 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.



WeeZuhl
![]()
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
No new patent on the new formulation? I am surprised they don't have one if it really is that good...though would suspect that because they have been able to keep it to themselves, no need to disclose at this point, so that may not be an issue at all. Still, I would have still expected to see a patent at this point to ensure ownership exclusivity.
Can you share any details on the unique abuse deterrent formulations without SequestOx’s of Naltrexone that was included in the pilot study?
No, except to say, I am extremely excited about this formulation because it also is a platform that apply to all the IRs and it happened to be about maybe 10% of the cost. So we're extremely excited about this, but it's still too early in the next few months. Once Dr. Smith files a patent and we do a little more trials, we’ll update a little more about it.
Hahaha wow!!
Kempharm's studies show that there is a decrease in plasma concentration when *EIGHT* (8!!!) tablets are taken. In other words, not much help
I thought preventing dead by lowering the concentration in plasma was good... I guess I was wrong ;)
Pro-drugs are cute but not abuse deterrent
Example: KemPharm's Apadaz (prodrug of Norco). Received FDA approval last week after initially getting CRL due to lack of snorting abuse-resistance. As far as I can tell, the approval was given without any modification, but there is no ADF label. Unless they can figure out a market niche for a very expensive version of Norco without an ADF label, all they have is a new Oxaydo (no commercial viability).
Like most pro-drugs, Apadaz has some inherent overdose protection. Kempharm's studies show that there is a decrease in plasma concentration when *EIGHT* (8!!!) tablets are taken. In other words, not much help. Prodrugs are very finicky. Don't believe anything you hear until the data is available to prove it.
But, hey, why not accumulate for a few more years?
the seven year issue that was long ago resolved? ok got it
- What are those 'questionable' effects of Targiniq?
the pharmacodynamics of naloxone is certainly different as it is metabolised faster and bioavalability is variable, however, the abuse-deterrence of this antagonist still works.
'Abuse-Deterrent' Label Panned for New Opioid
by Kristina Fiore, Staff Writer, MedPage Today
July 24, 2014
The FDA has approved another abuse-deterrent opioid, although addiction experts said the drug can still be easily abused. The agency cautioned that the long-acting, extended-release opioid can still be abused if chewed and swallowed.
"Targiniq ER can still be abused, including when taken orally, which is currently the most common way oxycodone is abused," the agency noted in its press release.
That's because of the way naloxone is processed when taken orally, said David Juurlink, MD, PhD, a medical toxicologist at the University of Toronto. It can exert its effects on opioid receptors in the brain if injected into the bloodstream or taken intranasally. But when ingested, it's not absorbed well.
Chewing and swallowing will thus enable abusers to get the full 12-hour oxycodone dose all at once, said Andrew Kolodny, MD, chief medical officer of Phoenix House, a substance abuse rehabilitation program.
"This product is obviously inferior to OxyContin and should certainly not be labeled abuse-deterrent," Kolodny said. (Purdue Pharma also makes OxyContin.)
Lewis Nelson, MD, a medical toxicologist at NYU Langone Medical Center, noted that other opioid products containing naloxone, such as the addiction treatment Suboxone (a combination of buprenorphine and naloxone), have been subject to abuse "so the underlying assumption that adding naloxone to an opioid completely prevents abuse is potentially misguided."
"Since most abuse and overdose occurs through ingestion, and since this combination provides no risk reduction when taken by that route, it seems that adding the abuse-deterrent moniker is premature," Nelson said.
Addiction experts noted that the agency approved Targiniq without consulting an advisory committee, basing its approval instead on its review of the results of a trial involving 601 patients with chronic lower back pain.
"There's no justification for approving the drug without an advisory committee meeting considering how controversial the topic is," Kolodny said. "I'm almost certain an advisory committee would have voted this product down."
