 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.





Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
early but TSLA losing the battle so far versus nwbo
Less did you ever go long? I can’t recall, but I thought you’d posted you were going to get long? Change your mind? Or Did Gro persuade you to buy?
holy batman bullshit. complete bullshit. first, old endpoints. Second, you are referencing the FUTURE RISK FACTORS section.
Killing on TSLA? The real money has already been made. With the Fed hell-bent on QT and preventing a 1929 type depression, those $60-100k vehicles will look a lot less attractive. The Fed hasn't even begun to unwind its balance sheet, but expect this to pick-up pace soon. A recession is staring us smack-dab in the face (some people are too "blind" to see it), and along with this lower crude and gas prices which will make gas cars and trucks much more attractive again. Crude prices ersion began about 2 months ago, gas will catch up pretty soon. Tesla is a highly leveraged company and sales rely on a good economy (discretionary spending,etc) to do well. While I 100% believe in Tesla long-term, and was a early investor in 2013, I think a it's got another 20-40% drop coming as its still overpriced vs earnings. Be careful.
-Fireman
some might try to make it sound like there is some limited upside but when you have a product to treat all solid tumors in your pipeline there is no ceiling
great stuff meirluc
Someday clinical trial confounding would be actually understood by investors. As NWBO declared their primary endpoint confounded and tossed it out, they recognize the issues of confounding. But they are still using naive OS data, even though they also declared the data as confounded. They admit they are doing it at risk of regulatory rejection. But clearly NWBO investors do not understand the risk of regulatory rejection.
There is a glass ceiling and the longer NWBO drags this out and diluted shareholders the lower the ceiling and the lower the payout, especially in light gave how long many shareholders have been here buying and holding.
It will be bittersweet when and if this ends in a positive way - sweet because most shareholders will be back in the green but bitter when the dreams of 20 baggers (from here) etc. are dashed by the sheer depth of the hole we are climbing out of to get to that ceiling.
It seems to me that the crossed over patients are demonstrating that if the vaccine is of maximum benefit to a given patient it's delay isn't terribly harmful. I'm not suggesting that there is a benefit, but if the demand for DCVax-L at first is substantial as production is being ramped up, patients can still get a major benefit which in some cases may prove to be curative.
Hopefully agencies like the FDA won't hold up approval waiting for more capacity to come on line, but in the beginning I suspect that the immediate demand will outstrip the ability to deliver the vaccine immediately, patients may need to wait a few months to get theirs.
Gary
Remember the King and Odie cartoons from the early 1960s? Maybe it was before your time, but King Leonardo used to say "Confound It" a lot, and whenever you say confound, I stop reading and I go right back to that cartoon. Thanks for the memories, but I never get what you are trying to say. Nor does anyone else.
NWBO stock is down >92% since LP became CEO, I will update and repeat this weekly until she is fired and replaced. She is horrible as a CEO!
