 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.






WeeZuhl
![]()
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Drug-Liking Curve Smackdown: Ventrela vs SequestOx
Ventrela looks decent on pharmacokinetics and drug liking, unless it is compared to gold-standard ELTP 2 bead pharma ADF. SequestOx wins, easily.

My son-in-law, who has worked on Wall Street for 25 years for three major investment firms, laughs every time I even mention shorting of any OTC stock. He reminds me that his ilk are really quite conservative types, and they would never short an OTC stock, given the potential for these stocks to skyrocket on good news.
I would believe it if I had a solid reason to believe it. I doubt that hedge funds even know we exist.

You've got know when to hold them and know when to fold them
June 7-14 makes me feel ELTP tingly.
Three year anniversary. Could it be the week?

Mazeppa, hope this helps...
Drug liking curves:
ELI-200:
Tarqiniq:

Remoxy:

Hyslinga:

One of the drugs, referred to as “16-8” proved successful at treating pain in mice including “abdominal aches” and “pancreas inflammation.”

New article on seeking alpha by Kempharm long.
http://seekingalpha.com/article/3978737-upcoming-shifts-abuse-deterrent-opioid-market-size-potential-upside-kempharm-small-biotechs
Upcoming Shifts In Abuse-Deterrent Opioid Market Size: Potential Upside For Kempharm And Other Small Biotechs In The Space
...
...Given that Kempharm will potentially have the first drug (Apadaz) with both abuse-deterrence properties and specific labeling as such by the FDA in accordance with the April 2015 document...
It's all about the label.
This article incorrectly refers to Pfizer's upcoming ALO-02 AdComm as their PDUFA date, but it gets the important part correct.
http://www.investing.com/analysis/here-are-two-large-cap-pharmas-with-pdufa-catalysts-next-month-200132618
The real question, and the factor on which the market will base its response to the ruling, will be the labelling. We’ve seen some pretty high profile examples of abuse deterrent candidate getting advisory approval this year so far, but not picking up an abuse deterrent label. This failure to get the labelling effectively renders the approval useless, as the pain management market is already crowded, and without a differentiating quality (i.e., abuse deterrence) there is no way a new drug can compete. As such, this is the part of the decision on which markets will be focusing.
The date to watch? June 8, 2016.
very nice! that almost looks like something the elite PRopaganda department would put together
Elite Pharmaceuticals ELTP



