 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.


Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Great you are into articles straight out of the UK, since you have quite a record of ignoring these, when they are writing anything in favor of NWBO or DCvax-L. Would that equal = "something is very wrong?" or just highlight the fact, that you have an incentive for only bringing forth information, that you in any way can subjectively distort to a bearish perspective?
I wouldn't know, because we all know how dearly retailers are to your Florence Nightinggale heart.
Let's look into your phenomenal record in that regard, you know .... how something is ripe for manipulation, and how something is left to ignore, because it can not be used succesfully in a short and distort scam.
Let's start easy with text. Just plain text of written evidence from exactly Brain Tumor Charity regarding DCvax-L.
https://committees.parliament.uk/writtenevidence/120702/pdf/
Personalised Medicines and in particular, DCVax®-L
The development of personalised medicines has huge long-term potential in transforming cancer treatment. DCVax-L is a type of immunotherapy known as a dendritic cell vaccine. It has been developed as a personalised vaccine made from each patient’s own dendritic cells. The peer-reviewed phase III trial
results were published in November 2022 and offered very promising results.
The process of making this vaccine involves taking both tumour cells and blood from the patient. Immunecells are separated from the patient’s blood and exposed to the tumour cells; it is through this process that dendritic cells learn to recognise the specific markers and proteins associated with the patient’s tumour cells.
The “educated” dendritic cells are then injected back into the patient, where they go on to recruit and “teach” other anti-cancer immune cells, known as T-cells, to travel to the tumour site and attack the cancerous cells.
Recent studies have shown that using DCVax-L alongside temozolomide chemotherapy can prolong the lives of people diagnosed with a new or recurrent glioblastoma by nearly three months on average, compared to chemotherapy alone. The trial also found that DCVax-L doubled the five-year survival rate for
those with a newly diagnosed glioblastoma and for those with recurrent glioblastoma, results saw the 30-month survival rate double.
It's been used for years and cheap as hell. If it works in a small trial it'll go straight to off label.
Dstock07, I have read many more than 200 papers on use of dendritic cells but have saved to my library over 200 as found them interesting enough to save to my library. Go to the national library of medicine - pubmed - and search on "dendritic cells and cancer" and you will find over 32,000 papers.
Over the years I have focused on papers authored by Prins and/or Liau or those on gbm or other brain cancers and yes there is good science there. By no means a cure for all as per Liau approximately 25% to 35% of gbm patients respond to the autologous tumor lysate but imo clearly helps some. Prins has a good published paper on how the vaccine produced a good infiltration of t-cells but that in some cases the body send in other cells - macrophage macrophage and myleiod cells that negate the effect of the t-cells and they are working to overcome this. Liau in a talk from several years ago speaks on other trials with dendritic cells and gbm and that most show at least some success yet the trials were deemed to be a failure as only a % were helped. She has a slide that says "don't throw the baby out with the bath water", as each trial had a positive effect on att least some of the patients just not a high %.
So yes I believe in the science but imo the management of nwbo has been pitiful slow in the process to trial evaluation (September 2020 when LP said results to be released that month) and completion of SAP (over a year) and applications for approval (LP said applications as in more than 1 - see 2022 asm) and even the single application took forever.
The science is sound the researchers are smart and dedicated the management imo rates a D-
Back in 2015 when I first invested (substantial amount) there were less than 100 million shares outstanding, stock was listed on nasdaq, traded in dollars - as high as $12.54 - and according to the ceo we were on the "home stretch"
And finally - yes I invest with the expectation of at least some rate of return
Not the point of my post, but you know that. It's why I always provide excerpts.
Vortioxetine (brand is TRINTELLIX) works on glioblastoma in MICE.
Could a common antidepressant be the key to fighting deadly brain cancer? New @ETH_en research offers hope, but experts urge caution. #CancerResearch #Glioblastoma https://t.co/Fhg6vGasL6
— ScienceBlog.com (@ScienceBlogTwit) September 20, 2024
Saw the article
Works well in mice and rat it seems . Sure will be a huge competition . We should all be very concerned .
Should we all sell in your esteemed opinion ?
Yet another article straight out of the UK. You can all ignore it but, sorry, something is very wrong.
>>Experts say, should it prove effective, vortioxetine will be the first medicine in recent decades to improve the treatment of glioblastoma.
Commenting on the findings, Dr Simon Newman, chief scientific officer at The Brain Tumour Charity, who was not involved in the study, said: 'Any scientific developments that bring us closer to new treatments for glioblastoma are promising, as treatments haven’t changed in decades.
https://www.dailymail.co.uk/health/article-13872579/amp/Antidepressant-brain-cancer-tumour-glioblastoma-vortioxetine.html
>>Glioblastoma — 22 percent (ages 20–44), 9 percent (ages 45–54), 6 percent (ages 55–64)
https://ukhealthcare.uky.edu/markey-cancer-center/cancer-types/brain-cancer
You read over 200 papers and presentations on this single subject. That's a great achievement! You must be all-in then. Any thoughts about what you read. Please share with us. The longs, at least some of them need some input on this one to boost the morale.
Did you make a comparison of Dr. Liau's work with those from Bhardwaj Nina, Ignacio Melero, and Carolyn Britten? I strongly suggest making a comparison to know how far ahead DCVax-L is.
To evaluate DC vaccine, my understanding as a lay person, is to check how many tumor-associated antigens can be presented to immune system. That's why people may pay attention to 13% OS. But I pay more attention to over 30% occurrence rate of pseudopgression, which is a clear indication of massive t cell infiltration. I suspect massive t cell infiltration can only be triggered when dendritic cells indeed present tons of tumor-associated antigens to immune system. Seems to me it's just that simple. I think data on this regard must be presented to RAs. Who wouldn't be amazed by the solid data of the breakthrough?
As for management, LP must have good reason about whatever she is doing. She has more shares and she has dedicated most of her career life to this cause. More importantly, she already showed us the ASCO presentation and the paper on poly-iclc trial.
BTW, when people say something like 'the science is solid' 'the science is good', I'd like to ask which part makes the science so special and unique.
So true...
Very informative post. I wish we get more info on updated DCVax-D.
You've invested nothing, but your day job of FUD postings.
Good luck to him. What's the schedule now, chemo-rad while they work on the vaccine, then administered when?
Such a simple question yet you all dodge it.
You pumpers are the ones who should be looking over your shoulder for spreading unverified information that even NWBO themselves doesn't mention.
Why?
"Direct needed tech transfer"
Yeah agreed. That creep didn’t talk about the science. Just talking about BK which shows their intention. Whatta POS . Looks like they are desperate.
The criminally collusive cabal must feel approval is near for them to hire that creep to trash nwbo. Talk about pulling out all the stops in their desperation.
Totally agree. This has happened to many pre- revenue companies including BIO. The question is how NWBO going to do about it. This is a mystery that nobody knows except LP and some close people to Decision making process.
If they go franchise direction they will able to collect $ from many BIO companies rather than a few.
After exceeding the £150,000 target in just a few days they now have all the funds they need to complete the full course of DCVax-L
We all wish Stephen Webb a speedy recovery after his successful surgery 2 days ago
Hello everyone. As you know Stephen went in for his operation yesterday to remove as much of the mass as possible.
After a long and complicated surgery, all went well and Stephen is now being closely monitored.
I will keep you all updated as much as I can.
Thank you for all of your well wishes, prayers and support.
Getting close to two years of holding, bought at just over a buck first. I averaged down but that didn't help. At two year anniversary will start selling off my position. Means I will have to work another year but I rolled dem dice and it hasn't worked out. Maybe something will happen in two months but I doubt it..
C'est la vie. Goodbye money but it is only money.
Why do you think these bashers are here 24h/d 7d/w 365d/y?
For the 50M shares reported shorts?
Nah.
Naked shorts are HUGE on NWBO. The range is 800M shares to 1,6B shares.
Hedge funds have shorted EVERY pre revenue companies for years since 99% of biotech companies fail over time.
The problem hedge funds have is they naked shorted NWBO hoping to bankrupt the company even if the Ph3 trial is a big success.
We’ll see soon.
Ps I don’t believe BP are trying to buy NWBO at depressed price.
The ROI is coming
How long have you been spreading BS? Eight years? What a waste!
Haha Vegas has it at 1,000 to 1 against an update from the mute nonmanagement crew. I'll take that bet.
(Sigh.) Another week gone by (including Sept. 17)...isn't it time for management to give us an update?
Complete and total nonsense, pulled straight out of your butt.
learningcurve2020,
Sorry if you couldn’t keep up. I do get in too much of a rush sometimes that leaves too many thoughts jammed together if I don’t review before sending. That is a well documented fault that I thank you for reminding me of so that I can be more careful next time; ). Best wishes.
Reefrad,
That is exactly the correct answer!; ). Until the breakthrough comes the burden of carrying the load and the perceived inequity of management gaining so many shares is rather obvious and can’t be ignored completely. However, when the breakthrough comes and the potential begins to be realized the retrospect view will see the burden as having been worth it and management motivated not to sell out cheap. Best wishes.
I don’t deny the facts . I seriously wish there was less red tape and less Bureaucracy so that the patients can get the treatment fast enough and lots of lives are saved . I am all for it and seriously feel for the loved one’s .
The whole discussion was that you can not ignore the fact that one of the major reasons people invest money ( including their retirement money) in stocks is for it to appreciate and get ROI as expected which is based on various things which may have been said or implied over a decade .
I think you have a point here.
you may be correct that nwbo has treated over 1000 patients in the compassionate care program. Wouldn't it be nice if the ceo would tell us that figure.
manibiotech,
Life and death decisions are being made by enforcement of “the process” and leaving patients no choice when they should have one. This is tantamount to homicide which some use “the process” to justify. However, when you run the numbers of patients who would be effectively cured if treated with L bs not being treated there is a problem with trying to justify “the process” when a new paradigm of safe and effective treatment has emerged. So yes, I use the word homicide because patients are being kept from life saving treatment because there are those justifying this based on upholding “the process” that keeps a significant group of patients from what would keep them alive because there are economic considerations.
You are certainly well aware of how automobile recalls are done based on cost of payouts vs cost of recall. It’s an economic decision by many companies based on the dollar value of lives impacted or lost. Regulators of drugs and other treatments are charged with first “do no harm” when considering new treatments and care of patients. That is a little different than what auto manufacturers and laws surrounding them are charged with so when I talk about regulators with regard to “the process” I am pointing out their accountability to this charge.
So think about a current example with checkpoint inhibitors trying to move from IV administration to subcutaneous administration. Both carry a risk of death from use but subcutaneous injection so far has demonstrated an increased risk of death from use compared to IV administration in the attempt to demonstrate non inferiority of treatment effect. In Germany, this attempt to protect patent rights likely would face a huge hurdle since the increased risk of death from sub cutaneous administration would be a major concern. The question facing BMY and their December padufa date is will FDA be as concerned. I wonder if patients think they should be. I know I would be if I was a patient especially if a regulator is supposed to protect me against anything that would do more harm than an existing treatment. L is better than current SOC and in some cases might actually be more effective without part or all of SOC and the harm that does without improved outcomes in some patient subtypes. Best wishes.
Just a stream of nonsense without even the courtesy of paragraphs.
How come I don't even know if I get paid? You don't like my posts. You may think I am a liar. But the data are real. I share something I truly believe and I always cite some facts. What about you? You are spreading doubts, fabrications, and casting negativity. Do you know you are missing this once-in-a-life investment opportunity?
Here is the latest news. BMS keep laying off people. Have you noticed what kind of portfolio BMS have been building to fight cancer? It is precision medicine! My conjecture is that DCVax-L as a platform is essential for the development of precision medicine. Time will tell if my conjecture is right.
Bristol Myers Squibb axes 79 more in New Jersey as $1.5B cost-reduction program rolls on
https://www.fiercepharma.com/pharma/bristol-myers-squibb-axes-79-more-nj-15b-cost-reduction-program-rolls
The “majority” of the savings from the Strategic Productivity Initiative—as it has been dubbed by the company—“will be reinvested to fund innovation and drive growth,” a BMS spokesperson wrote in an email Friday.
“As part of this initiative, the company is focusing resources on R&D programs with the potential to deliver the greatest return on investment, prioritizing investing in key growth brands and optimizing operations across the organizations,” BMS' spokesperson added.
suit,
What are you talking about? That post is of great interest to NWBO investors.
The trials that are linked are two PII trials involving dendritic cell vaccination in combo with pembrolizumab. These two studies are highly relevant and quite significant for NWBO (the two Roswell studies below are in addition to the ongoing UCLA study for rGBM that also includes pembrolizumab).
The United States Department of Defense is listed as a collaborator on one of the Roswell trials, and Merck’s pembrolizumab is being used in both of these studies.

https://clinicaltrials.gov/study/NCT04348747

https://clinicaltrials.gov/study/NCT05539365

https://physicianresources.roswellpark.org/news/roswell-park-clinical-trials-offer-novel-immunotherapies-for-advanced/metastatic-tumors-refractory-melanoma


https://www.prnewswire.com/news-releases/northwest-biotherapeutics-announces-exclusive-in-license-of-portfolio-of-dendritic-cell-technology-and-intellectual-property-302174237.html
“The license includes 5 new patent families that were just filed in 2023 and hence have their full potential patent life ahead of them. The technologies include enhanced versions of dendritic cells (DCs) and DC based therapies, as well as conditioning regimens designed to enhance patient responses and approaches to reprogram the tumour microenvironment to boost immune therapies and help overcome resistance to checkpoint inhibitors.
The DC based therapies include versions with tumour antigens loaded into the DCs and versions for intra-tumoural administration without pre-loading of antigens. Phase 2 trials involving the licensed technologies for two different cancers opened for enrollment earlier this year and are currently under way, and a third phase 2 trial for a third cancer is pending. The trials are fully funded by grant funding and are being conducted as investigator led trials. The company does not anticipate having to provide any funding or undertake any operational role for these trials.
As previously reported, over time the company has been quietly in-licensing various technologies and IP from various institutions and entities which it believes can be valuable in building a leading franchise in dendritic cell therapies.
The portfolio in-licensed from Roswell Park is complementary to, and builds upon, a portfolio which the company exclusively licensed from another institution last year. Together, the two portfolios encompass more than 20 years of work by one of the foremost groups of dendritic cell experts, led by Dr. Kalinski.
The portfolio in-licensed last year includes the foundational technologies and IP, and positive early-stage clinical trial results, developed by the Kalinski group over 17 years before coming to Roswell. The portfolio in-licensed now includes the further work during the last 7 years at Roswell. Taken together, the company believes that the two portfolios comprise a whole that is greater than the sum of its parts and offer compelling synergies with the company’s own portfolio. The company plans to collaborate with Dr. Kalinski on the further clinical development of the combined technologies.”
https://investorshub.advfn.com/boards/read_msg.aspx?message_id=175085456

The following are all the dendritic cell clinical trials sponsored by DoD. It seems like they all are connected to NWBO in some way. Did LP mention at ASM that NWBO has collaboration with academic institutions other than Roswell Park?
— d_stock (@d_stock07734) September 20, 2024
A First in Human Dose Escalation of… pic.twitter.com/IffpGJaBy1
Please just stop, you are embarrassing. I know you are getting paid, but still bro.