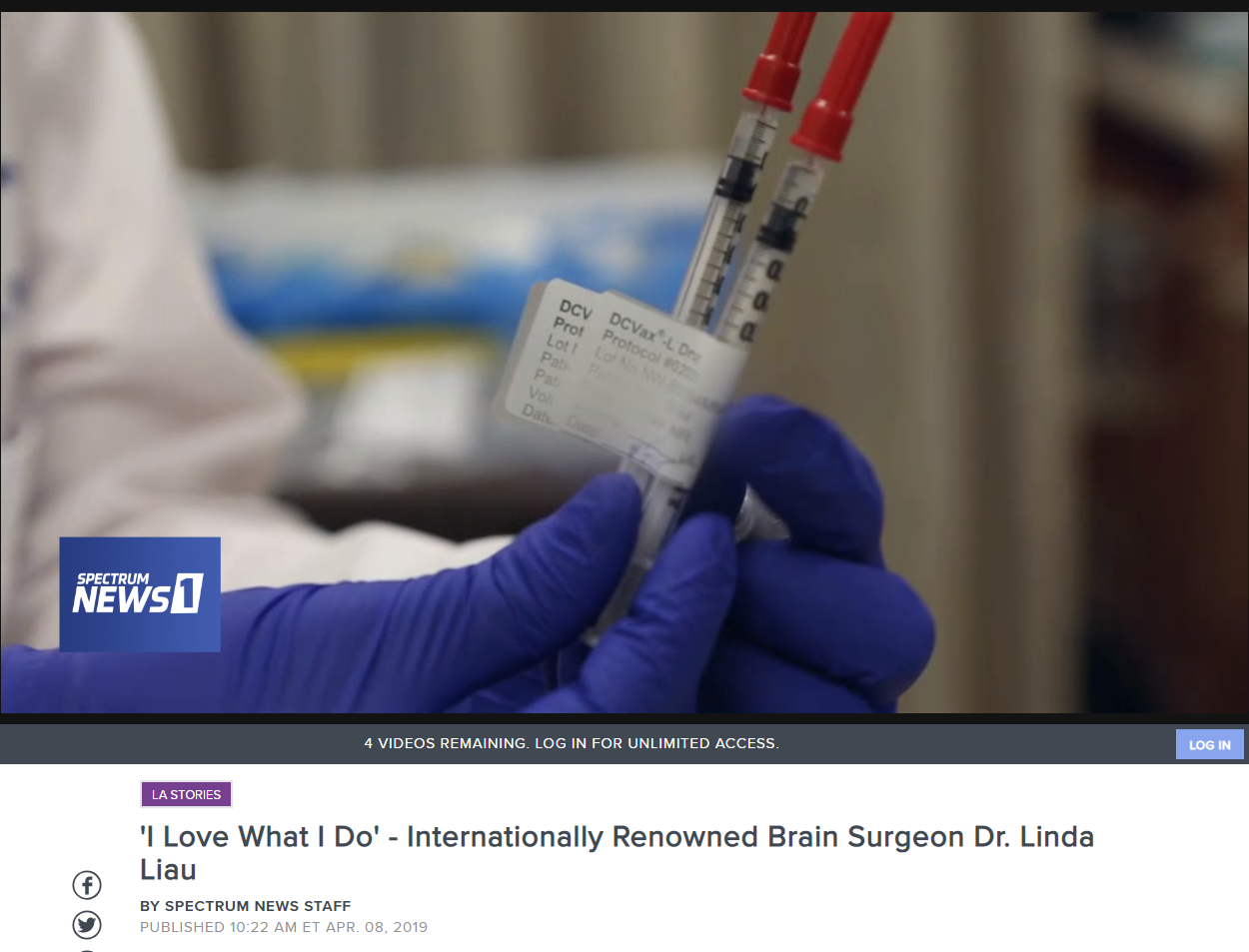
Anyone have a video of Linda Liau's Prague presentation?
Thanks Meirluc for the commentary.
Hopeforthefuture, prior to May 10 many of us believed that almost all the benefits of the increased survival times that were calculated from the 2018 JTM and SNO update data, were due to the appreciable increased survival capacity of the treatment group whereas not much benefit was envisioned to emerge from the crossovers.
The NYAS presentation clarified that the survival benefits are distributed between both the treatment and crossover groups The survival results of the Treatment patients though much better than those displayed by the ECAs are somewhat less than the spectacular results that we predicted, but the survival stats of the crossover group are spectacular and that I for one never expected.
I will take the appreciable success of the treatment group and the unexpected, remarkable success of the crossovers over a a spectacular success of the treatment group and no appreciable benefit for the crossovers. I am guessing that there is a reason that the NYAS, UK and Prague presentations have not as yet shown us the K-M survival graph of the crossovers. I have a feeling it is the most impressive part of the trial and is therefore reserved for the JA.
Also please take notice of another previously uncertain benefit.
Although the mOS of the unmethylated treatment patients was only minimally longer than the mOS of the matched ECAs, a number of those patients demonstrated an increased survival capacity and 8 of the 131 unmethylated treatment patients (6.1%) became post 5 year survivors. Prior to the last three presentations, I was not confident that the regulators would approve the use of DCVax-L for patients with the unmethylated GBM. Now I am much more optimistic that the approvals will cover all GBM patients and am hopeful that the unmethylated GBM patients in the crossover group will also demonstrate that they derived appreciable survival benefits from the vaccine.
there is no ceiling on where this can go.
