 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.



flipper44
![]()
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Good Thai food does that every time.

So does mine. In more ways than one!

Oh man, even more stuff!?!?
The amount of amazing stuff that is coming up is imminent and significant. Afford567

Jeez, you are moving a ton of stuff!

Great!
Answer 1. Overcoming local and systemic tumor immune suppression is enough to completely eliminate cancer from the body over time (IMHO) if you are also using the full complement of tumor biomarkers. ICT-107 and other gene jockey methods not only do not use partial maturation to overcome local and systemic tumor and tumor microenvironment immune suppression, but they also hamstring themselves by only using a few random antigens when there are hundreds of tumor antigens, and even different antigens in different tumors throughout the body.
If DCVax-Direct used perfect partial maturation but only a few antigens, it would not be enough. If DCVax-Direct used all the antigens available in all the tumors, but it did not use perfect partial dendritic cell maturation, it would not be enough. Thankfully, DCVax-Direct did not skimp on its technology.
Answer 2. This technology was developed and perfected over many years. The DCVax-Direct preclinical and clinical trial pathology, observations and other results thus far present no reason to suggest the mechanism of action is significantly different than the MOA Bosch and Boynton perfected their patents upon, and that Liau and Prins helped develop through their work at UCLA.
Thus the title for the 2014 SITC abstract should, for all intensive purposes be claiming a result that is based upon the MOA that was/is being carefully perfected to the exact hour and dose -- even in the upcoming phase 2 multi-injection trial starting this fall. That perfection is being conducted based upon well documented advantages previously described and detailed by Doctor's Bosch and Boynton in their patents, by NWBIO in their literature, by other similar peer reviewed preclinical and clinical trials, including the recent phase 2 DCVax-Direct trial abstract published by UCLA -- and indirectly by many other dendritic cell preclinical and clinical trial efforts. (You may have noticed, I've been going to the trouble of reprinting and explaining more NWBIO literature today.) IMHO.
We and a few other companies are taking a different approach, based on the belief that existing dendritic cells in situ in a patient’s body are impaired, and their ability to receive and process the necessary signals is blocked. Under this view, if the signaling is blocked, then no matter how “loud” the signal may be, it will not get through and will not achieve the activation needed. Our DCVax-Technology unblocks and re-establishes the flow of signals through delivery of a fresh set of newly matured, activated and educated dendritic cells, which the tumor has not had a chance to paralyze or impair to block the flow of signals. Source: NWBIO
[P]artial maturation of the immature dendritic cells down regulates cytokine receptors on the surface of the cell rendering them less sensitive or responsive to any [tumor induced] immunosuppressive effects of cytokines present in the intratumoral space and provides for [dendritic] cells that can efficiently process tumor antigens present within the intratumoral space. -- DCVax-Direct patent
A diagram of some key agents and weapons of the immune system is set forth: (Also see explanation following diagram)
( Note:Keep thinking about this sentence as you digest this information: "Activated autologous dendritic cells injected intratumorally are able to overcome local and systemic immune suppression imposed by the tumor and its microenvironment.")
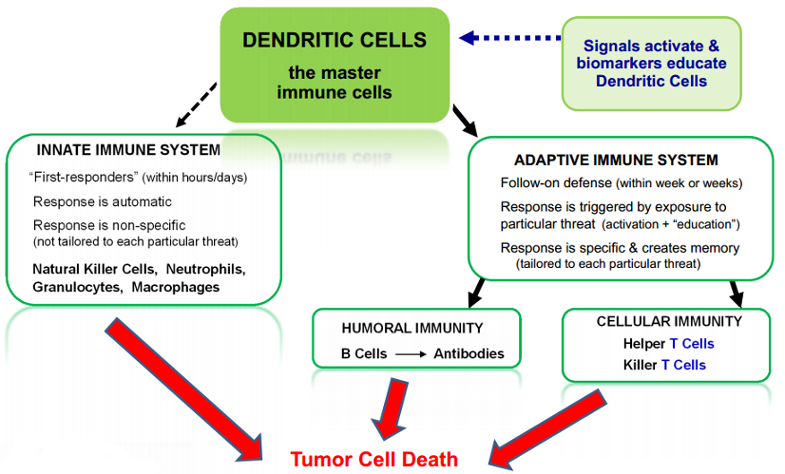
It has taken decades of research to identify the many different types of agents and weapons, to determine the relationships among them, and to determine how they work together to attack and defeat invaders such as bacteria, viruses and cancers. While the research was in process, early versions of immune therapies against cancers were tried, with mixed results and a number of failures. Over the course of the 1990s and 2000s, the first commercially successful category of immune agents to treat cancers emerged: drugs that consisted of individual antibodies, such as Avastin, Herceptin and Erbitux. These are considered passive immune therapies (in contrast to dendritic cell and T cell therapies which are considered active immune therapies).
Antibodies are just one category of weapon in the overall immune “army,” and there are many, many kinds of individual antibodies within this category. Each antibody drug, such as Avastin, consists of just a single one of the many kinds of antibodies within this one category of immune system weapon. These drugs do not involve or make use of the numerous other important agents in the immune army, such as T cells, NK cells, and so on.
Antibody drugs have been moderate medical successes and huge commercial successes. These drugs have delivered moderate extensions of patient survival compared with traditional chemotherapy drugs, with somewhat lesser (though still significant) toxicity. On this basis, these antibody drugs are achieving multi-billion dollars per year in sales.
Now, more broad based immune therapies are starting to come of age: “therapeutic vaccines” designed to mobilize the entire immune system “army,” rather than just a single agent or single category of agents. Therapeutic vaccines are similar to preventive vaccines in that they work by mobilizing the immune system. However, therapeutic vaccines are administered to patients who already have a given disease, for the purpose of preventing or delaying recurrence or progression of the existing disease.
Several of the therapeutic vaccines that are now coming of age are focusing on dendritic cells in various ways, or on T cells. The vaccines focusing on dendritic cells offer a broader potential immune response because dendritic cells are the master cells of the immune system — as noted above, they are the “General” of the immune system “army.” When dendritic cells are activated against a particular pathogen (or cancer) they, in turn, mobilize all of the other agents (including T cells as well as B cells, NK cells and others) to attack that pathogen (or cancer). The process by which dendritic cells communicate to and mobilize other agents takes place to a large extent in the lymph nodes.
A major challenge faced by immune therapies for cancer has been that, unlike in a healthy patient with an infectious disease, in cancer patients the dendritic cells fail to do their job, and the other immune agents also fail to do their job. Pathologists analyzing tumor tissue removed from cancer patients have long observed that there are often substantial numbers of immune cells in the surrounding tissue, but they are not infiltrating and attacking the tumor — as though the immune cells have made it to the doorstep of the tumor and then stopped.
The mechanisms by which cancer cells selectively suppress or block the immune system are still the subject of much research. It is known that cancer cells have many such mechanisms, including secretion of biochemical signals that jam normal immune signaling, that make tumor cells invisible to immune detection and/or that convey false messages to the immune system. Different therapeutic vaccines are taking different approaches to trying to overcome these cancer mechanisms and put the immune system back in action.
Many of the therapeutic vaccines for cancer (e.g., Cell Genesys, CancerVax) have targeted existing dendritic cells in situ in a patient’s body, by administering various compounds or factors that are designed to attract dendritic cells to the tumor or enhance the tumor signals to the dendritic cells (in essence, making the tumor signals “louder”).
We and a few other companies are taking a different approach, based on the belief that existing dendritic cells in situ in a patient’s body are impaired, and their ability to receive and process the necessary signals is blocked. Under this view, if the signaling is blocked, then no matter how “loud” the signal may be, it will not get through and will not achieve the activation needed. Our DCVax-Technology unblocks and re-establishes the flow of signals through delivery of a fresh set of newly matured, activated and educated dendritic cells, which the tumor has not had a chance to paralyze or impair to block the flow of signals. Source: NWBIO Website
Extensive scientific evidence has shown that there is substantial variation in tumor profiles and characteristics among patients with the “same” cancer. The degree of variation is particularly enormous in some of the most aggressive cancers, such as GBM brain cancer and pancreatic cancer. DCVax is designed to target the full set of biomarkers on a patient’s cancer. Such a treatment approach makes it more difficult for tumors to develop escape variants. Source: NWBIO Website
Pyrr penned a terrific article with great attention to current considerations.
In contradiction to what AF once said, there are many articles written about Dendritic therapy.
"During the last 13 mo (July 2012 - July 2013, both included), no less than 4,400 articles dealing with DCs have been published in peer-reviewed scientific journals (all types of publication confounded, source www.ncbi.nlm.nih.gov/pubmed/)."
I'm simply a poster with shares in NWBO. I have no other connection with NWBO whatsoever -- except perhaps my wish that cancer is but a memory. I read a lot, as do Pyrr and other posters.
I really am a very long investor, so I do not attempt to time the market. That said, here is part of a comment I just left on Pyrr's recent article:
On DCVax-Direct, your points regarding MDAnderson, UCLA, Orlando Health and Northwest Biotherapeutics mutually signing off that.... "Activated autologous dendritic cells injected intratumorally are able to overcome local and systemic immune suppression imposed by the tumor and its microenvironment," should be a wake up call to even the most jaded clinician, researcher, patient, investor and average citizen.
I remember the day it was clear to me (and a very small percentage of the public) that the Berlin wall would fall. It was very difficult to convince my friends why this was imminent. Now it is almost difficult to convince a young student how significant it really was. No matter, it fell....and I think you can purchase pieces of it on ebay:) -- Flip
Les Goldman's 2 cents on biotech Short manipulation.
(I say this indirectly, because the quote below suggests Goldman believes small biotech's are vulnerable to short manipulation, which is what the article was about, prior to crossing a particular threshold in market cap size.)
(May or may not be not be an accurate quote, because the author had a pro-AF agenda.)
“We’re still a small biotech company,” he adds. “If you’re looking for validations from major institutional investors, they start playing with somebody, if you will, when they approach a billion-dollar market cap.” Columbia Journalism Review quoting L. Goldman
I object to the misleading and false statements intentionally and crudely shouted by AF from his bully pulpit. I know he knows the rules, and that is what makes his frequent lies and damn lies all the more infuriating.
I think 1-2 years for complete availability is spot on. 12 months - 18 months until global availability for DCVax-L, and 18 months to 24 months until global availability for DCVax-Direct. IMHO. I am sorry for your losses, and I believe those who went before us will somehow see this journey through with us.
One more time....
I'm pretty certain Roy has a different take on this.
Perhaps one must take it to the streets, in order to take it to The Street....
Hi Retiredinlovinglight,
Here is something I wrote recently, which kind of jives with your numbers.
Various potential scenarios in DCVax-Direct multiple injection (phase 2) trial starting this fall.
Let's imagine:
1. 24 pancreatic 100% response no recurrences. 24 lung 100% response no recurrences. 24 colorectal 100% response no recurrences. No major adverse side effects. I'd say they would approve it. (100%)
2. Change those numbers to 90%. Expand each indication to 60. I'd say they'd still approve it. (100%)
3. Change those numbers to 87%. Expand each indication to 120, I'd say they'd still approve it. (100%) IMHO
I won't get too caught up in analogies here, the proof will come in the pudding:) From here forward, I'm focused on results. Financially, NWBO can see themselves through phase I Direct results and phase III L results with minor/moderate financing. The trial results will either catapult us into the stratosphere, or they will not. I believe they will, and I think NWBO management is keeping their powder dry for November and December 2014. That will likely bring us up to a much higher base, then we will likely have a lull until the end of March 2015, a higher base, then another lull until ASCO in May/June and an astronomically high base. The advancements after that will be during such time that NWBO is a household name. IMHO.
Blessings to Ethan, his family and his community.
I'm afraid we are currently rocket scientists in this household, and my offspring and I fully intend to break the 1200 foot limit set by Quest Aerospace's rocket starter set. However, you may be gratified to know that our mutual brain power confirms your sensible conclusion.
It doesn't take a rocket scientist to figure out that all you needed to do to shut down Herr Feuerschtick is make an announcement of results with MD Anderson. -- DiamondJim
A symbolic gesture?
ASCO (Amercan Society of Clinical Oncology) shares the same side of the street with NWBO:)
I'm very sorry to hear about your dog. I hope that the animal vaccine will be rekindled once the human versions are marketed. Direct will likely be a much better option for animals, as many owners simply can't afford surgery plus treatment. Beyond pets, the global agricultural industry may help finance this technology as well.
Thanks antihama
[U.S.] [s]pending on all oncology drugs hit $28 billion in 2013, an increase of 9.2% over the previous year, according data from drug market research firm IMS Health. The average cancer prescription now costs 22 times more than it did a little over a decade ago, according to Express Scripts, a company that manages pharmacy benefits. -- Milwauke Journal Sentinel
Granted, an Artist's rendering.
Still, timeless discoveries provide elegance.
Nanotube and Bucky-Ball
Serene Structure for Engineers
Dendritic Cell and Double Helix
Exquisite Entanglement for Biologists
Carbon Atom and Water Molecule
Continuous Composition for Chemists
Relativity and Quantum Mechanics
Certain Chance for Physicists
Granted, an Artist's rendering.

The current short interest numbers only bring it current to October 15, 2014. Any short covering since that time will not be reported until November 11, 2014, and that will only reflect short interest through Halloween.
How DCVax-Direct Overcomes Local and Systemic Tumor Immune Suppression.
(Reprinted for a better sticky title.)
I'm going to try and explain this at a more digestible level -- per request.
1. DCVax-Direct (Dendritic cells) is/are injected into a cancer tumor.
2. DCVax immediately secretes (releases) massive amounts of cytokines (natural chemicals) that kill tumor cells, create inflammation and signal the innate (early) immune system (e.g. Natural Killer Cells) to respond. This is just the beginning.
3. The DCVax dendritic cells start nibbling on the dead tumor debris. Because these are special dendritic cells, the tumor cannot use its normal toolkit of different cytokines (natural chemicals) to stop the dendritic cell from ingesting this dead tumor debris. Just call them the teflon DCs.
4. After dining on the tumor debris, the dendritic cell processes the dead tissue into tinier fragments scientists call antigens, and the DC actually displays these dead tumor parts (antigens) on the dendritic cell surface. Again, normally the tumor environment would stop or interfere with dendritic cells trying to process and display dead tumor debris (antigens), but not our DCVax dendritic cells. They are like super-mailmen undeterred by local lousy conditions, and intent on making their appointed rounds.
5. Now the dendritic cells escape the tumor micro-environment laden heavy with a dense coating of tumor antigens on their surfaces. Again, here the DCVax-Direct dendritic cell carries far more antigens packed upon its surface than any common dendritic cell might.
6. Next, the dendritic cell literally crawls through the extracellular matrix toward a nearby lymph node. Again, the DCVax dendritic cell is not slowed by the prior tumor environment attempts to weaken it before its journey.
7. Upon arrival at the lymph node, most dendritic cells would have been previously weakened by chemicals released by the tumor microenvironment both inside and outside the tumor; instead, the DCVax dendritic cell is still completely able to (hyper) activate t-cells and b-cells to multiply and attack the intended target.
8. These t-cells and b-cells are so well instructed/activated that they immediately proliferate into the millions and seek out tumor cells throughout the body.
9. The primary tumor, now weakened by the dendritic cytokines and innate immune system, is attacked by the SUPER t-cells and b-cells. Next, other tumors throughout the body are likewise attacked.
10. These members of the adaptive immune system are not fooled or blocked by the tumor, as non-DCvax activated t and b-cells might otherwise be. They finish off the tumors and store their description in long lived memory cells that will mount a faster immune system attack should the same cancer try to return.
Dendritic Cell.
An easy summer read, a light bedtime story.....not!
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3841205/
OK. I'm going to try and explain it at a more digestible level.
1. DCVax-Direct (Dendritic cells) is/are injected into a cancer tumor.
2. DCVax immediately secretes (releases) massive amounts of cytokines (natural chemicals) that kill tumor cells, create inflammation and signal the innate (early) immune system to respond. This is just the beginning.
3. The DCVax dendritic cells start nibbling on the dead tumor debris. Because these are special dendritic cells, the tumor cannot use its normal toolkit of different cytokines (natural chemicals) to stop the dendritic cell from ingesting this dead tumor debris. Just call them the teflon DCs.
4. After dining on the tumor debris, the dendritic cell processes the dead tissue into tinier fragments scientists call antigens, and the DC actually display these dead tumor parts (antigens) on the dendritic cell surface. Again, normally the tumor environment would stop or interfere with dendritic cells trying to process and display dead tumor debris (antigens), but not our DCVax dendritic cells. They are like super-mailmen undeterred by local lousy conditions, and intent on making their appointed rounds.
5. Now the dendritic cells escape the tumor micro environment laden heavy with a dense coating of tumor antigens on their surfaces. Again, here the DCVax dendritic cell carries far more antigens packed upon its surface than any common dendritic cell might.
6. Next, the dendritic cell literally crawls through the extracellular matrix toward a nearby lymph node. Again, the DCVax dendritic cell is not slowed by the prior tumor environment attempts to weaken it before its journey.
7. Upon arrival at the lymph node, most dendritic cells would have been previously weakened by chemicals released by the tumor microenvironment both inside and outside the tumor; instead, the DCVax dendritic cell is still completely able to fully/hyper activate t-cells and b-cells to multiply and attack the intended target.
8. These t-cells and b-cells are so well instructed that they immediately proliferate into the millions and seek out tumor cells throughout the body.
9. The primary tumor, now weakened by the dendritic cytokines and innate immune system, is attacked by the SUPER t-cells and b-cells. Next, other tumors throughout the body are likewise attacked.
10. These members of the adaptive immune system are not fooled or blocked by the tumor, as non-DCvax activated t and b-cells might otherwise be. They finish off the tumors and store their memory in long lived memory cells that will attack should they try to return.
Thanks Evaluate!
[T]he word cure is certainly on the tip of all of our tongues as we're treating patients with immunotherapy agents".
Good points Pyrr. I thought I'd throw this in from the 2012 DCVax patent for those who are interested.
In it, please note that partially mature dendritic cells can uptake tumor debris, process antigens, present antigens at higher density levels and create stronger t-cell activation. The SITC statement confirms DCVax-Direct is able to do this without interference by the tumor microenvironment both within the tumor and systemically (e.g.. at the lymph during presentation and activation)!
Greater MHC expression leads to an increase in antigen density on the DC surface, while up regulation of costimulatory molecules CD80 and CD86 strengthens the T cell activation signal through the counterparts of the costimulatory molecules, such as CD28 on the T cells. Partially mature dendritic cells as used in the present invention typically comprise those dendritic cells that once exposed to a dendritic cell maturation agent demonstrate an up-regulation of expression of a co-stimulating molecule including, but not limited to, CD80, CD86 and/or CD54. The cell may or may not express CD83, but maintains the ability to uptake and process antigen. Further, the partially mature dendritic cells may produce TNF-a, IL-6, IL-10 and or IL-12 which are not typically produced by immature dendritic cells.
Fully mature dendritic cells are not preferred for the present invention because they do not efficiently process antigen. Further, immature dendritic cells as used in prior methods are not desired because the immunosuppressive environment typically found within a tumor, including substantial concentrations of cytokines known to prevent the processing of antigen by immature dendritic cells. In the present invention, partial maturation of the immature dendritic cells down regulates cytokine receptors on the surface of the cell rendering them less sensitive or responsive to any immunosuppressive effects of cytokines present in the intratumoral space and provides for cells that can efficiently process tumor antigens present within the intratumoral space. Once the partially mature dendritic cells have matured within the tumor as measured by the production of, for example, TNF-a and IL-12, and the expression of the chemokine receptor CCR7, the cells can migrate to the lymph nodes where the cells will contact T cells to up regulate the immune response to the tumor antigens.
Afford, to me, the title suggests DCVax-Direct works exactly the way it is supposed to. Bosch, Boynton and Liau have been tinkering and collaborating over the past 10-15 years to perfect DCVax-Direct. This includes but is not limited to perfecting resistance against tumor suppression, increasing initial cytokine induced tumor death, increasing uptake and expression through proper maturity, eliminating dendritic cells prior to injection that would have the opposite effect, increasing t-cell proliferation, tumor cell targeting and the list goes on.
When Direct works the way it is supposed to, it stops, kills and eventually (over weeks and months) eliminates tumors from the patient. Finally, it should prevent cancer from returning (durability/immune memory). We are still awaiting future presentations to learn what degree of success these trials are demonstrating in humans.
Yes, I am in agreement with Pyrr's statement, but it should read "tumor necrosis." (not just necrosis). However, you must also hit the right target. That is why the section I highlighted in red below is included in my last message.
IMHO, systemic immune suppression imposed by the tumor does not just mean against the dendritic cell, it means against the entire immune response. Thus, if DCVax-Direct is able to overcome all the "tricks" used by the tumor microenvironment to otherwise effect immune suppression within the tumor itself (locally) and throughout the body (systemically), then all that is left to accomplish is tumor recognition, and as we know, DCVax-Direct uses the full compliment of tumor antigens to empower t and b cells to locate their target.
The title suggests that anti-PD1 therapies are not necessary for DCVax-Direct to overcome local and systemic immune suppression imposed by the tumor and its microenvironment.
Maybe this is a poor way for me to describe what the SITC NWBO title potentially means, but this is extremely significant because it intimates that adjuvants are not necessary to make DCVax-Direct effective.
If tumors cannot mount suppression against dendritic cells, one can infer that they are also not mounting effective tumor response against the t and b cells activated by the dendritic cells. This is why the last part of the SITC sentence is so important.
"able to overcome local and systemic immune suppression imposed by the tumor and its microenvironment."
By November 4, 2014, nearly 5 months will have gone by since the last significant DCVax-Direct update. That's a lot of pent-up data.
Best wishes to patients.
10 days until the embargo is lifted.
No it doesn't. It sounds like a small company doing far better than you could at developing an international infrastructure, new processing platform, intergovernmental relations for regulatory support, and oh yeah....a possible cure for cancer -- all on a relative shoe string budget.


