 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.



GermanCol
![]()
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
I think those patients that Dr. Liau mentioned are part of the 17 that didn't cross over (not part of the 18 censors that crossed over and received DCVax after pseudoprogression or whose time of progression was not well established in order to be included in the 64 rGBM arm). And most of them didn't cross over because they very sick or died without crossing over.
I never said or implied they could detect psPD in the 99 arm and not in the 232 arm. What I said is that in the 99 patients arm, all patients that were pseudo progressors, that were additionally thought to be progressors and, as consequence of that, crossed over (and started to recieve DCVax L) had to be censored not only for PFS, but also for OS. And that is because they were not SOC-only patients anymore, they started receiving DCVax from pseudoprogression, so their OS could not be used for the purpose of comparing against SOC after that. On the other hand, that is not the case for the 232 patients arm, because anyway they were receiving DCVax from the beginning. So for the case of this arm, they needed to be censored for PFS, but not for OS.
The whole explanation is in my answer to Ex. Post 677821
So 13 of the 13 early OS censors just happened to be in the SOC arm? Wow. What are the odds. Try ..00000014738810721990. Any RA would have a field day with that one.


So they could detect the psPD in the 99 but not the psPD in the 232. Sure.
The 1% difference can explain 13 censors in theory. Censors only effect the step size after them. So if most censors have few events after them they have little effect.
And now you are off the deep end. Anybody with the slightest clue knows that the the original OS of 232 vs 99 would be a huge.
GermanCol, your argument on censors being discarded fails, badly.
First, Flipper is correct. If the LTFU's are gone, that is because they were found. One does not delete censored data when the SAP says otherwise. This one is trial stats 101.
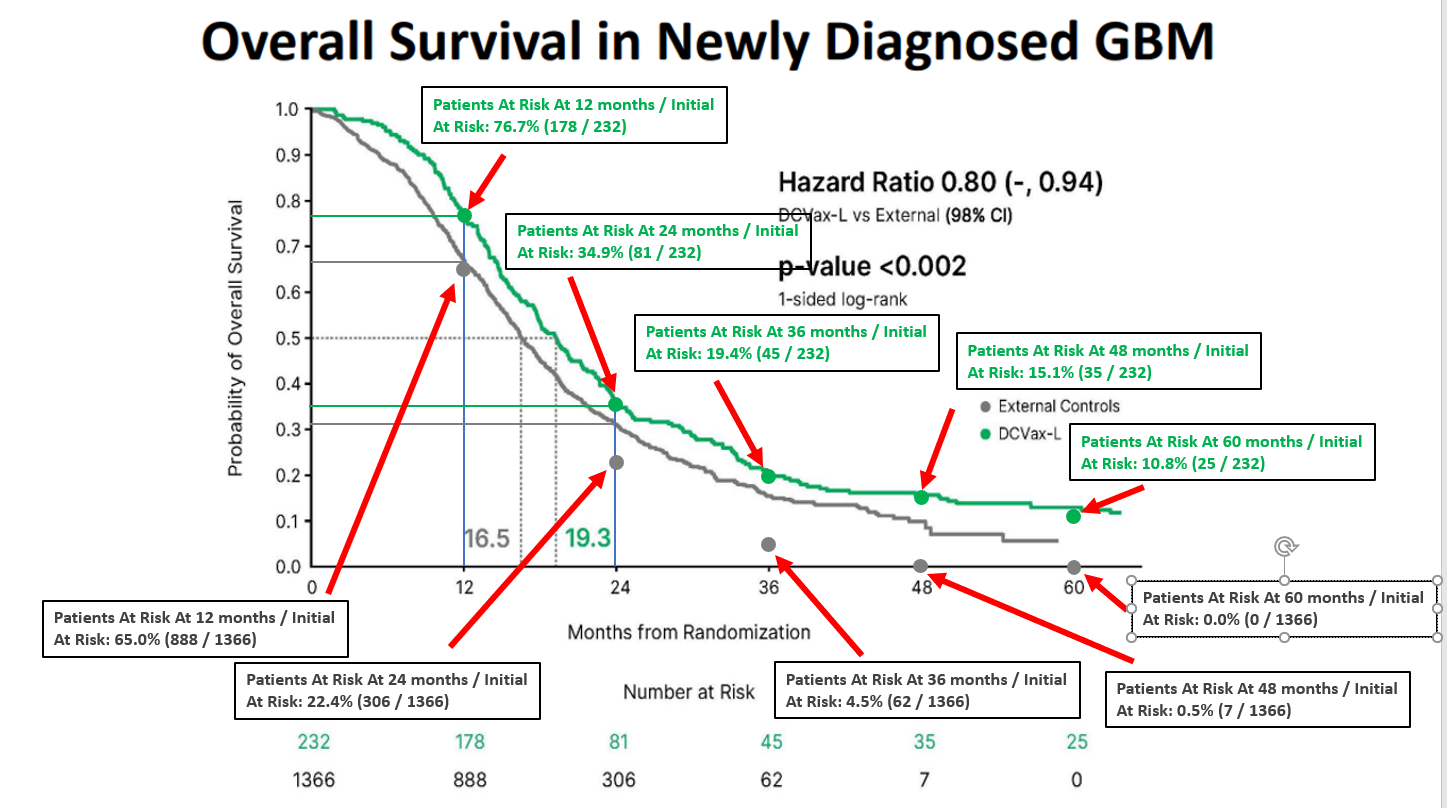
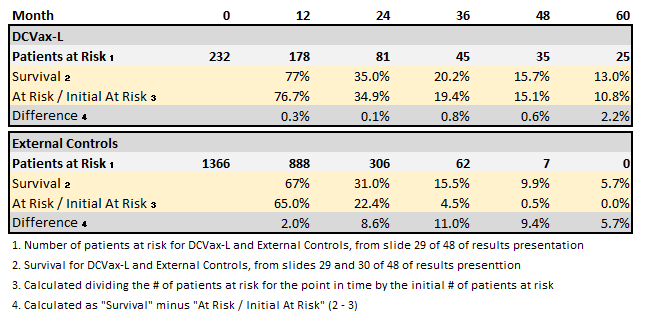
Your key point is the read at 24 months where you assert the K/M shows 35% OS and thus no censors prior to then (when about 8 or 9 would have been expected in the 2018 dataset).
Problem is that 35% read. I put the graph into a digitizer and see the number more like 36% (precision is clearly an issue, even with tech assistance). And that is enough to allow for several censors, even 8 or 9 is possible.