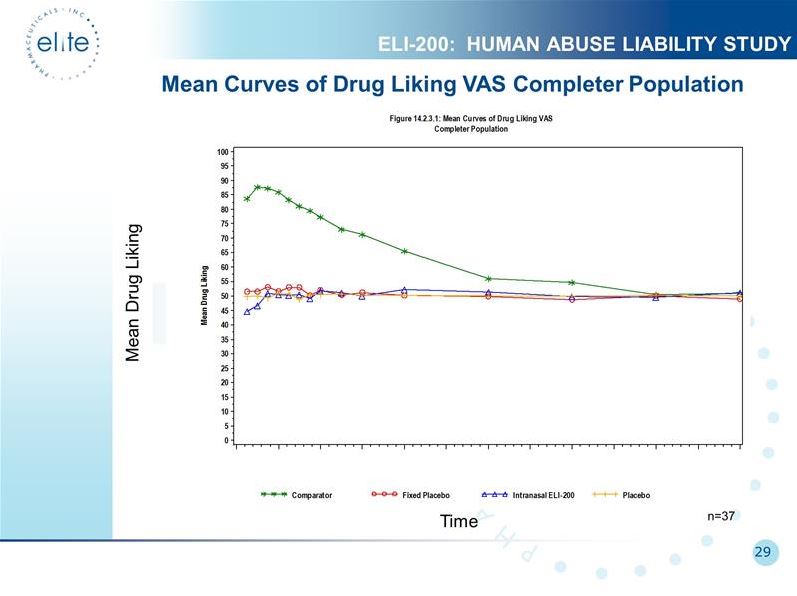
Shows Mean Drug Liking on Visual Analog Scale (VAS). Time is on horizontal axis. On the verticle axis, anything above 50 means they liked it, below 50 they disliked it. Notice the expected liking of snorted oxyIR (green). ELI-200 (blue) has ZERO drug liking, indicating an EFFECTIVE ADF. ELI-200 is *disliked* at the outset (blue line falls below the placebos (red & yellow)). This means it is an AVERSIVE ADF. Also, ELI-200 never bumps above the placebo line, indicating it is a DURABLE ADF.
ELTP 2 bead pharma ADF is EFFECTIVE, AVERSIVE, DURABLE, and MODULAR across the entire spectrum of opioid agonists and time-release profiles. Fully-licensable. The Golden Ticket.
Purdue's current technology works pretty well.
I am happy to criticize the notorious dose-dumping, easily-abused OxyContin. I've even implied that when better alternatives are available, OxyContin is at risk for FDA action due to its sketchy ADF. While that may be true, Purdue will never let that happen. I am certain they have OxyContin3 ready to go, probably using the Resistec technology they used for Hysingla (24 hour hydrocodone). Hysingla did receive the ADF label, and the pharmacokinetic and drug liking curves are reasonable. It's the exact same concept, a hardshell ADF that gums up when hydrated. But this formulation actually seems to work as an ADF. I'm sure that Purdue is trying to figure out a way to bring OxyContin3 to market such that they somehow weasel another 5 years of market exclusivity without generic competition, just like they did for OxyContin2. But even so, hopefully in the very near future they will have serious competition from multiple brand-name ADF's, including Xtampza, Rexista, ELI-201, and ALO-2.
http://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/206627Orig1s000CrossR.pdf
This article is very good, rollin2nyte.
http://marketexclusive.com/weekly-biotech-report-covering-novo-nordisk-nysenvo-sanofi-sa-nysesny-kempharm-inc-nasdaqkmph/6455/
The way to think of this is the abuse deterrent element of the drug is its efficacy. That benzhydrocodone hydrochloride and acetaminophen work to reduce acute pain was never in question, hence their current standard of care (SOC) status in just this indication. What was under scrutiny in this trial, and subsequently, in the review meeting, was the drug’s abuse deterrent qualities. Essentially, is it an improvement on the current SOC, with improvement defined as some sort of differentiation – specifically, that users cannot overdose or abuse the active compounds that make up the drug. This differentiation is the efficacy in this situation, and with the review panel voting against a label that highlights the drug as abuse deterrent, they are essentially saying that the drug is not effective.
This selloff reflects the fact that without abuse deterrence properties, the company’s pipeline is effectively composed of generic pain therapies, and in turn, is not likely to generate much in the way of sales going forward.
Fentanyl: Good, Bad, and Ugly
Fentanyl is mostly used in hospitals for IV drips and injections. Critical care docs tend to use a lot of fentanyl for sedation of intubated patients. There are no approved fentanyl tablets sold in the United States- nothing to add a naltrexone bead to. The only consumer product is Duragesic, the fentanyl patch. Duragesic is a great drug, the second most commonly prescribed opioid by me after oxyIR. The oldest of the olds seem to very nicely tolerate a 12 mcg patch, even if they never did well with oral drugs due to nausea, confusion, or somnolence. Some folks just plain out-live their spine and develop terrible degeneration and spinal stenosis, and I’ve gotten several up & moving again with a fentanyl patch when nothing else worked.
The patches can be abused by various measures, and there also have been deaths of children who accidently get hold of the patches. But the major problem with fentanyl is not abuse and diversion of patches or dead kids. The problem with fentanyl is that it is SYNTHETIC, and that is an extremely important difference. It may seem weird to think of OxyContin and SequestOx as agricultural products, but that is exactly what they are. All of the opioid drugs are manufactured from pharmaceutical API which is derived from industrial-farmed poppy. It requires massive infrastructure, including land and water and energy and workers and security and governance etc etc etc. But synthetic fentanyl is manufactured in a lab. All one needs is a decent chemist and access to the right compounds. With access to even rudimentary equipment, a devastating quantity of illicit fentanyl can be easily produced.
Heroin is also an agricultural product that requires massive infrastructure. It is no wonder that synthetic fentanyl has become cheaper and more readily available. But addicts actually try to avoid fentanyl because it significantly increases their tolerance to heroin and oxycodone. So dealers are cutting the more expensive, more desirable heroin with the cheaper, manufactured fentanyl, but they hide this from their customers. Unsuspecting addicts with high tolerance to heroin may not have cross-tolerance with fentanyl, and they have no idea how much they are injecting. Buyer beware. Fentanyl is especially killing people who do not even realize they are using it.
Illicit synthetic fentanyl is a big problem, but not one in which the ELTP antagonist ADF can be helpful.
great to see us over a million shares traded today.
There is no public data for Rexista.
Rexista is a hardshell ADF that gums up when hydrated to resist injection. IPCI says it is "difficult" to vaporize or inhale from burning. The technology could be applied to other agonists, but each will require reformulation.
IPCI has not to my knowledge ever disclosed any kind data, including HAL results. There are no pharmokinetic or drug liking curves available to compare, so nobody has any factual basis to say Rexista is any better or worse than any other hardshell ADF that gums up. One thing that confuses a lot of people is the overdose protection system known as PODRAS. It is purely conceptual, but the way IPCI has presented it tends to make some investors believe it is ready to file NDA now. PODRAS is years away from anything. Rexista with nPODDDs is the hardshell version supposedly ready to file NDA without Phase 3, so we'll get a look at the data soon enough.
One thing for sure Rexista does that Elite's platform does not:
http://files.shareholder.com/downloads/ABEA-43EQSZ/180376177x0x881307/0AA81A60-E645-4481-8DED-AD17516D579E/Roth_Investor_Conference_March_2016_upload_version.pdf
Abuse by grinding, chewing, licking, inhalation, snorting, and
insufflation releases a stigmatizing blue dye.
Another ADF implicated in serious heart damage.
The Canadians are learning about our pathetic game of Whack-A-Mole. Kill one drug, something else replaces it. Hydromorph Contin is time-release hydromorphone, which is better known as Dilaudid in this country, but I'm not aware of time-release Dilaudid available in USA. Very similar to the Opana ADF, the Hydromorph Contin ADF is easily injectable, but the extraction process introduces contaminates that cause big problems. A good reminder that just because a company says a drug is an ADF does not make it true.
http://www.ctvnews.ca/health/new-type-of-oxycodone-abuse-causing-spike-in-heart-infections-1.2912237
When the Ontario government banned OxyContin four years ago, the goal was to curb rampant abuse of the powerful painkiller.
But doctors in London, Ont., are now seeing people abuse the drug’s “tamper-proof” replacement – with gruesome consequences.
OxyContin -- a brand name for a painkiller called oxycodone – was removed from sale in 2012.
The use of a related painkiller, Hydromorph Contin, exploded after that - a formulation designed to thwart people from dissolving the pill and injecting it, it is designed to turn into a thick, gel-like substance when exposed to water.
When crushed and injected, fragments of the pill sometimes end up in the mixture. These shards can travel through the blood into the heart, scratching the organ’s interior and damaging valves.
The result, says cardiac surgeon Michael Chu, is an increase in strokes, blood clots and death among addicts. Chu specializes in repairing damaged valves at London Health Sciences Centre.
“Surgeons should shudder if they ever see this,” Chu says, pointing to a picture of a damaged heart.
“This is a hole into the left side of the heart. Basically the entire middle of the heart’s been cut out here because of infection,” he says.
ALO-02 will have exclusivity
but where are the clinical trials needed for such filing?
ELITE PHARMACEUTICALS REPORTS SUCCESSFUL PIVOTAL BIOEQUIVALENCE STUDY FOR ABUSE-DETERRENT OXYCODONE PRODUCT ELI-201
Posted on December 3, 2014
Northvale, New Jersey, Wednesday, December 03, 2014: Elite Pharmaceuticals, Inc. (“Elite” or the “Company”) (OTCBB: ELTP) announced today successful results from a pivotal bioequivalence (BE) study for ELI-201, Elite’s twice daily abuse-deterrent oxycodone product which utilizes Elite’s proprietary pharmacological abuse-deterrent technology.
There is no more versatile ADF platform.
(1)Oxycodone
(2)Morphine
(3)Hydromorphone
(4)Hydrocodone
This would be eight 505B2 NDA ADFs.
Nasrat Hakin keeps saying that he has ideas for 17 ADFs.
Some very interesting goings on recently around Opana “ADF” and generic oxymorphone formulations based on “original” Opana.
A lot of important background, some of which I’ve addressed in previous posts. The ADF version of Opana introduced by Endo in 2012 has been a complete disaster. Not only is the ADF version easily abused via intravenous injection, it is directly implicated in outbreaks of HIV and Hep C. The nature of the agonist requires frequent injections in order to avoid withdrawal, and the nature of the ADF requires large bore needles and extraction through steel wool, both of which are repeatedly shared and reused in a contaminated state.
http://investorshub.advfn.com/boards/read_msg.aspx?message_id=113693008
Additional background: when ADF OxyContin was introduced in 2010, Original OxyContin was subsequently deemed unsafe due to abuse potential and the NDA approval revoked by FDA. This was uncontested by Purdue because it gave them an additional 5 years of market exclusivity with the new ADF version. Still reeling from this stink, FDA refused any such favor for Opana, saying the ADF version was not an improvement over the original version and therefore the original Opana NDA was kept in tact.
http://www.fiercepharma.com/legal/endo-scores-victory-opana-er-generics-patent-battle
"We think the public health would not be served if a company can market itself as 'abuse deterrent,' if the scientific evidence did not support that claim," Douglas Throckmorton, a deputy director in the FDA's Center for Drug Evaluation and Research, said at the time.
Endo International Plc agreed to stop marketing its Opana ER painkiller pill as crush-resistant, and stop downplaying the risks of addiction associated with the narcotic, under a settlement with New York state announced on Thursday.
The company will also pay a $200,000 penalty.
State Attorney General Eric Schneiderman said Endo's own studies found that the pill could be crushed, but that the company's misleading marketing provided a false sense of security to doctors and patients, and might have boosted sales.
At issue in this case is the concept of patent protection. A drug manufacturer that brings a new product to market enjoys 20 years from the date of first patent filing to exclusively manufacture, market and ultimately profit from the drug.
Considering the time it takes to gain Federal Drug Administration (FDA) approval, the effective window a drug designing company has to maintain exclusive control is usually 7-12 years.
Enter the pay-for-delay concept that allows companies like Endo to pay generic drug manufacturers to delay bringing their versions of name brand drugs to market.
The FTC alleges that Endo paid up to $40 million to Impax to keep a generic version of Opana ER off the market for two years.
The U.S. District Court for the Southern District of New York has issued an order upholding its August 2015 ruling in Endo’s favor and confirming the court’s prior injunction against the manufacture or sale of the generic version of non-crush-resistant Opana.
In December 2012, Endo (NASDAQ: ENDP) filed a patent infringement complaint against Actavis. Endo, which is based in Dublin, Ireland, and has it U.S. headquarters in Malvern, Pa., filed additional patent infringement suits against several other generic drug companies that file applications to make generic non-crush-resistant Opana.
One of those companyies, Par Pharmaceutical, was later acquired by Endo for $8 billion. Other lawsuits were filed against Teva Pharmaceuticals (NYSE: TEVA) , Mallinckrodt LLC, Sandoz, Roxane Laboratories and Ranbaxy Laboratories. The suits against Par and Mallinckrodt were dismissed pursuant to settlements, and the suits against Teva and Sandoz were dismissed based on those companies’ demonstration to Endo that they are not seeking FDA approval to sell generic versions of non-crush-resistant Opana prior to the expiration of Endo’s patents.
Aurobindo Pharma on Thursday announced that it had received final approval from the Food and Drug Administration for its generic Opana (oxymorphone HCl) tablets.
Dear Purdue Pharma,
In the matter of your petition, we refer you to our previous reply in the matter of Arkell v. Pressdram.
Sincerely,
The FDA
Could happen any day, Lasers.
No FDA Advisory Committee scheduled for SequestOx. Essentially 100% conclusion now that none is required and the FDA will make their own decision. This usually means approval granted.
Remoxy will have its day in court.
See my previous post for drug liking curve.
http://investorshub.advfn.com/boards/read_msg.aspx?message_id=122581242
http://www.pharmiweb.com/PressReleases/pressrel.asp?ROW_ID=168113
Pain Therapeutics Announces FDA Advisory Committee Meeting for REMOXY®
Posted on: 19 May 16.
- August 5th is FDA’s Tentative Date for Advisory Committee Meeting -
- No Change to PDUFA Date -
AUSTIN, Texas, May 19, 2016 (GLOBE NEWSWIRE) -- Pain Therapeutics, Inc. (Nasdaq:PTIE) announced today that an Advisory Committee of the U.S. Food and Drug Administration (FDA) will review the REMOXY® New Drug Application (NDA), tentatively scheduled for Friday, August 5, 2016. This is intended to be a joint meeting of the FDA’s Anesthetic and Analgesic Drug Products Advisory Committee and Drug Safety and Risk Management Advisory Committee.
“This could be a prime opportunity to showcase the abuse-deterrence and other properties of our lead drug candidate, REMOXY,” said Remi Barbier, President & CEO of Pain Therapeutics. “We look forward to sharing our data with the FDA, Committee members and the general public.”
FDA also advised us that the Prescription Drug User Fee Act (PDUFA) date for the REMOXY NDA, September 25, 2016, is unchanged.
.
More: www.pharmiweb.com/PressReleases/pressrel.asp?ROW_ID=168113#ixzz497Rv4Qbu
So who are the new patients going to be for ELI200?
This is not true.
Overdose resistant opioid Rexista planning to file NDA this summer.
PRESCRIBER ALERT: Is This Your Oxycodone?
Did you prescribe this OxyIR? Are you sure?

SequestOx delivers the exact same pain relief as OxyIR, but it cannot be crushed, snorted, smoked, charred, or injected.
Update on drugs to prevent oral abuse and overdose.
Some day, when there are are a plethora of ADF opioids that prevent oral abuse and overdose, any company still using the 2 bead system (or any ADF that does not prevent oral abuse) will be at risk. For now, there is not even one drug that can prevent oral abuse and overdose, but I watch these efforts closely. I said all sorts of mean things about KemPharm KP201 last week, and I want to redeem myself now because KP201 is a pretty cool molecule that does something no other drug can do: “Reduced hydrocodone exposure at oral doses >= 8 tablets” and “Reduced incidence of hypoxia at oral doses >= 8 tablets.”
KP201 is a prodrug ADF. It requires the GI tract to convert inactive prodrug into active opioid agonist. In theory, this would not only prevent nasal and intravenous usage but also would offer some protection from oral overdose. That is a blockbuster idea, if it works. Unfortunately for KemPharm investors, it was only moderately successful at two of the three. It gums up and is not suitable for injection. The nasal pharmacokinetic graphs were posted by me last week (http://investorshub.advfn.com/boards/read_msg.aspx?message_id=122440578). It only modestly delays Tmax, decreases Cmax, and decreases AUC. Nasal Drug Liking data is scarce in the public domain, suggesting poor results, confirmed by AdComm 18-2 vote against ADF label. Even with questionable snorting studies, it might have been different for KemPharm if the oral overdose protection worked better. But it doesn’t kick in until 8 tabs have been swallowed! 7.5mg hydrocodone x 8 = 60mg IR hydrocodone. Quite a serious nap, add alcohol and benzos for the final cut. Any bigger size tabs there would be virtually no protection: 15mg tabs x 8 = 120mg hydrocodone IR would cause life-threatening respiratory depression in any opioid-naive patient. By far, Kempharm was furthest along in this in this effort to prevent oral overdose, and they just went back to the drawing board.
The other two publicly-known candidates to prevent oral abuse and overdose are Acura’s LIMITX and Intellipharmaceutics’ PODRAS technologies. They both have their own patents and both use a gastic-acid based system to prevent usage of multiple pills. Both have received Fast Track designation from FDA, and Acura LimitX was also awarded a $300,000 federal grant for phase 1 development back in 2014. Acura’s system requires them to develop separate “microparticles” for each opioid agonist, while IPCI says PODRAS will work for any abusable drug, not just opioids.
I really like Bob Jones at Acura. He reminds me of Jerry Treppel- gives a frank and forthright discussion, and sometimes more. He updated us on LimitX progress during their conference call this month:
In April we announced results of cohort one from study 400 which demonstrated that a three tablet dose of one of our test formulations LTX-04P lowered the relative maximum blood level of hydromorphone by approximately 22% compared to a non abuse deterrent version. This result exhibited the ability of LIMITX technology to retard the release of active ingredient when multiple tablets are ingested and makes it a viable abuse deterrent platform. The one and two tablet doses of LTX-04P did not deliver the active drug as we would expect for an immediate release dosage form which will require us to reformulate the microparticles in tablets that contain the active drug.
Research and development ("R&D") expenditures in the year ended November 30, 2015 were $7.2 million in comparison to $8.0 million in the year ended November 30, 2014.
…
The Company had cash of $1.8 million as at November 30, 2015 compared to $4.2 million as at November 30, 2014. As of February 25, 2016, we had a cash balance of $0.4 million.
Dear WeeZuhl,
Some of our regular readers send questions to WeeZuhl. By request, this is a repost of a recent response, with a follow-up discussion on drugs that prevent oral abuse and overdose.
Dear WeeZuhl,
I have a question that I have seen them arguing about on the Elite Facebook page. The question is: If Elite’s drugs are not crushed does it or does it not behave like any other opioid when taken as directed?
If a user takes more than directed without crushing it, will they not get high and possibly overdose?
Please explain this with a post to the board.
Thank you,
Afraid On Facebook

Agreed!!! LOL.
they better get busy it is May 14
HAL studies do not count. yes, they COULD do some more bunion trials
of course elite could get exclusivity, but only if it conducts clinical trials (other than bioequivalence) necessary for approval.
Exclusivity provides the holder of an approved new drug application limited protection from new competition in the marketplace for the innovation represented by its approved drug product.
another puny "generic" with no exclusivity
Amen to that! Say it again!
I like this part:
We share the same technology as Pfizer have for their pharmacological approach. We have our patents on our polymer, they have theirs on there.
Great question, doc
if ALO-02 is approved will it not have exclusivity?
Expect to file at least two more opioid products in 2016.
...the Company is not required to return any portion of this $5 million received from Epic, and the Company can, and has, used these funds to advance the Company’s business objectives.
...I’ve said this before, I have more than a dozen ideas for our stock that are ready to go into clinical trials and into the market. We don’t have to mind or to execute all of them. So we decide which are the cream of the crop, the top two, three, or four, and focus on these, keeping in mind how much they’re going to cost..
You do not sell a billion dollar technology for one product’s price.
Elite Pharmaceuticals Goals, Investor Presentation April 2016
http://ir.elitepharma.com/events_presentations
Lasers try this link:
http://ir.elitepharma.com/events_presentations
Please point out what is factually inaccurate below.