Now, regarding naltrexone and withdrawal symptoms... I'm sorry to say, but that is not caused by small amounts of naltrexone and certainly not by 'leakage'... that is the effect caused by manipulating these formulations and releasing either naloxone or naltrexone... and in fact, it is one of the main concerns among clinicians regarding these approach (opioid/antagonist) that abusers may suffer from severe withdrawal symptoms if they manipulate the formulations
Opioid withdrawal symptoms:
Pain areas: in the muscles
Gastrointestinal: diarrhea, vomiting, or nausea
Whole body: restlessness or sweating
Mood: general discontent or anxiety
Eyes: dilated pupil or watery eyes
Also common: cramping abdominal pain, fast heart rate, excessive yawning, goose bumps, insomnia, or tremors
More naltrexone should not be necessary... the concentration ratio of agonist/antagonist sufficient to block the euphoria induced by opioids is well know and it is what the current formulations use and any formulation scientist with good knowledge would use.
High concentrations of naltrexone in circulation also have effects on liver and kidneys, as it is metabolised slower and excretion takes longer.
2011 ???? lol old old news
dr_lowenstein Tuesday, 02/20/18 03:30:30 PM
Re: WeeZuhl
Post # 284273 of 284313
Really???? Got any evidence to support that old nonsense about embeda? Sheeeeze
dr_lowenstein Tuesday, 02/20/18 06:10:28 PM
Re: WeeZuhl
Post # 284298 of 284313
none of the links support anything about embeda instability
none of the links support anything about embeda instability
MARKET NEWSMARCH 16, 2011
Pfizer recalls pain drug acquired in King deal
Ransdell Pierson
Embeda, which has annual sales of less than $70 million, was recalled in the United States because of a stability defect found in the extended-release product during routine testing, according to a notice posted Wednesday on the drug’s website, Embeda.com.
The drug contains pellets of morphine that surround naltrexone, a chemical which blocks opiate effects if the product is crushed or chewed -- thereby deterring misuse or abuse. The naltrexone component was shown to have degraded to unacceptable degrees in samples of Embeda that were tested, Pfizer said. The problem is unlikely to pose a safety risk and patients can continue taking the drug as prescribed, the drugmaker said.
Embeda, approved by U.S. regulators in August 2009, was recalled three times last year due to other formulation problems, all relating to how it dissolves, Pfizer spokeswoman Joan Campion said.
REPOST DEAR WEEZUHL 2/1/17
Dear WeeZuhl,
Ever since ADF OxyContin was released, I have been injecting heroin on a daily basis. I have a job and can support my habit, and I have plenty of experience and know my limits. But they don’t sell the stuff at McDonald’s, and I cannot always get it from a safe, reliable source. Now there is an epidemic of heroin overdose deaths because of unknowingly using heroin that has been laced with much more powerful and deadly fentanyl. Today my pharmacist told me the naloxone injector I carry to prevent opioid overdose will cost $4500 instead of $700. What should I do?
Signed,
Priced Out of Overdose Protection
Jan 31, 2017
Kaleo Hikes Price Of Opioid Overdose Antidote Evzio From $690 To $4,500
But here we are again—now with Kaleo’s novel handheld talking auto-injector Evzio, designed to reverse opioid overdoses, increasing in price from $690 in 2014 to $4,500 in 2017, according to a recent report by Kaiser Health News.
You should get updated data ;)
Here it is:
Embeda had issues with naltrexone leakage back in 2010-2011... it was then discontinued voluntarily by Pfizer (Pfizer acquired Kings/Alpharma in 2011)... it was then reformulated to fix the issue and the new formulation with NO leakage was re-approved in 2014, when it was also awarded the abuse-deterrent label by FDA
Really???? Got any evidence to support that old nonsense about embeda? Sheeeeze
Embeda has stability issues because the naltrexone is within the core and very difficult to fully sequester. The designers were forced to limit the amount of naltrexone in each tablet because of the leakage, which will cause withdrawal symptoms in legitimate users. More naltrexone means more symptoms in legit users. Less naltrexone means more potential for abuse.