What is a fact is that a "win" in the 232 vs 99 OS comp would be huge, even if not stat sig. It is still an endpoint of the trial. And team NWBO has buried it.
1. The primary objective of this study is to compare overall survival (OS) between patients randomized to DCVax-L and control patients from comparable, contemporaneous trials who received standard of care therapy only, in newly diagnosed glioblastoma.
2. The first secondary objective is to compare overall survival (OS) between patients randomized to placebo who received DCVax-L treatment following disease recurrence, and control patients from comparable, contemporaneous clinical trials, in recurrent GBM.
3. The fourth secondary objective, OS, is overall survival compared between subjects randomized to DCVax®-L and those randomized to Placebo within Study 020221.
At best, DCVAX doesn’t do anything
I missed that. Could you link to his post? Thanks.
Thanks a lot.
Thanks Flipper, something I didn't see mentioned is the proportion of MGMT Methylated vs. MGMT Unmethylated patients and if that was taken into account for randomization. That clearly affects the results. I also didn't see anything regarding IDH-1 Mutant vs. Wildtype. Did you or anyone see anything about that and if any other aspects like age, KPS, etc. were taken into account for randomization?
Thank you very much for saving us. I can clearly see you are an expert. How couldn't we see that before. Unfortunately I can´t sell my shares Today, will do it first time Monday. I hope I can sell them before too much people read your analysis. Thank you savior.
Thanks a lot Flipper!!
Thanks a lot TTsr!!
Thanks a lot Hoff!!
Hello Hoff!! Nice to see you. Could you explain me and any other interested parties exactly what is this (in more detail)? Thanks in advance.
Dstock07734, no, I'm not from Germany. Sorry, I don't know the answer to your question.
The endpoint of OS for 232 vs 99 is still a secondary endpoint of the trial and certainly has meaning. One would expect that if -L works then the 232 live (numerically) longer than the 99 despite the crossover.
1. The primary objective of this study is to compare overall survival (OS) between patients randomized to DCVax-L and control patients from comparable, contemporaneous trials who received standard of care therapy only, in newly diagnosed glioblastoma.
2. The first secondary objective is to compare overall survival (OS) between patients randomized to placebo who received DCVax-L treatment following disease recurrence, and control patients from comparable, contemporaneous clinical trials, in recurrent GBM.
3. The fourth secondary objective, OS, is overall survival compared between subjects randomized to DCVax®-L and those randomized to Placebo within Study 020221.
Further, it would hugely positive. if even close to stat sig. Why would they not be shouting t out?
On the LTFU issue, you still have issues. Despite what you and flipper assert, finding censors does not have to lower the OS. It could go either way depending on how long the lived after the censor. If the censors were unbiased and random they would have no effect. True, there likely is some bias. But you still are talking a fairly minor effect from the few found LTFUs. More on the numbers on a post later.
Thanks a lot Dr Bala!!
Thanks a lot for your words Bio!!
Thank you very much for your words Marzan!! Appreciate them.
you can not ignore NWBO's failure to disclose the data. That is such a huge issue that I fall to see how anybody can ignore it.
So additionally, I’d point out you have already claimed multiple times the original main OS endpoint failed, that the original experimental arm is worse than control, and they will never show it. You don’t know any of this is true. They are still conducting follow up. Those results have not been released. You don’t understand impacts of censoring removal.
You can think whatever you want. I can understand that for you that behavior would be completely normal, because of the way you act.
Hyperopia, I totally agree with you. I continue being positive about the science, haven't sold a single share and for now will keep them (I don't know for how long). But I am really disappointed with this management, mainly because of this aspect you mention. We, longtime shareholders, don't get the respect we deserve, to say the least.
I believe that half-truths have been used to string investors along
I think your confusion may come from mixing up short sale volume with short interest. Below you will find an explanation of the difference and why they can be normally confusing:
https://www.tradersmagazine.com/departments/equities/understanding-short-sale-activity/
https://www.finra.org/investors/insights/short-interest#:~:text=The%20short%20interest%20data%20is,sales%20on%20individual%20trade%20dates.
Since this data also comes from FINRA, what gives? The daily short selling volume is misleading because market makers and principal trading firms report a large number of trades as short sales in positions that they quickly cover. For market makers with a customer order to sell, they will temporarily sell short (which gets published to the tape as a media transaction for public dissemination) and then immediately buy from their customer in a non-media transaction that is not publicly disseminated to avoid double counting share volumes. SEC guidance also mandates that almost all principal trading firms that provide liquidity at multiple price levels, or arbitrage international securities, must mark orders they enter as short, even though those firms might also have strategies that tend to flatten by end of day. Since the trade reporting process for market makers and principal trades makes the Daily Short Volume easily misleading, we do not display it on www.otcmarkets.com.
What Short Interest Is Not
In addition to short interest data, FINRA also publishes Short Sale Volume Data. The Daily Short Sale Volume data provides aggregated volume by security for all off-exchange short sale trades. This data excludes any trading activity that is not publicly disseminated and is not consolidated with exchange data.
Some market participants mistakenly conclude that the bi-monthly short interest data is understated because the Short Sale Volume Daily File reflects volume that is much larger than the positions reported as short interest. However, short interest position data does not—and is not intended to—equate to the daily short sale volume data posted on FINRA’s website.
The short interest data is just a snapshot that reflects short positions held by brokerage firms at a specific moment in time on two discrete days each month. The Short Sale Volume Daily File reflects the aggregate volume of trades within certain parameters executed as short sales on individual trade dates. Therefore, while the two data sets are related in that short sale volume activity may ultimately result in a reportable short interest position, they are not the same.
Investors may establish short positions in a security that continue to exist for varying lengths of time, which can result in a short position being represented in one of the data sets but not the other. For example, an investor may sell a security short and purchase shares to close the position on the same trade date. That position would not appear in the short interest data, though the short sale transaction would appear on the Short Sale Volume Daily File.
On the other hand, an investor may hold a short position open for days or weeks, perhaps as a hedge against another position. While the short sale transaction that established that short position would appear in the Short Sale Volume Daily File only on the date the short sale transaction occurred, the short position would continue to be reflected in the short interest data for as long as the position remained open.
65 % (n=15) had diagnoses of IDH wild type glioblastoma (WHO Grade IV), while 35 % (n=8) of the patients had a diagnosis of IDH mutant malignant glioma (WHO Grade III).
The DC+Poly arm showed a 27 month in the 5 GBM patients. None lived 5 years, And this is with a large percent of IDH mutant (which live longer)
65 % (n=15) had diagnoses of IDH wild type glioblastoma (WHO Grade IV), while 35 % (n=8) of the patients had a diagnosis of IDH mutant malignant glioma (WHO Grade III).
