 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.






WeeZuhl
![]()
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
50% to Epic seems a little steep but maybe it was the best good deal Nasrat could swing
Elite will receive a license fee computed as a percentage (50%) of net sales of the Products as defined in the Agreement and is entitled to multi million dollar minimum annual license fees Elite will manufacture the product for sale by Epic on a cost plus basis
Couch, I feel better now.
Added 16,000 at .332. Both of my accounts are now back in good order with share counts divisible by 10,000, as is right and proper. My OCD exacerbation is now resolved. Thanks to the MM's for this opportunity to top-off my accounts and resolve my neuropsychiatric dissonance. Ahhhhhhhhhhhhhhhhhh, that's the stuff!
First report of this. Sweet deal, Nasrat.
Elite will receive a license fee computed as a percentage (50%) of net sales of the Products as defined in the Agreement and is entitled to multi million dollar minimum annual license fees Elite will manufacture the product for sale by Epic on a cost plus basis
Nice e-mail N2K.
By so specifically detailing your concerns, you've boxed them in to disclose public info if anything is awry with the Epic SequestOx deal. I'd say you got about as much of an answer as you could rightfully expect. Steady as she goes, keep on keepin' on, "business as usual."
I've always subscribed to the theory that the SequestOx deal was the real value asset in Humanwell Epic acquisition. Just like that they've gotten themselves a foothold in the U.S. opioid market. I'm a strong proponent of the deal, and I believe it is a benefit to Elite to have a more muscular partner in the rollout. I also expect the future milestone payments will not only be prompt and in-full but also will no longer be preceded by the obligatory ELTP share sell-off by Epic Investments. And I'm positively thrilled by the movement to independent directors and away from Epic insiders. Those guys saved our ass, and they will be handsomely rewarded. But I'm glad to have them at arm's length.
Another Nasrat Question: Did You Kill KemPharm?
The FDA is now well-familiar with SequestOx HAL data. Did the excellent performance and impending approval of IR opioid SequestOx contribute to the rejection of IR opioid Apadaz and the demise of KemPharm?
Thanks MJ.
Question: Pfizer's antagonist ADF ALO-02 had less than impressive HAL results with crushed tablets orally ingested. How does Elite's antagonist ADF ELI-201 perform on HAL studies when crushed and orally ingested?
Perfect timing for SequestOx approval.
I would like to personally thank KemPharm and the FDA for the high drama leading into the first ever approval of an immediate-release opioid with Category III ADF label. SequestOx is the flagship proof of concept of the ELTP modular 2 bead pharma ADF technology. Unlike KemPharm's prodrug ADF, SequestOx ADF properties are confirmed in HAL trials: effective, durable, and aversive. Approval of SequestOx is just the beginning...
http://www.fiercebiotech.com/fda-overrides-adcomm-shoots-down-kempharm-s-opioid
FDA overrides adcomm, shoots down KemPharm’s opioid
by John Carroll | Jun 13, 2016 4:35pm
Evidently the FDA insiders were even less impressed, issuing its complete response letter. The company gave no hint about what the FDA will require them to do to get the CRL reversed and the pain drug on the market.
The rejection comes at a time that the opioid epidemic has become a central issue in communities across the country. Today a new study from Johns Hopkins noted that more than half of the people taking an opioid end up setting some aside to share or use later. And that is contributing to an epidemic that has roiled the nation and put all opioids under an intense spotlight. In many ways, this is a bad time to try to introduce a rival that can't be considered abuse deterrent.
It is very simple. Never push the FDA! KMPH should have accepted APAP Apadaz approval WITHOUT ADF label!
I would like a peek at that letter.
Didn't see that one coming. Any thoughts on the outright rejection?
Well that's interesting, Heidi.
The FDA issues CRLs to indicate that the Agency considers the review cycle for an application is complete and that the application is not ready for approval in its present form.
No ADCOM could mean they just haven't scheduled one yet. PDUFA dates get pushed. Examples posted on this thread.
The inference of certainty based on something not happening is a form of extreme optimism bias.
Interesting deal for ADF development.
Looks like mostly European (UK) interests developing an ADF for U.S. Market. As of yesterday, SkyePharma is now merged with Vectura, whoever the hell that is. The details are interesting, especially since the claims of their physiochemical barrier technology sound very similar to IPCI’s claims about Rexista. There are no other drugs in development using this technology, and the deal basically sets up a four year development to market timeframe. Based on the data available on the Lucideon website, the technology is already well-developed at this point, but it does not sound like they have even started a specific agonist formulation as of yet, whereas IPCI has announced bioequivalence to OxyContin and claims NDA to be filed in next few months. The basic gist of the deal is US $6 million over 4 years with “single digit share of Skyepharma's royalty revenues from in-market sales of the product,” whatever the hell that means. Lucideon will provide “specialist expertise with its technology” but sounds like the agonist formulation work will be done in-house by SkyePharma/Vectura.
http://www.pharmatimes.com/news/skyepharma_buys_access_to_abuse_deterrent_drug_delivery_tech_1036803
SkyePharma buys access to abuse deterrent drug delivery tech
8th June 2016
By Selina McKee
…
The UK group has signed an exclusive feasibility, development and licence agreement with Lucideon for use of its iCRT proprietary oral drug delivery platform technology, which is designed to enable drug products to retain their controlled-release properties regardless of tampering methods such as chewing, crushing and heating.
Skyepharma said it initially intends to use the technology to develop an abuse deterrent formulation of a "major opioid" for the US market which, according to GBI Research, is set to grow from $11 billion in 2014 to $17.7 billion by 2021.
Under the deal, the firms will work together over the coming months to assess the feasibility of using the technology in this novel way. Skyepharma will fund this development work, in line with current R&D spend plans. Lucideon will provide specialist expertise with its technology, and Skyepharma's oral business will formulate the product and complete an abuse deterrence challenge study.
Lucideon stands to receive milestone payments as the development progresses as well as a single digit share of Skyepharma's royalty revenues from in-market sales of the product. Assuming a successful development, the investment by Skyepharma is expected to be around £4 million over four years, which is within Skyepharma's existing guidance for overall investment in research and development.
Abuse Deterrent Technology
iCRT-deter is Lucideon’s patent-pending, oral drug delivery platform technology that provides abuse deterrent controlled release properties.
Products that use iCRT-deter retain their controlled-release properties during conventional tampering methods such as chewing, crushing and heating, unlike many other tamper resistant techniques.
Key abuse deterrent features include:
*Extremely hard structure that is very difficult to crush without specialist grinding
*Particulate technology that allows individual particles to retain their properties even if crushed from a tablet
*Extremely high melting point (1000°C+) to deter injection, as melting the carrier will destroy the drug
*Low solubility and large particle sizes unsuitable for injection through suspension
*Equal or significantly reduced drug dissolution in alcoholic media and other household solvents.
iCRT-deter technology incorporates active molecules within the nanoporous matrix. A coating can also be added to the formulated product to add extra protection and increase the control over release rates.
Aversive agents can also be added if the coating is broken to aid abuse deterrence. These include:
*Unpleasant tastes to deter oral consumption after the tablet is broken
*Waxy additives to stick together crushed powder, making nasal inhalation difficult
*Color leaching in liquids, to deter spiking of drinks.
We know it.
Not that the FDA shouldn't need a broad swath of opinion but some of these contributors are making things more difficult to treat in the real world, outside of the ivory tower.
Pfizer's Oral Problem.
First is the large volume extraction issue, where oxycodone is selectively extracted with multiple common solvents. This problem is for whole beads and not applicable to ELTP 2 bead tech, which has different polymers and sequesters naltrexone differently (i.e. not buried in the core of oxy). It has been reported in multiple ways that ELI-200 passed this kind of common solvent extraction. Since ALO-02 solvent extraction requires a relatively large amount of fluid, it rules out IV injection but makes for a lovely oxy cocktail.
But there's also this: ALO-02 does surprisingly bad on crushed oral ingestion HAL studies. The following graph shows the data differently than we are used to seeing on the drug-liking curve. (Remember what I said about being suspicious of any ADF without a published drug-liking curve). Here, they take the peak number from the drug liking curve and show it as a bar graph. Below that is a bar graph for "Take Drug Again." It speaks for itself, especially the higher dose.


Pfizer's recent AdComm was for their extended release product. People are misconstruing the facts. SequestOx IS an immediate release product.
This is a trick question.
if the fda gives Sequestox the same approval as PFE's drug (I.e., adt labeling for iv and nasal but not oral), it's not going to help us - we need all 3 adt labels (iv nasal oral) to be profitable.
Right?
The FDA made it clear that $ELTP would get no credit for their ADF Naltrexone bead combined with an Agonist/APAP.
The FDA does not label APAP ADF as made very clear to Nasrat Hakim.
Our discussions with the FDA have been constructive and we are hopeful that we can agree on an approval pathway that includes abuse-deterrent labeling for Apadaz,” said Travis C. Mickle, Ph.D., President and CEO of KemPharm(KMPH).
I highly doubt the price drop today had anything to do with Pfizer's meeting, honestly.
Exactly right.
The FDA is trying to come to grips as to what ADT should mean at its minimum and you could hear the panel struggle with what is or isn't enough as to what is or isn't a "true" deterrence.
Once again we agree, namtae
Just a matter of time.
ELTP a total POS headed much lower.

This must be what Pfizer is talking about?
http://blogs.fda.gov/fdavoice/index.php/2016/02/changing-course-a-new-approach-to-opioid-pain-medication-at-fda/
Changing course: A new approach to opioid pain medication at FDA
Posted on February 5, 2016 by FDA Voice
By: Robert M. Califf, M.D.
First, we’re going to be more transparent and open in the approval process for this category of drugs. Starting today, the FDA will convene an expert advisory committee before approving any new drug application for an opioid that is not in an abuse-deterrent formulation (ADF).
Robert M. Califf, M.D., previously FDA’s Deputy Commissioner for Medical Products and Tobacco, became FDA’s Commissioner of Food and Drugs on Feb. 25, 2016
One issue no one seems to be discussing much is why is there no AdCom for ELTP?
Teva's Vantrela gets ADF nod from AdComm.
Teva's Vantrela hydrocodone ADF is recommended to get Category III ADF label by AdComm, and rightly so. It looks good on the drug liking curve:

For comparison, see the SequestOx drug-liking curve, which will be the first immediate-release opioid to receive Category III ADF label from the FDA:
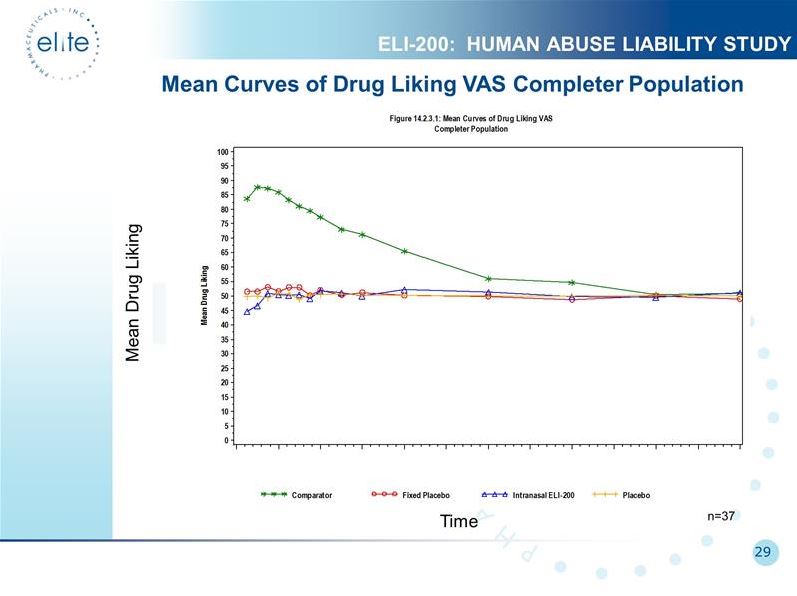
Shows Mean Drug Liking on Visual Analog Scale (VAS). Time is on horizontal axis. On the verticle axis, anything above 50 means they liked it, below 50 they disliked it. Notice the expected liking of snorted oxyIR (green). ELI-200 (blue) has ZERO drug liking, indicating an EFFECTIVE ADF. ELI-200 is *disliked* at the outset (blue line falls below the placebos (red & yellow)). This means it is an AVERSIVE ADF. Also, ELI-200 never bumps above the placebo line, indicating it is a DURABLE ADF.
ELTP 2 bead pharma ADF is EFFECTIVE, AVERSIVE, DURABLE, and MODULAR across the entire spectrum of opioid agonists and time-release profiles. Fully-licensable. The Golden Ticket.
N2K, he seems to have a different target...
To the point of an acquisition, there is absolutely NO VALUE in uplisting to the Nasdaq. That takes time and money not well spent.
...I’ve said this before, I have more than a dozen ideas for our stock that are ready to go into clinical trials and into the market. We don’t have to mind or to execute all of them. So we decide which are the cream of the crop, the top two, three, or four, and focus on these, keeping in mind how much they’re going to cost..
You do not sell a billion dollar technology for one product’s price.


Zogenix ER Bunionectomy
https://clinicaltrials.gov/ct2/show/NCT02197156?term=Bunionectomy+and+ER&rank=1
This is a Phase 2 trial where each participant received one single dose of drug after surgery. Really, you should just take my word for it at this point. There will be no true ER/LA opioid Phase 3 efficacy study for moderate-severe chronic pain that uses an acute pain bunionectomy trial.
It is an ER analgesic.
Xartemis XR = 7.5mg hydrocodone
It may be "XR" (12 hour release), but Xartemis XR contains half the hydrocodone (7.5mg) compared to the equivalent dose of oxycodone used in the ELI-200 bunionectomy trial (15mg). ELI-201 Phase 3 would not evaluate acute, post-op pain but rather chronic pain, and the dose will be higher than 7.5mg- 15mg, more like 30-40mg- much too high for opioid-naive post-op patients.
505b2 with bioequivalency bridge to freshly-approved ALO-02 will save 6-12 months and millions of dollars.
Bring on ELI-301
Yep, ELI-301 (morphine ER) should be Elite's third ADF opioid NDA application of the year, after ELI-200 and ELI-201.
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndAnalgesicDrugProductsAdvisoryCommittee/UCM505122.pdf

Yes and no.
$ELTP could use the same two month 150 to 200 persons P3 Bunionectomy trial for their 12 Hr ER Oxy/Nal trial vs Comparators Roxicodone and Revia. There is no need to wait for ALO-02 for which no PDUFA date has been set.
Troxyca Extraction Issues
There are several issues identified. I do not believe any whole pellet studies can be extrapolated to Elite's 2 bead technology, and their most significant issue was in large volume extraction from whole pellets. Large volume essentially rules out IV abuse, but the preparation could be orally ingested.
There was one issue identified with crushed pellets, which would be essentially the exact same as crushed ELI drugs. There was selective extraction of oxycodone without naltrexone in solvent M27. I suspect crushed ELI drugs should have this same issue. This is not going to be a problem because extraction requires a large volume and the solvent is organic (not household, not readily available, not consumable or injectable). In order to utilize the extracted product, it would require extraction from the organic solvent, which is another multi-step, multi-reagent process.
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndAnalgesicDrugProductsAdvisoryCommittee/UCM505128.pdf
At time point 1, there was similar and nearly complete release of oxycodone and naltrexone in 30 of 31 solvents studied. In one solvent (M27) there was somewhat selective extraction of oxycodone from crushed pellets.
...
The solvent in which potential vulnerabilities were identified is a non-ingestible hazardous solvent that would require additional steps to separate the oxycodone for oral abuse.

Wouldn't it still be more expensive and take longer as Nasrat stated in the past?
what do you think about the FDA decision on Teva?
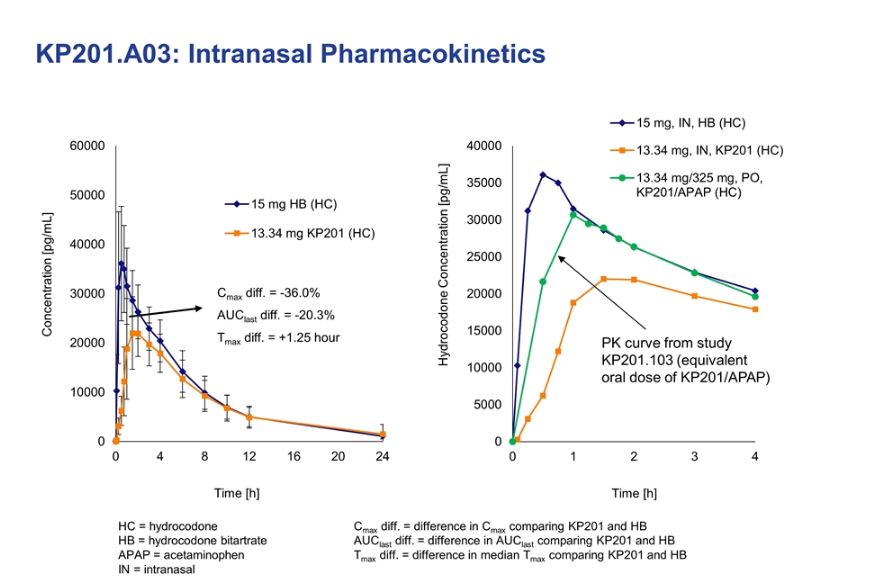
In the second oral pharmacokinetic study, manipulated VANTRELA ER was compared with
intact VANTRELA ER and hydrocodone bitartrate API as an IR comparator. While
hydrocodone levels rose rapidly following administration of hydrocodone bitartrate API,
manipulated VANTRELA ER retained part of its ER properties. The Cmax and AQ of
manipulated VANTRELA ER were approximately 54% and 86% lower than hydrocodone
bitartrate API, respectively.
Five advanced solvents were identified with hydrocodone bitartrate solubility sufficient to be
used for extraction experiments with isolation of drug residue: Solvents m, l, i, j, and n. Prior to
extraction, tablets were manipulated using either Tool A or Tool E. The extractions were
performed at Temperature 7, with Agitation Method W or Z, from 30 minutes to 180 minutes.
Samples were filtered and the solvent removed to isolate solid material. The percent of drug
recovered and the purity of the isolated residues were determined. ZOHYDRO ER manipulated
with Tool A was included as a comparator.
Recovery of >80% of the drug was generally achieved within 30 minutes for VANTRELA ER,
relative to the solubility limit of hydrocodone in the respective solvent. However, the purity of
drug substance extracted from manipulated VANTRELA ER tablets was very low. The percent
of drug recovered from manipulated ZOHYDRO ER was generally >90% within 30 minutes.
The residues isolated from manipulated ZOHYDRO ER extracts, however, exhibited higher
purity than those from manipulated VANTRELA ER tablets.
Nice article, but take caution...
I especially liked Figure 2. But this is from January 2015, and the info is out-of-date in regards to Elite and competitors.
that invalidity is why you never see such cross study comparisons in peer review journals. Of course there is a legitimate technique called meta-analysis but the sophisticated amongst us know the profound difference
Great catch, Couch
While Vantrela ER’s abuse-deterrence properties work better against snorting or injecting, they are only comparable to other extended-release hydrocodone products when abusers use a solvent to extract the opioid from the other ingredients in the pill, FDA staff said in the report.
Recovery of >80% of the drug was generally achieved within 30 minutes for VANTRELA ER,
relative to the solubility limit of hydrocodone in the respective solvent. However, the purity of
drug substance extracted from manipulated VANTRELA ER tablets was very low. The percent
of drug recovered from manipulated ZOHYDRO ER was generally >90% within 30 minutes.
The residues isolated from manipulated ZOHYDRO ER extracts, however, exhibited higher
purity than those from manipulated VANTRELA ER tablets.
surely you know that cross study comparisons are statistically, and clinically invalid
No 10-Q filed since January.
What else is there to say?
ADF WARS: Ventrela vs. Zohydro
Ventrela hilariously throws an elbow at Zohydro on their nasal PK graph.