In my personal opinion we're sitting on a goldmine. If people understood that they might not complain so much about the price as it is today.
repeated bullshit. old endpoints and you are citing the future risk factors and mistaken them as facts
are you assuming "in the process of approval" means accepted MAA?
Yes, I think the next PR will be that MHRA has accepted the MAA application for DCVax marketing approval in UK. They can PR the manufacturing approval when they PR that MHRA approved DCVax as these go together.
As evidently the NWBO SEC filing outlining the confounding issue was missed, here's the key section:
"Under the Protocol the primary endpoint was progression free survival, or PFS, and the secondary endpoint was overall survival, or OS. Both of these endpoints were confounded: the PFS endpoint by pseudo-progression, and the OS endpoint by the “crossover” provision in the trial design, which allowed all of the patients in the trial to cross over to DCVax-L treatment after tumor recurrence (while remaining blinded as to which treatment they received before tumor recurrence). The statistical analysis plan uses external control patients rather than within-study controls. There can be no assurance that regulatory authorities will allow a product approval to be based upon this approach."
Anyone who compares Vascepa, a concentrated version of fish oil, with DCVax really has no clue.
Commercial manufacturing cert. cannot occur before MAA submission/acceptance. Thanks anyway.
Hoffman thank you for answering the question.
As for the 13% yes it is better but I rationalized it taking longer than expected for my coworker in that even if he received dcvax he still had an 87% chance of not getting to long term survival.
This is also something have to consider when thinking of having to self pay in the specials program - chances are better 13% vs 5or6% but do I spend that $ knowing chances are still not very good for a cure (87%) or do I leave the $ to help the family after I'm gone
Another poster had this same question.
Once insurance covers it then of course get the vaccine
OTC is a challenging exchange to be on. After 5/10 retail has to be spooked. SP seems at the whim of manipulators, who are not being dealt with, for whatever reason. Same ol’ same ol’.
You are arguing that a top notch journal will time a publication with a company commercial manufacturing milestone? I don't buy it. Please provide the context of Dr. Musella's quote and a link. I usually agree with everything that comes from Dr. Musella.
As far as the next milestone announcement, you might be right. I have no idea. It would be pure speculation in this regard. It might be the full MAA submission. It might be a JA. It could be commercial manufacturing certification. Maybe BLA related. Or maybe, just the ASM date. Who knows.
Thanks Flipper.
No, they’d have that done by now. That’s old news. I prefer to look at Dr. Musella’s reasoning for why this is kept under the radar for now. My guess is next milestone announced promptly will be MAA acceptance (possibly submission announcement prior because it is also a milestone.)
Keytruda failed with GBM but unlikely that a subcutaneous jab would be a better route for every new cancer. And as I said, they likely chose the initially best route for Keytruda from the start. This is a work around and it may not work as well as the current method, but more importantly, that work around is just a patent on a specific delivery method and would not be a barrier to entry for generics in already approved indications.
As for a DCVax-L and PDL/PDL1 combination, that will be what the combination patent should facilitate. And it could work with any of those drugs and all. It would be better if they were able to get multiple deals for different versions and some versions may be better than other.
Heck, a combo with a subcutaneous version as well.
I think it’s just the beginning as the poly ICLC arms suggest and yes, with significance as per Linda Liau. They have more to come with the addition of adjuvant only trial as well as combination trials, current and in the future. With real world data policies implemented and the regulators trying to make the combination and other trials broadly available to all patients, a lot of this should ultimately be much accelerated.
No I do not know of any similar gbm trials.
I agree. We are obviously blazing our own trail. And to answer your question, no.
As far as 2011 information, we are in 2022. I don't care what forward looking statements were said in 2011. My investment is based on the presently available information and that includes great data, commercial manufacturing certification by years end and MAA/BLA fully accepted submissions shortly.