IDH mutations were observed in 35% (n=8, all grade III)
Excellent post. Agree 100%.
OncoJock, thanks for your answer and sorry for my comment accusing you. My mistake :)
Page 17, cont'd. Footnote (3) in the chart makes clear that only one of 6 projects related to the application, the project describing the mechanism of action of DCVax, had been completed as of March 31. The other 5, namely sections on comparability, stability, potency, product profile, and fill/finish, remained to be completed.

Biosectinvestor, it is because aproximately $76.3 million of warrant liability was reclassified from liabilities to equity after the AS increase, as explained in section 3. Summary of Significant Accounting Policies of the 10-Q.
Sequencing
The Company adopted a sequencing policy under ASC 815-40-35 to determine if reclassification of contracts from equity to liabilities is necessary pursuant to ASC 815 due to the Company’s inability to demonstrate it has sufficient authorized shares. Certain contracts were classified as liabilities as the result of the instruments containing a potentially indeterminable number of shares and, most recently, due to the Company entering into agreements providing for the potential issuance of more shares than authorized. While temporary suspensions are in place to keep the potential exercises beneath the number authorized, certain instruments are classified as liabilities, after allocating available authorized shares on the basis of the earliest grant date of potentially dilutive instruments. Pursuant to ASC 815, issuance of stock-based awards to the Company’s employees, nonemployees or directors are not subject to the sequencing policy.
On January 9, 2023, the Company filed a Certificate of Amendment of its Seventh Amended and Restated Certificate of Incorporation (the “Certificate of Amendment”) with the Secretary of the State of Delaware, which effected an increase in the Company’s authorized shares of common stock, from 1.2 billion to 1.7 billion, par value $0.001 per share. As a result of this increase in authorized shares, the liability-classified warrants were reclassified to equity. Approximately 141 million warrants, with a value of approximately $76.3 million, to purchase shares of the Company’s common stock were reclassified from liabilities to equity on January 9, 2023. The remaining balance of $1.4 million in warrant liability as of March 31, 2023 was related to certain conditional rights to independently purchase shares from the Company in a future raise of capital (the “Piggy-back Rights”).
Just checking it.
10Q out.
Agree 100% kabunushi
Thanks a lot pqr for your words and for all you do for us also. Best regards.
Whatever they saw was not an issue with DCVax, because the plan for the trial was to have 232 patients randomized to DCVax and 116 to placebo and it ended with the same 232 randomized to DCVax and only 99 to placebo. So the 17 not recruited where taken out of the placebo arm. Actually what they did was send all the last patients to DCVax. Opposite to what you are trying to infer, it is a very positive sign because they accelerated DCVax recruitment and didn't recruit all placebo patients. And maybe, just maybe, the reason is that the external control arms where starting to be seen as an option with the crossover and pseudoprogression issues that were leaving the trial without a placebo arm, so they didn't want to continue sending patients to placebo, and decided to send all of them to a treatment that was clearly working.
*English is not my native language.
Can’t explain why Jerry J. entered into a purchase agreement for preferred shares, especially given the company clearly is in the process of material events. Perhaps there are some fine legal distinctions between what constitutes material and non-material, or material matters not yet brought before a vote, and don’t involve him; otherwise mattered kept to a much tighter circle.
Excellent work Hoffmann. Thank you, very much!!!
I wasn't able to watch the video and now it is not available anymore for what I see.
You're very welcome NotSure2.
No, JAMA didn't give details about that. I think we will get those details in the future.
NotSure2. I think they are not related (I tried to find a link between the two 17 numbers because I don't believe to much in coincidences, but didn't find it). The 17 Doc Logic is talking about are patients that were supposed to be enrolled in the trial, but were not finally enrolled:
348 (initially supposed to be enrolled) - 331 (finally enrolled) = 17
And the good news is that the 17 not enrolled were taken out of the initial placebo arm and not of the treatment arm:
Number of patients in intial trial design:
Placebo: 116 (1/3 of patients)
Treatment Arm: 232 (2/3 of patients)
Total: 348
Final number of patients:
Placebo: 99
Treatment Arm: 232
Total: 331
61 days.
In case this kind of posts do anything to the stock, it is not support, just harm.
Yes, NWBO was included in Powerscourt healthcare clients page in May 26, 2022 and not anymore. I used the wayback machine to check:


