SequestOx was used by 163 bunionectomy patients during the PIII trials in 2014 with NO problems. The only problem with the drug was the Tmax value taking longer than the comparator drug used. The FDA said this could be remediated by a label warning then they changed their minds.
In our meeting with the FDA in November of 2014, Dr. Hertz requested three extra studies:an efficacy study (a Bunionectomy),an anti-abuse study and a BE study - sorry, it was a withdrawal study and a BE study. We indicated that we know that there is a food effect on our product so why are we doing another BE study for fed? FDA clearly stated that this is not a pass or fail, it’s a BE for labeling issue. We complied and we ran the study. We ran a three armed study: SequestOx fed intact, the capsule with a fatty meal; SequestOx sprinkled on applesauce with a light meal - bagel cream cheese, yogurt and applesauce - over 400 - 500 calories - and the brand. The fatty meal,as expected, showed that we are bio-equivalent for the AUC and Cmax but not the Tmax. For the light meal we were bio-equivalent for all three; AUC, Cmax and Tmax.
Let me very quickly summarize, when you’re on SequestOx against the brand on fasted conditions we are bioequivalent for AUC, Cmax,and Tmax. When you compare SequestOx in the fed condition using a light meal - a bagel,cream cheese, yogurt and applesauce - that’s sprinkled we are also bio-equivalent under AUC, Cmax and Tmax. When you compare SequestOx under fed conditions - a fatty meal, the brand and SequestOx are bio-equivalent for AUC and Cmax but not Tmax. What that means is that there’s a delay in getting the effect. We also ran 163 patients in a Bunionectomy that met all its primary points. The Bunionectomy was critical in that these patients ate wherever they fed them at the hospital or the clinic and they went home and ate whatever they wanted for the remainder of the week. The results were successful and we met all of our primary end points.
Historically, again, with this tremendous success and a small effect from the food it would have been a labeling issue where you instruct the patients to take the drug an hour before a meal or two hours after a meal. As a matter of fact that was the FDA’s stand when we met with them in 2014. FDA today believes that this is a safety issue and this is exactly what they told us and I’m quoting from the FDA’s complete response letter: “The extent of the delay in the absorption and peak concentration of oxycodone from SequestOx under the fed conditions is unacceptable as it places patients at risk of unintentionally overdosing” the FDA goes on to say because the proposed indication is for acute pain and the product is to be taken as needed product labeling with a specific food recommendation cannot fully mitigate this risk”.
Sorry wrong, FDA never said no to : Reformulated Patent Pending SequestOx™ is the SAFEST IR Opioid in the World. It will easily receive Oral (chewing) Abuse Deterrent Labeling like no other IR ADF Opioid has.
Here’s how it works:
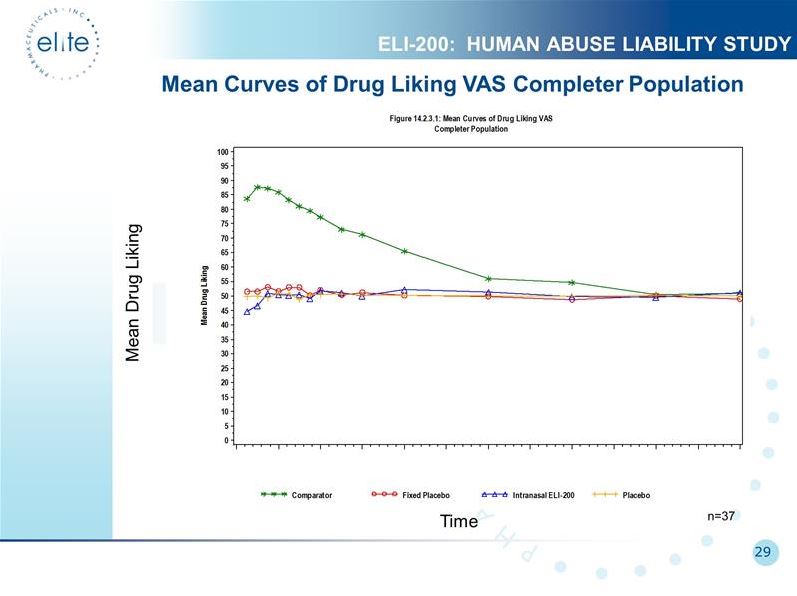
FDA validated the entire ER ADF line of ELTP 2 bead antagonist ADF tech works. It works very well, and it will also work very well for any opioid agonist with any time-release. Below is the ELI-200 nasal abuse HAL study. Recreational users thought ELI-200 (blue line) was same as placebo (red and yellow lines). Actually, they initially disliked it, and they never started liking it. The blue line never rises above placebo throughout the duration of the test. No doubt the antagonist bead works great. (The agonist bead is supposed to be the easy part.) FDA did not find one issue with Elite 2 bead ADF except for fed Tmax which only applies to IR opioids. Not one issue with HAL studies.
Quote:
"the FDA made no comment about Elite’s technology because it works and it’s solid. They made no comment on the human abuse liability studies because again they were solid and they work; or with the withdrawal study or the efficacy study – the Bunionectomy. This is great news for Elite’s ADT platform. There is no effect on Elite’s ER formulations"
ELTP 2 bead antagonist ADF tech works. It works very well, and it will also work very well for any opioid agonist with any time-release. Below is the ELI-200 nasal abuse HAL study. Recreational users thought ELI-200 (blue line) was same as placebo (red and yellow lines). Actually, they initially disliked it, and they never started liking it. The blue line never rises above placebo throughout the duration of the test. No doubt the antagonist bead works great. (The agonist bead is supposed to be the easy part.)
Recent Pilot study for Re-formulated SequestOx validated entire lineup of IR ADFs Now Elite's tech can be used on all IR opioids Pilot Study: shows a positive FedTmax for SequestOx which was the ONLY ISSUE with the IR ADF lineup.
Q The only issue with SequestOx™ was the FedTmax. That was fixed months ago the PR was early this year. See below for supporting link and exceptional results.
Quote:
“We resolved that issue and our patent attorney, Dr. Smith determined that this is something patentable and we will be filing a patent sometime next week.”
IR SequestOx™ will establish a New Standard of Care 2020-2021. The most frequently abused opioids are currently immediate-release (IR) opioids.
In 2016 93% of new opiod RXs were for IR(Immediate Release) opiods.
Reformulated SequestOx™ with lowered fed Tmax is the SAFEST Immediate Release opiod in the world, and the only one using a Pharmalogical Approach to abuse deterrence.
According to data from “Do abuse deterrent opioid formulations work?” Richard C. Dart, MD, PhD; Janetta L. Iwanicki, MD; Nabarun Dasgupta, PhD; Theodore J. Cicero, PhD; Sidney H. Schnoll, MD, PhD, in the Journal of Opioid Management 13:6, November/December 2017, reported that Immediate Release (IR) opioids are 4.6 times more likely to be intentionally abused and 6.1 times more likely to be diverted than Extended Release (ER) formulations. Not surprisingly, cited in the aforementioned work is a real-world study of 300 opioid abusers entering treatment for substance abuse who indicated they prefer abusable IR opioid products because they provide faster onset of the rewarding effects.
 News
News  Market Data
Market Data  Discover
Discover