The more these pumpers post non sense, the more it becomes clear that you don't want to be a bagholder after UK approval spike!
exwannabe,
Direct needed tech transfer and also has been improved upon which may require a new IND. in the mean time product release issues that will also affect Direct have been in process of being worked out both by NWBO and regulatory guidance. You know that NWBO wanted to include the Roswell Parks tech in the next iteration of Direct and that agreement has been worked on for the last 2 years. So you see, NWBO has been building up their relationship with MHRA through the Specials program which has provided substantial additional data from use of L outside the full parameters of the Phase 3 trial. That is going to help speed up all future trials and give MHRA a chance to really demonstrate leadership in a field that lays the groundwork for potentially all future cancer care treatment and beyond. Best wishes.
The present and future of bispecific antibodies for cancer therapy
https://www.nature.com/articles/s41573-024-00896-6
The above is a paper on t-cell engagers both approved and under clinical trials. All the targets adopted by those t-cell engagers can also be found on brain tumor cells from the poly-iclc trial. The interesting part is that it seems like HER2 needs to be taken care of specifically. Roswell looks like having some know-how to target HER2 specifically.




Dendritic Cell Vaccines Against Her2/?Her3 and Pembrolizumab for the Treatment of Brain Metastasis From Triple Negative Breast Cancer or HER2+ Breast Cancer
https://clinicaltrials.gov/study/NCT04348747
Dendritic Cell-Based Treatment Plus Immunotherapy for the Treatment of Metastatic or Unresectable Triple Negative Breast Cancer
https://clinicaltrials.gov/study/NCT05539365
“ROI includes patient lives changed for the better. Others here share the same view. Best wishes.”
Here you clearly imply others meaning all others except you in common English . I don’t see “ some of us “ or “ many of us “ .
You start bringing up irrelevant and nonsensical topics like homicide , law etc etc in a simple discussion that the primary reason people invest in Wall Street is for ROI. But you go on irrational rant not relevant to this simple concept . But go right ahead .
JTORENCE,
Very likely true about what the Chinese would have done. Best wishes.
manibiotech,
Your “all” is not my “many”. Putting the word all in quotations and attributing it to me is misquoting me. I do not speak for all, rather for myself, but I do agree with many who are here and I do appreciate all honest opinions whether I agree with them or not, including yours. Best wishes.
I agree with you. At the same time if this thing ever succeeds we will be fine also. I know it doesn’t seem like it now but approval in the UK will turn everything around.
That's very believable
You are free to think what you like . I am fine with my belief
|
Followers
|
1640
|
Posters
|
|
|
Posts (Today)
|
24
|
Posts (Total)
|
721330
|
|
Created
|
02/02/05
|
Type
|
Free
|
| Moderators flipper44 sentiment_stocks CaptainObvious Poor Man - Doc logic JerryCampbell | |||
![]()
“Now this is not the end. It is not even the beginning of the end. But it is, perhaps, the end of the beginning.”
~ Winston Churchill

Stylized Dendritic Cell featured on NWBO board since 2015

- Dr. Linda Liau, PhD, MBA, Professor and Chair, Department of Neurosurgery, David Geffen School of Medicine at UCLA
Clinical Trials
DCVax®-L to Treat Newly Diagnosed GBM Brain Cancer (NCT00045968) - Phase III (Double Blind)
UK (MHRA): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
DE (Germany - PEI): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
Expanded Access Protocol for GBM Patients with Already Manufactured DCVax®-L Who Have Screen-Failed Protocol 020221 (NCT02146066) (Expanded Access)
Safety and Efficacy Study of DCVax-Direct in Solid Tumors (NCT01882946) - Phase I/Phase II (Open Label)
UK Clinical Trials - Study of a Drug (DCVax®-L) to Treat Newly Diagnosed GBM Brain Cancer
EU Clinical Trials for DCVax-L - Phase III
Dendritic Cell Vaccine for Patients with Brain Tumors (NCT01204684) - Phase II - at UCLA - Randomized (Open Label) testing DCVaccine with Resiquimod and DC Vaccination with Adjuvant polyICLC
Pembrolizumab and a Vaccine (ATL-DC) for the treatment of Surgically Accessible Recurrent Glioblastoma - Phase 1 (NCT04201873)
Dendritic Cell-Autologous Lung Tumor Vaccine (DCVax-L) and Nivolumab in Treating Patients with Recurrent Glioblastoma - Phase 2 (NCT03014804)
Dendritic Cell Therapy for Brain Metastases From Breast or Lung Cancer (NCT0368765) - Phase 1 - Collaborator: Mayo Clinic
Announcement of DCVax-L and Anti-PD-1 Monoclonal Antibody (Pembrolizumab) for Patients with Liver Metastases of Primary Colorectal Carcinoma Phase 2 Trial - November 17, 2016 - University Medical Center (UMC) of the Johannes Gutenberg University of Mainz
Cognate Bioservices - Owned by Charles River Labs
Website
Company Contact Info
Investor Relations:
Les Goldman (Company) (202) 841-7909 lgoldman@nwbio.com
Sign up for Northwest email list here (hit the subscribe to email list button in the lower right)
Company Headquarters
4800 Montgomery Lane, Suite 800, Bethesda, MD 20814 (240) 497-9024
NW Bio is developing cancer vaccines designed to treat a broad range of solid tumor cancers more effectively than current treatments, and without the side effects of chemotherapy drugs. NW Bio’s proprietary manufacturing technology enables them to produce its personalized vaccine in an efficient, cost-effective manner. NW Bio has a broad platform technology for DCVax dendritic cell-based vaccines.
Their lead product, DCVax-L, is currently in a 331-patient Phase III trial for patients with newly diagnosed Glioblastoma multiforme (GBM), the most aggressive and lethal brain cancer. This trial is currently underway at 69 locations thoughout the United States, Germany and the United Kingdom. NW Bio has also conducted a Phase I/II trial with DCVax-L for late stage ovarian cancer together with the University of Pennsylvania.
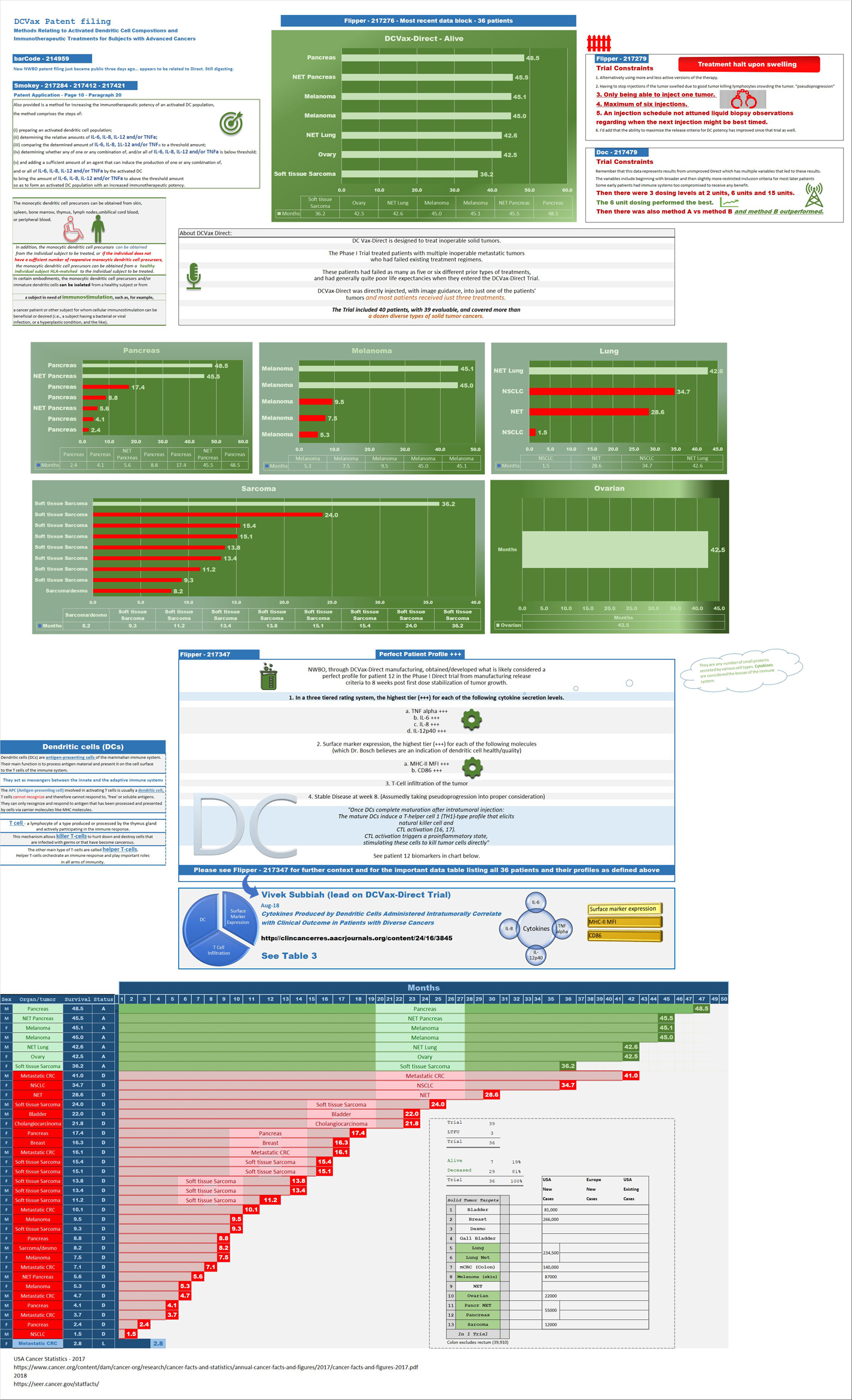
Their second product, DCVax-Direct, is currently in a 60-patient Phase I/II trial for direct injection into all types of inoperable solid tumor cancers, with trials currently being conducted at both MD Anderson Cancer Center in Texas, as well as Orlando Health in Florida.
They previously received clearance from the FDA for a 612-patient Phase III trial with its third product, DCVax-Prostate, for late stage prostate cancer.
DCVAX Survival Stories & Testimonials
Alice - Metastic Merkel Cell patient from Florida - ASCO 2018
Brad Silver - GBM patient from Huntington Beach, California - ASCO 2018
Sarah Rigby - GBM patient from Hong Kong - ASCO 2018
Kristyn Power - daughter of GBM patient from Canada - ASCO 2018
Kat Charles - GBM patients from UK - ASCO 2018 - as related by her husband Jason (Kat's Cure)
Prospective patients may contact NW Bio at patients@nwbio.com
UCLA Jamil Newirth DCVax-Patient Video - 2015
Allan Butler Video - National Geographic Vice President - DCVax-Direct patient from Phase 1 Trial with Pancreatic Cancer
NWBO - Patients Sunday Dennis and Jami Newirth - Enrolled at UCLA - Vimeo, Uploaded approx. May 2015
NWBO - Vaccine Helps Keep Brain Cancer Patient Alive (Jennifer Sugioka) - NBC Channel 4, Southern California, February 24, 2015
NWBO - National Geographic's Allan Butler Stage IV Pancreatic Patient using DCVax-Direct at MD Anderson
NWBO GBM Brain Cancer Survival Story of Mark Pace

Presentations

UCLA Agreements
Prostrate
DCVax-Phase II
DCVax-Booster
Upcoming Events
Videos
Linda M. Liau, MD, PhD, MBA - April 24, 2019 at University of Washington, Neurosciences Institute
| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |