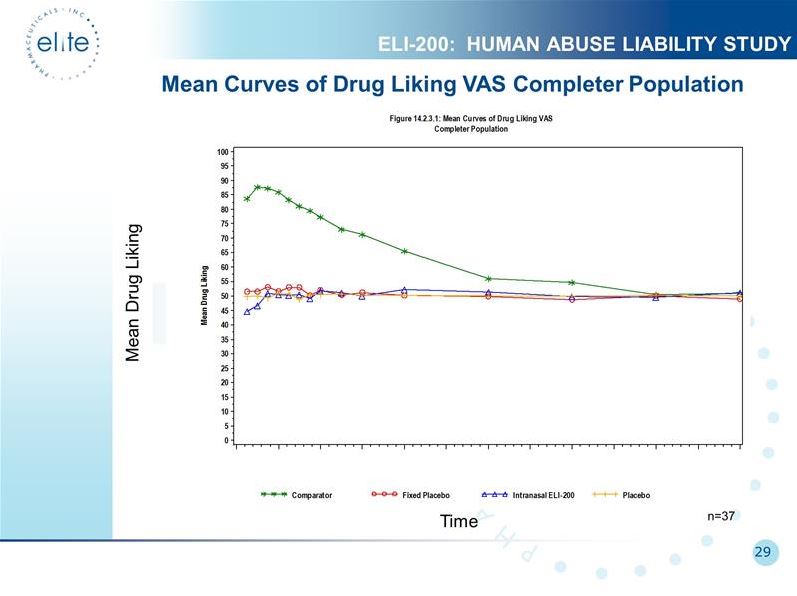
Naltrexone HCl 4.8 mg co-administration resulted in ≥30%
reduction in morphine-induced euphoria for >50% of subjects who completed the study, assessed
by VAS-Drug Liking. This degree of reduction in morphine drug liking mitigated by naltrexone
HCl would be expected to reduce morphine abuse potential.
You may get that .09 or lower. RSI is at 43---lots of room to the downside before it gets into rebuy territory (RSI under 30).
Can you just enlighten us on how it works better than the competition?
How does it compare to other Opioid/Antagonist ADFs such as Targiniq ER, Embeda, Hysingla ER, Troxyca ER ?
Thanks :)
Still, more than 10 years and nothing approved
Elite started an ADF company multiple years before OxyContin came out. It would be nine more years until the movie OxyContin Express won the Peabody for documenting the craziness in Florida. By then, Elite had been less than a dime for nearly two years. ADF OxyContin didn't come out until 2010, and before that nobody ever heard of an ADF label. A lot has changed since then. We have a whole new language for describing ADF properties, testing for effectiveness, and certifying the label. My bet here is that it is worth something to have a unique ADF tech that can readily meet the requirements for chewing, snorting, and IV abuse deterrence labels for any opioid agonist and any time-release characteristic (even if it isn't first and isn't revolutionary). I own about one in 500 share of this very cool, very versatile ADF tech, and I'm very much looking forward to seeing how it turns out. Patience, my friend.
Still, more than 10 years and nothing approved, no other companies approached Elite to use their technology, interest in the company is only strong in this forum
if this technology works, the preliminary results would be out already, but it has been more than 10 years and nothing
if this technology works, the preliminary results would be out already, but it has been more than 10 years and nothing


The judge didn't sided with Pfizer, because the litigation was dismissed by both parties... in fact, if anything, it was in favour of Watson because the litigation was dismissed with 'prejudice', which means Pfizer cannot sue Watson again for this.
Maybe if you read more about this deals you would realise how this works, because Watson/Actavis/Teva are the manufacturers of Embeda for Pfizer, they are and have been for the last 8 years, so the deal just brings money to Teva while they pursue their ANDA.
If you haven't seen an approval yet it is because Embeda was discontinued in 2011 until 2015, then it got its AD label in 2015... so other things happen thru these years that delayed any Gx Embeda
and as a note for all of those who wonder why there are no Gx ADFs yet, it is because FDA is waiting for the post-marketing studies from the current branded ADF to prove they work before they go and approve generics ;)
One of the factors that the FDA would consider relates to generic access. We must have the potential to improve access to the newer formulations, for appropriately selected and monitored patients, through the introduction of generic competitors.
In order to support this transition and encourage advancements in this area, today the FDA issued a final guidance to assist industry in their development of generic versions of approved ADF opioids.
General Principles for Evaluating the Abuse Deterrence of Generic Solid Oral Opioid Drug Products
Guidance for Industry
November 2017
As a matter of fact, the litigation was settled by both parties as they reached an agreement (you can see this in the litigation history), additionally, in 2016 (during an investors presentation) Teva presented Embeda as a product they had confidentially settled and would be launching when exclusivity ends.
Not that interesting, it is a well known fact that Watson (now Teva) filed for Gx Embeda back in 2011, and so far they are the only ones.
and with the exclusivity expired the approval can happen any time
In a one page order, Judge Andrews adopted plaintiffs’ proposed construction, construing the term “sequestering subunit” to mean “Any means for containing an aversive agent and preventing or substantially preventing the release thereof in the gastrointestinal tract when intact, i.e., when not tampered with.”
They should just buy the ANDA that their good friend Epic already has ;)
If Elite's filing hasnt been sued/under litigation, it may indicate that they filed thru paragraph 3, as Oxycontin still has one patent that prevents ANDAs approvals.
so if Elite filed thru Para 3, that means they won't launch until 2025, when the remaining patent expires
otherwise generics face much more competition and price disadvantage than branded products... even with generics in the market branded products can retain a significantly profitable price and a considerable market share
Smart pharma companies do not rely on their "pending" products to play with their stock price, but instead in having an attractive and constantly evolving R&D pipeline to attract new and big investors.
Elite's attractive selling point was (WAS) their dual bead (opioid/ant) system, however they haven't learn how to exploit it and as I said before, by the time any of these get approved it will be obsolete.
I am extremely excited about this formulation because it also is a platform that apply to all the IRs and it happened to be about maybe 10% of the cost. So we're extremely excited about this, but it's still too early in the next few months. Once Dr. Smith files a patent and we do a little more trials, we’ll update a little more about it.
CC Question
Elite's generic Oxycontin ANDA was submitted on Sept 20, 2017. Has the application been accepted for review by FDA? If so, has Purdue been given Paragraph IV notification? If so, when was it given and has there been any official or unofficial response from Purdue? Are there any human abuse liability studies that have been done yet or are scheduled to be done for Elite's generic version of OxyContin?
Don't forget PODRAS is totally useless to prevent oral abuse or suicide, even if it works as is intended, which it won't.
lmfao!!!
Q:How do you abuse any drug with PODRAS?
Q:How do you kill yourself despite PODRAS?
I stand corrected.
In fact your own follow up statement you're using as proof doesn't even say "chewed like bubblegum" it clearly states "become like bubblegum" oops!!!
BTW, don't forget that Dr. Odidi himself said Rexista can be "chewed like bubblegum."
BTW, don't forget that Dr. Odidi himself said Rexista can be chewed "like bubblegum."
Nobody still here has lost 1 dime WeeZuhl...
also your 2nd paragraph about the removal of the blue dye being the only oral abuse deterrent in regards to chewing is bs...and where did Dr. Odidi supposedly ever say that Rexista could be chewed like bubblegum? That's a bs claim to>>>
What we have designed makes it so that, yes you can go ahead and crush the tablet, however if you crush the tablet, all the moisture content will suddenly gel… they form a very strong gel and become like bubblegum, therefore, you can’t snort them and you can’t dissolve them to inject them. That’s what we’ve done, that’s the area we’ve gone into.
Well now, that was interesting thing to say. Rexista can be readily crushed (and therefore chewed). I always thought the blue dye #1 was a superfluous add-on marketing gimmick in order to differentiate Rexista from the other physiochemical oxycodone ADF's. But apparently the blue dye is a necessary add-on due to Rexista's lack of crush-resistance. That's a problem not even I anticipated. Just wow. Now we know why the HAL studies are top-secret. LOL, Rexista is "like bubblegum." Delicious, delicious bubblegum. Spearmint my ass, where's the Rexista??
Physico-chemical studies suggest that Rexista™ oxycodone:
should be difficult to abuse through crushing, chewing or licking
release of oxycodone is likely to be slower or not instantaneous in a range of beverages and solvents (Ed. Note: does not prevent chewing)
should not "dose dump", or instantaneously release the entire dose of oxycodone, in the presence of ethanol over a range of concentrations (Ed. Note: does not prevent chewing)
when pulverized and reduced to particles, should be difficult and time consuming to syringe or inject in the form and volume suitable for intravenous administration (Ed. Note: does not prevent chewing)
when pulverized or reduced to particles, should be difficult or inefficient to snort or inhale (Ed. Note: does not prevent chewing)
release of oxycodone should be insignificant or inefficient via heating and vaporization (Ed. Note: does not prevent chewing)
extraction of oxycodone which has been microwaved should be difficult or inefficient
(Ed. Note: does not prevent chewing)
Results from accelerated stability studies indicate that the Rexista™ oxycodone formulation is stable even at a high temperature (40°C) and relative humidity (70%) of storage. (Ed. Note: does not prevent chewing)

Based on the meeting, the product candidate will no longer include the blue dye.
“The FDA approval of the sNDA is a major milestone for Collegium. With the addition of comparative pharmacokinetic data with OxyContin and an oral abuse deterrent claim, Xtampza ER is the only single agent oxycodone with oral, intranasal and intravenous abuse deterrent labelling,” said Michael Heffernan, CEO of Collegium.
its going down FASTTTT better SELL
I just post the facts RED 3days what=u-want-me-to-say-its-green

Welcome Winechemist.
The test products included two formulation modifications of SequestOx, a unique abuse-deterrent formulation without sequestered naltrexone, and a reference product.
I am wondering what this formulation could be, this seems very interesting.
Elite Pharmaceuticals, Inc. ("Elite" or the "Company") (OTCBB:ELTP) today reported positive topline results from a pilot study conducted for SequestOx™, Elite's immediate release Oxycodone Hydrochloride product that incorporates its proprietary abuse-deterrent technology.
SequestOx is Elite's investigational abuse-deterrent immediate-release oxycodone product with sequestered naltrexone for the management of moderate to severe acute pain where the use of an opioid analgesic is appropriate. The study was a Phase 1 pilot, randomized, single-dose, single period, pharmacokinetic study in healthy male and female volunteers in the fed state. The test products included two formulation modifications of SequestOx, a unique abuse-deterrent formulation without sequestered naltrexone, and a reference product. The following table summarizes the Tmax results for the pilot study.
Nailed it!
SequestOx Tmax
Treatment-----N---median---min---max
Reference-----12---2.25---1.28---5.00
Test-A----------12---2.5-----1.25---5.00
Thanks steadyhand. Good eye.
The figure you cite is better than 3D cell culture (which is a pretty tacky method). The figure you cite is from an orthotopic mouse model (tumor model). Notice the Y axis is tumor weight in grams.


Reasonable question.
The reason I say all of this is because I don't see how you can you simulate the mechanism of action in a 2D or 3D culture environment. Prolanta works via autaphagy as a result of human prolactin receptors (hPRL) being antagonized. How could a 2D or 3D culture possibly create a scenario that involves hPRL receptors? Prolanta is fighting cancer in an indirect manner.



Prolanta is fighting cancer in an indirect manner.
Recent studies have shown that levels of PRL were substantially
elevated in ovarian cancer patients and concomitantly
enhanced proliferation, migration, and invasion and promoted
tumor angiogenesis (Asai-Sato et al., 2005; Levina et al., 2009).
Our results indicate that antagonism of PRL/PRLR axis enriched
late-stage autophagic vacuoles in cancer cells cultured in 3D
conditions, which led to programmed cell death. This might
explain the robust inhibitory effects of G129R on tumor growth
that we observed in vivo, but not in 2D cultured cancer cells.
Yes.
is Vyvanase an extended release product?
Sorry, I should have been more specific.
yeah, probably crestor. what, about 30 companies already w approved generics, wow, this is a real blockbuster LOL no wonder they didnt disclose
and the attention-deficit drug lisdexamfetamine dimesylate (Vyvanse, Shire), at about 10.6 million.
what is the undisclosed drug in today's news?
Through June of this year, the cholesterol-lowering drug rosuvastatin (Crestor, AstraZeneca) was the most prescribed branded drug in the United States, and the arthritis drug adalimumab (Humira, Abbott Laboratories) was the best-selling branded drug, according to the latest data from research firm IMS Health.
Rosuvastatin had about 21 million prescriptions, followed by asthma medication fluticasone propionate/salmeterol (Advair Diskus, GlaxoSmithKline), at about 13.6 million prescriptions; the proton pump inhibitor esomeprazole (Nexium, AstraZeneca), at about 13.2 million prescriptions; the insulin glargine injection Lantus Solostar (sanofi-aventis), at about 11.2 million; and the attention-deficit drug lisdexamfetamine dimesylate (Vyvanse, Shire), at about 10.6 million.
Is today opposite day?
Funny thing is, "progressing" was my word choice that I decided to use when paraphrasing our conversation. She actually said that all of the patients were "improving". I forgot that in the world of cancer 'progress' is a negative word as in the cancer is progressing to a worse state. You obviously knew I was trying to say though.
Are you thinking of the word "regression"? LMFAO
"Progression" is bad.
I asked her about the efficacy of the drug, and she told me that every patient that was tested had progressed with their conditions and it's a shame that they had to stop the trials.
...
All in all, I would say it was a positive phone call and is in line with a lot of what we already knew. It sure made me feel good to hear her say that ALL of the patients were progressing.
Nah...take .09 and run. Nobody cares.
During the last cc they mentioned they had 30 days to respond to FDA on Perc and Norco. I assume Sungen product got delayed. I am ASSUMING they responded in time. Nasrat clearly mentioned that if they didn’t respond timely they would have to get in the back of the line...
Let me try this into our pending applications to-date. We have filed four ANDAs, Oxy APAP, Hydro APAP, non-disclosed and OXY ER. We received a complete response letter that defined exactly what more does the FDA want. The requirements range from, A, make a commitment that you can comply with elemental analysis which will become the law of the ANDA in 2018. We did. Provide the additional testing for certain things. We did. Do a micro on the specific things. We did. We just filed our response to FDA’s complete response letter for OXY APAP and we will file the response to Hydro APAP hopefully within the next couple of months.
FDA has hardly asked a single question about the undisclosed application the last night. Late p.m. yesterday they sent us the inquiry asking a host of questions and gave us 30 days to answer them. We have not received any inquiries yet on Oxy ER.
Just to put things in perspective for you. During Q4 of this year, in addition to having to prepare to file and we will file the SunGen application in December of this year. In addition to that, we have to response to the FDA for Oxy APAP. We are responding for Hydro APAP and we are responding for our undisclosed, all within couple of months, that’s a huge burden on the staff especially when the FDA give this specific time you get to respond in 30 days or you are in the back of the line, okay. So we are doing a lot of work in here and this is why it takes a little bit of time to put the response together and sent it to FDA.

