therapeutics. Dr. Harris’ field work focuses on laboratory-based and epidemiological studies of dengue in endemic Latin American countries, particularly in Nicaragua, where ongoing projects include clinical and biological studies of severe dengue, a pediatric cohort study of dengue and influenza transmission in Managua, and a project on evidence-based, community-derived interventions for prevention of dengue via control of its mosquito vector.The market size for anti-influenza drugs is currently estimated to be in several billions of dollars worldwide. The Company believes that if its FluCide® drug becomes available, the influenza drug market size could become substantially larger. It is well known that when an effective treatment for a disease becomes available, the market size explodes and the novel effective treatment captures a substantial portion of the market.
Scale up studies are studies to ensure that when you up-scale or go from a smaller concentrations of formula or batches to larger batches that they remain as close to identical, or to the prototype originally produced in lab, as possible. You go from lab, to the pilot lab and finally to production lab. An easier way to describe it is going from a small pot of formula to a much larger pot and the formula must stay the same...so the more the scale up, the more the chance of a mistake could multiply. A very small mistake can produce extreme differences in forumla. Scale up is going from lab to production state. Critical variables to be considered are things like batch size, energy requirements, equipment capabilities, acids, bases and temperature to name a few. This may take some trial and error at first as very minor mistakes can really be detrimental; Especially in Anti-Virals. If they have found a formula that works like they claim, then this scale up process is the difference between success and failure. These tests should be on production plant. ~ gizmo_puppy95
GLP material can be used up to Phase 1 trials. GLP can be made to GLP-like material standards. Scale-up in existing lab space includes specialized larger lab equipment capable of producing 1 kg batches rather than 10 gram (might be a little larger than that). That's two orders of magnitude larger and the new pilot facility I understand will 5 times the retooled space (possibly 10).
At 10-20 gm batches it took a long time to manufactured enough material for maximum feasable dose studies as well as reach an LD10 standard. That's enough material to blow up 1 in ten mice in the test group.
I might be wrong or misremember, but I recall 3 days per batch (though might be 5 including cleaning and prep time between batches) in a quasi-assembly line of mixing and cooking. Anyone who followed Breaking Bad has an idea of the sort of larger scale apparatus that will eventually be in place in the new lab, and an idea of the smaller scale in the current space if one recalls the equipment in that first mobile lab. ~ Big Kahuna
Only partly true. Scale up is a problem faced by EVERY drug company. There are many factors that are strongly affected by change in scale (for example an exothermic reaction at lab scale may require no measures at all to get rid of the excess heat generated but in a 1,000 liter biofermentation vessel may require extensive measures to remove heat).
BUT there are some unusual considerations that apply to NNVC"s scaleup so you do have a point. Their products are micelles which have inherently far more variability than almost all other biotech products and scale up can have effects on that.
BUT it's also true that many, possibly most, biotechs have some similarly unusual problem that they have to deal with at some point.
There IS an usual ("unique'is an overstatement: other companies use micelles as well) aspect to NNVC's scale up but having some unusual characteristic is far more the norm than the exception.~ Zincfinger
There is no need to ask Dr. Seymour frivolous questions from naysayers about GLP, cGMP, cGMP-like!
The question that should be present in everyone's mind is, if GLP and cGMP are equivalent, if FluCide (or any other nanoviricide(R)) are low-toxicity and effective regardless if the path is GLP or GMP, why not allow it to take the fastest path/means to the clinical trials and save as many lives as possible? Let's show some more flexibility! Reimburse some of the costs (50% or more) incurred by NanoViricides, Inc. to bring life-saving drugs to the market. Our government has done it before for far less worthy causes.
The question(s) should be directed to:
1- The FDA
2- Your state U.S. Senator/U.S. Representative (science, technology, healthcare committees)
3- Every time you see a report/news on viruses taking human life, write to your local broadcaster and tip them about NanoViricides, Inc. life-saving therapeutic drugs
The GLPs are designed to protect scientific data integrity, and to provide EPA or FDA with a clear and auditable record of open-ended research studies. In contrast, the GMPs are intended to demonstrate to FDA whether or not individual batches of a regulated product are manufactured according to pre-defined manufacturing criteria.
lousyengineer, thanks for pointing the board to the excellent article! I think the machine behind Dr. Anil Diwan (R&D lab)is one of the main components of cutting-edge nanotechnology machine(s) that manufactures the low-toxicity, life-saving nanoviricides(R). The new machine must be larger, 5kg capacity, soon to be operating at the new cGMP Pilot Plant.
It seems you missed the thrust of my post. People posting here are trying to demean the formal education of the NanoViricides, Inc. 'the company'. CEO and that of the inventor(s) of nanoviricides(R).
How about you going on your proposed "wild goose chase" and demonstrate why it is not a fundamental patent? After all, who is challenging NanoViricides, Inc. claim of a fundamental patent?
NanoViricides, Inc. is on the cutting edge of nano-technology.
“By 2011, when Dr. Diwan went all out and bought the Controls Drive property, we had spent several years searching for a third party contract manufacturer, capable of producing our drug candidates under the rigorous standards required for clinical trials, without success,” said Eugene Seymour, MD, MPH, adding, “NanoViricides continued to search for available contract manufacturing capability even after Diwan’s purchase of the Controls Drive property. Most facilities we interviewed could not manufacture our novel polymer molecules without extensive renovations. The cost of such custom renovations and equipment would be passed on to us, as is customary. In addition, we would have to train their technicians and scientists and transfer important know how and other aspects of our intellectual property.”