13% chance of survival is slim?! This is huge when you were looking at 5-6%. That is a completely nonsensical narrative. Also, drugs get approved on extending patients life for 2 months.
I consider the negatives but invest based on the positive information available. I find no benefit to continuously repeating misleading negative narratives about a company where I'm a long term investor.
Have a good one #3!
Hoff I have not avoided your question this is an excellent trial in helping those with gbm. I applaude the increase from 5 to 6% long term survival for soc to 13%. A wonderful increase bit also a long way to go. No I do not know of any similar gbm trials. Let us hope the combination trials improve on the survival figures, many posters had predicted 20, 25, 40 even 50%. We clearly did not get that but hope for improvement in the future.
I still ask if you have seen any such quiet periods as I have never seen anything at all similar and imo the stick valuation reflects that lack of communication.
I am clearly pleased from the asxm results but had really expected to be giving the sir P wowweee based on nwbo results on 5/10 but imo was handled very poorly and we look up at 70cents
I have been in nwbo near 8 years and early on listened to LP say how close we were even her 2011 interview "about 18 months" and still we wait and worse patients wait. To us for the most part it is just $, for some it is a 13% chance at survival. Two or 3 years back I was calling LG multiple times a month as had a coworker with gbm and others I had hoped could get into a direct trial, it was all supposed to happen 'soon' but they all passed on. At the time I was also thinking 30% or possibly better for gbm survival so I was diligent in calling on progress. Obviously it has taken way longer but that was the expectation given by management not made up by me. I'm a bit more comfortable regarding the passing of the coworker with gbm as yes 13% is better than the soc he received but even at 13% long term survival his chances were pretty slim - 13% vs 87%
Bio, I think the revenue protection would be gained from Dr.'s and Patients choosing the less intrusive and probably less expensive jab. The GBM market for Keytruda is probably a niche market as far as they would see numbers.
Can we see a Keytruda/DCVAX combo injection? ... LOL.
No they do not, Hope, but you can continue to insist. I’m not going to keep posting how over and over and over again with you. It’s a different context and a broadly commercial application basically of a quasi-drug that any doctor in any office in the world can prescribe. Therefore, broadly and especially for a journal, it has completely different commercial and other implications both in terms of the scale of the trial and the incredible number of variations of “studies” under it but also in terms of any embargo, because publishing it will sell journal imprints in the many millions, regardless of which is published first and the drug manufacturer has incredible leverage. You disregard the obvious to claim a “gotcha” that is ridiculous in the context of a tiny study involving an orphan indication and an orphan drug. In this context, being first to publish is likely incredibly important and the reality is, you are not actually in the room negotiating with any editors or journals. We are just anonymous persons on a bulletin board chatting hypothetically. Big difference from actually being there and in the room.
Um bio, the facts conform EXACTLY to how I have described them. I suggest you go back and read the amrn press releases as are still on their site. The conference calls have however been deleted
I think that's Plan 9
BY 9/10:
Red_Right_Hand
Friday, August 19, 2022 1:17:05 PM
Re: hoffmann6383 post# 506419
Post#
506444
of 506510
I believe it was submitted soon before or soon after NYAS and 3-4 months is nothing as compared to how long it can take some articles to work their way through a journal's review and publication process.
I agree and try to convey this as well regularly. It's really a very volatile sector and not for regular folks who are thinking that buying stocks are like investing in a CD or treasuries or IBM.
Exactly right Crash!
I agree 100% Jimmy.
Exactly, and a subcutaneous version of Keytruda seems unlikely to be more efficacious against GBM and probably won't be efficacious against many cancers. Plus it's not a different drug. The patent would be for the way it is delivered, which would mean that generic versions of the current drug and it's method of delivery would be fair territory. It's not a strategy for protecting and advancing their business further. They'd likely lose a lot of revenue.
Regarding your spouse, I'm glad to hear. You also avoided my question. Anyways, hope you have a good weekend #3!
Hoff, there have been many astounding trials over the years none that I know of had such a quiet period.
My spouse is alive due to one of those breakthrough trials.
Also as most of us seem to believe this treatment has excellent potential how many other companies with succesful phase 3 trials trade at 65 cents and management that remains mostly silent. There is this concept of quarterly calls, letter to shareholders and timely asm - what an odd concept
Have a great on - I did
I disagree completely and I have given you numerous explanations. You don't agree, that's fine, but I think it's a completely different situation and in fact that the facts don't fully confirm your assertion. But that's because it's such a huge, consumer focused trial, with numerous nuances and sub-studies.
Better to not ask how the same sausage is made.
Meanwhile, as Stephen Colbert says, the FDA can spend months deciding whether to end a sentence with a period, question mark, or exclamation point. I shouldn't take 6 months to decide how to boil 4 minute eggs, but at the FDA that's about the minimum time that anything can be decide
Bio imo the amrn case is completely comparable- pr and conference call in September with tld summary on primary endpoint. November a presentation with company and.PI on a conference call and at same time published in NEJM. Completely what I had hoped for from nwbo.
Did great things for stock valuation wish nwbo had followed the same path I wanted $6.50 by now not 65 cents and wondering if there is even a paper or bla on the way - it shows in the stock valuation. Based on the potential it should be much higher if handled well.
At least I had a GREAT day
What we don't know, and probably never will, is what's holding up the Journal publication. If it's an issue between the clinicians and the Journal, I'd think that L.P. could have some influence, but if the Journal wants to see something from the regulators, probably the FDA, they move at their own pace and the last thing you want to do is irritate them.
I really can't say if the Journal publication will go into how this trial may be changing the way most future trials are done, but in reality it's doing that. If the Journal is going that far, I could see them wanting official acknowledgement of the changes from the FDA, not just a publication they made in Annuls of Oncology. While it was clear there as to what the FDA intends to do, it wasn't official.
The good news is the U.K. isn't waiting for the FDA, and I don't believe the other regulators are either. Canada really hasn't been heard from but I believe many think they'll follow the U.K.'s lead. For all I know the next thing we may hear is that the U.K. has accepted our application, we know they're looking at the manufacturing process, so if we get that, no telling how soon the first approval will come.
Meanwhile, as Stephen Colbert says, the FDA can spend months deciding whether to end a sentence with a period, question mark, or exclamation point. I shouldn't take 6 months to decide how to boil 4 minute eggs, but at the FDA that's about the minimum time that anything can be decided.
Gary
The only confounding thing here is lack of Growth on ur part!
Keep trying the Lack perspective.
Smart investors pass that barrier long long long ago!
SMH
Very long NWBO!
martyDg - I PM'ed you.
ILT
Very interesting. Thanks for sharing.
Comparing this with standard trials is nonsense. Again, where is any international trial that obtained 5 year survival data for nGBM and rGBM patients?! There isn't one. We are making our own path and following best practices while doing so.
Have a good weekend #3
|
Followers
|
1622
|
Posters
|
|
|
Posts (Today)
|
35
|
Posts (Total)
|
689065
|
|
Created
|
02/02/05
|
Type
|
Free
|
| Moderators XenaLives sentiment_stocks CaptainObvious Poor Man - Doc logic JerryCampbell | |||
![]()
“Now this is not the end. It is not even the beginning of the end. But it is, perhaps, the end of the beginning.”
~ Winston Churchill

Stylized Dendritic Cell featured on NWBO board since 2015

- Dr. Linda Liau, PhD, MBA, Professor and Chair, Department of Neurosurgery, David Geffen School of Medicine at UCLA
Clinical Trials
DCVax®-L to Treat Newly Diagnosed GBM Brain Cancer (NCT00045968) - Phase III (Double Blind)
UK (MHRA): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
DE (Germany - PEI): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
Expanded Access Protocol for GBM Patients with Already Manufactured DCVax®-L Who Have Screen-Failed Protocol 020221 (NCT02146066) (Expanded Access)
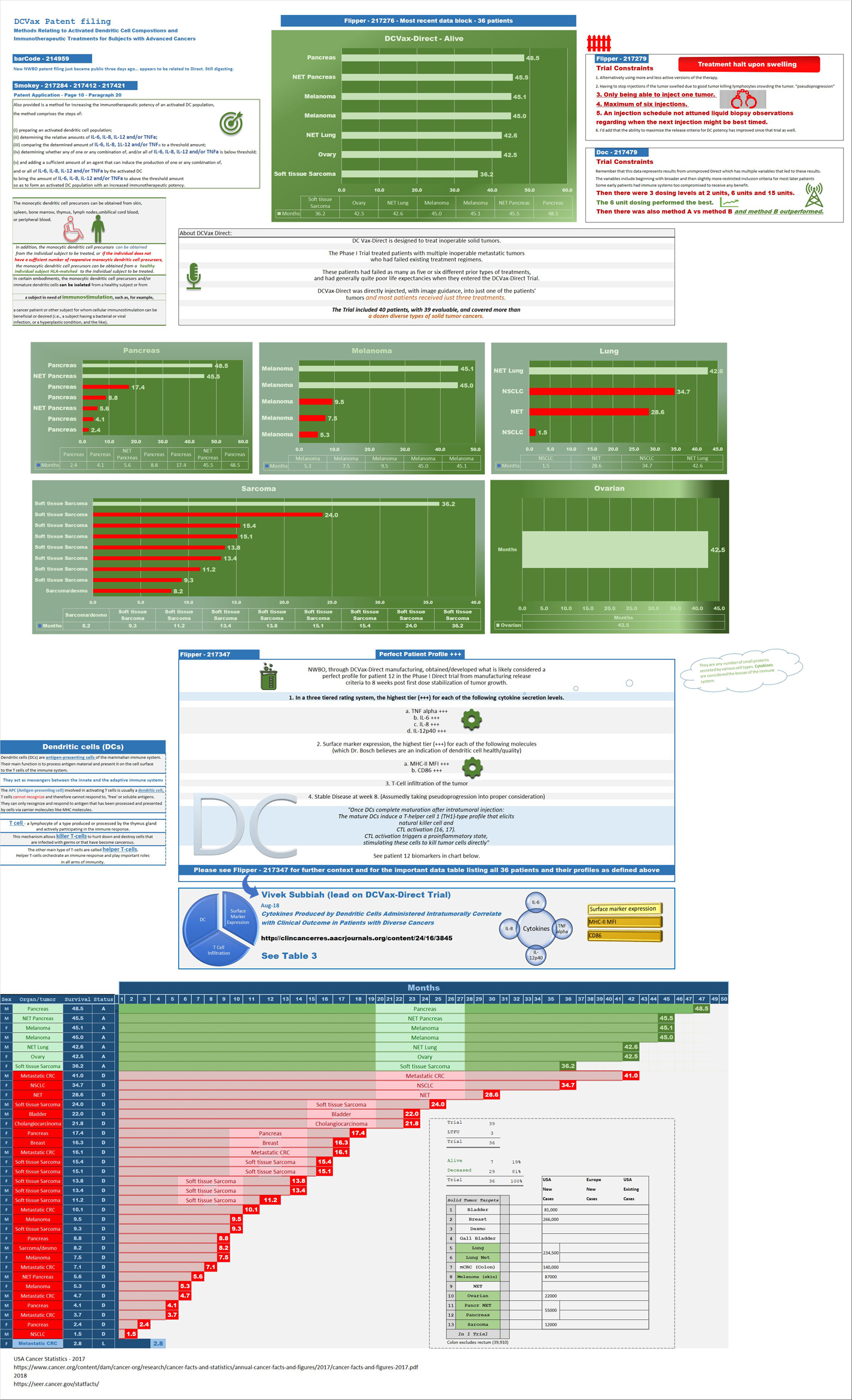
Safety and Efficacy Study of DCVax-Direct in Solid Tumors (NCT01882946) - Phase I/Phase II (Open Label)
UK Clinical Trials - Study of a Drug (DCVax®-L) to Treat Newly Diagnosed GBM Brain Cancer
EU Clinical Trials for DCVax-L - Phase III
Dendritic Cell Vaccine for Patients with Brain Tumors (NCT01204684) - Phase II - at UCLA - Randomized (Open Label) testing DCVaccine with Resiquimod and DC Vaccination with Adjuvant polyICLC
Pembrolizumab and a Vaccine (ATL-DC) for the treatment of Surgically Accessible Recurrent Glioblastoma - Phase 1 (NCT04201873)
Dendritic Cell-Autologous Lung Tumor Vaccine (DCVax-L) and Nivolumab in Treating Patients with Recurrent Glioblastoma - Phase 2 (NCT03014804)
Dendritic Cell Therapy for Brain Metastases From Breast or Lung Cancer (NCT0368765) - Phase 1 - Collaborator: Mayo Clinic
Announcement of DCVax-L and Anti-PD-1 Monoclonal Antibody (Pembrolizumab) for Patients with Liver Metastases of Primary Colorectal Carcinoma Phase 2 Trial - November 17, 2016 - University Medical Center (UMC) of the Johannes Gutenberg University of Mainz
Cognate Bioservices - Owned by Charles River Labs
Website
Company Contact Info
Investor Relations:
Les Goldman (Company) (202) 841-7909 lgoldman@nwbio.com
Sign up for Northwest email list here (hit the subscribe to email list button in the lower right)
Company Headquarters
4800 Montgomery Lane, Suite 800, Bethesda, MD 20814 (240) 497-9024
NW Bio is developing cancer vaccines designed to treat a broad range of solid tumor cancers more effectively than current treatments, and without the side effects of chemotherapy drugs. NW Bio’s proprietary manufacturing technology enables them to produce its personalized vaccine in an efficient, cost-effective manner. NW Bio has a broad platform technology for DCVax dendritic cell-based vaccines.
Their lead product, DCVax-L, is currently in a 331-patient Phase III trial for patients with newly diagnosed Glioblastoma multiforme (GBM), the most aggressive and lethal brain cancer. This trial is currently underway at 69 locations thoughout the United States, Germany and the United Kingdom. NW Bio has also conducted a Phase I/II trial with DCVax-L for late stage ovarian cancer together with the University of Pennsylvania.
Their second product, DCVax-Direct, is currently in a 60-patient Phase I/II trial for direct injection into all types of inoperable solid tumor cancers, with trials currently being conducted at both MD Anderson Cancer Center in Texas, as well as Orlando Health in Florida.
They previously received clearance from the FDA for a 612-patient Phase III trial with its third product, DCVax-Prostate, for late stage prostate cancer.
DCVAX Survival Stories & Testimonials
Alice - Metastic Merkel Cell patient from Florida - ASCO 2018
Brad Silver - GBM patient from Huntington Beach, California - ASCO 2018
Sarah Rigby - GBM patient from Hong Kong - ASCO 2018
Kristyn Power - daughter of GBM patient from Canada - ASCO 2018
Kat Charles - GBM patients from UK - ASCO 2018 - as related by her husband Jason (Kat's Cure)
Prospective patients may contact NW Bio at patients@nwbio.com
UCLA Jamil Newirth DCVax-Patient Video - 2015
Allan Butler Video - National Geographic Vice President - DCVax-Direct patient from Phase 1 Trial with Pancreatic Cancer
NWBO - Patients Sunday Dennis and Jami Newirth - Enrolled at UCLA - Vimeo, Uploaded approx. May 2015
NWBO - Vaccine Helps Keep Brain Cancer Patient Alive (Jennifer Sugioka) - NBC Channel 4, Southern California, February 24, 2015
NWBO - National Geographic's Allan Butler Stage IV Pancreatic Patient using DCVax-Direct at MD Anderson
NWBO GBM Brain Cancer Survival Story of Mark Pace

Presentations

UCLA Agreements
Prostrate
DCVax-Phase II
DCVax-Booster
Upcoming Events
Videos
Linda M. Liau, MD, PhD, MBA - April 24, 2019 at University of Washington, Neurosciences Institute
| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |







