 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.


Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
No dilution Outstanding Shares
483,714 as of 07/06/2021, almost 2 months since RS the company hasn’t diluted the shareholders
Yes, merger approved. And current imun bid 3.31 ask $4 and only 2 shares traded. Where's that twitter "expert" with 15,000 followers when you need him/her? You know, the one saying buy, buy, buy back at $20? Long gone I bet, along with all the money from anyone who acted on his/her advice about imun.
Big question now - how long will imun hold above $1?
imun ceo have anything to say to shareholders as they get wiped out? Or just hiding under a table somewhere with a business plan that says gradually sell off the new cyto shares to finance insiders' lifestyles for the next 5 years?
Really annoys me to see crap like this happen. And somehow it is legal.
So quiet without all the pumping about $160 share price. $16 would be a miracle.
Lack of confidence in IMUN management. Yeah, IMUN owns a nice chunk of an asset. If people had confidence that management was savvy and could turn that $15,000,000 asset into $30,000,000 the price would reflect that. Right now it looks like investors think management is going to turn their $15,000,000 into $2,500,000.
Dilution is always a concern, too.
Ok. Putting all the verbal back and forth bullshit aside, what do you think investors are missing? Using currently known numbers, imun should be worth about $30/share. Why do you think it trades around $5?
Assumptions:
Current market of new company: $200,000,000
Cyto owns more than 50% so use: $100,000,000
Imun owns 15% of cyto shares so? $15,000,000
Divided by 487,000 imun shares: $30/share
So what's the missing piece of the puzzle?
here the Cytocom/CBLI CC can be heard again
https://www.webcaster4.com/Webcast/Page/2462/41942
I find a lot of posts funny. I have read people saying Netlist, when it was at 0.20 cent last year, that the company will be dead and BK.. Now it´s trading above $5.00 and the same people still saying it´s a bad investment.
so just don´t care what others say. do what your gut tells you.
We know that IMUN owns 15% of Cytocom.. that´s all you need to know..;)
(I am not talking to you MSDR directly. I just used the word "you" generally :) gltall
Did they say exactly what the share structure was going to look like??
What was said… they crushing CBLI.
I didn’t think the call was that bad this morning???
So what have I been missing out on? Not buying cbli over $6? Not buying imun over $20?
the merger has been approved by the shareholders
https://www.streetinsider.com/dr/news.php?id=18647881
I'll see what happens tomorrow after the conference call.
Yes I bought some recently at $4.75 didn't buy any today. Unfortunately, I have enough at the moment. Certainly I'm not selling.
So yes, you're an imun buyer here?
You have been missing out on CBLI and will eventually miss IMUN.
Missing what? Price under $5 and 300 shares traded. Were you the one buying those 300 shares today?
Interesting blurb Combined companies “developing therapies and plans to launch therapies into the $48.7 billion gastrointestinal market, the $84.3 billion therapeutic oncology market, the $82.5 billion hematology market and the $125.0 billion autoimmune market.”
Yeah, volume in cbli just exploded.
Look at CBLI go. IMUN won't be far behind. You are missing it all SSC!
Cleveland BioLabs, Inc. (NASDAQ: CBLI), an innovative biopharmaceutical company developing novel approaches to activate the immune system, today announced that the Company and Cytocom Inc., a leading biopharmaceutical company developing next generation therapeutics that target immune restoration and homeostasis, will host an investor call and live webcast on Wednesday, July 7 at 8:30 a.m. ET.
https://mma.prnewswire.com/media/1440125/Cleveland_BioLabs.jpg
During the call, Michael K. Handley, President and Chief Executive Officer of Cytocom, and members of the Cleveland BioLabs Board of Directors will discuss the results of the vote on the merger transaction, scheduled to take place July 6, 2021, during a Special Meeting of Cleveland BioLabs shareholders. Mr. Handley will also discuss the strategic vision for the combined companies including the opportunities in COVID-19, Crohn's disease, pancreatic cancer, hematology, and acute radiation syndrome. The company is developing therapies and plans to launch therapies into the $48.7 billion gastrointestinal market, the $84.3 billion therapeutic oncology market, the $82.5 billion hematology market and the $125.0 billion autoimmune market. The combined company could have the broadest Toll-like receptor therapeutic platform in the industry, allowing it to potentially treat a multitude of immune-related diseases and significantly expand the size of its total addressable markets.
I thought imun was going to $160 lol? Why the need to do a reverse merger?
Acquisition or reverse merger but IMO reverse merger is more likely
Going forward… the most likely scenario is a reverse merger. Why else do the reverse split??
A special meeting of the Cleveland BioLabs stockholders related to the merger (with Cytocom) will be held virtually on July 6 at 10:00 a.m. E.T.
IMUN will finally receive its shares in the merged companies. This is huge for all three companies. CBLI should have a run-up on the merger today.
Penny stock Advaxis and Biosight Announce Entry into Reverse Merger Agreement
IMUN is perfect to do reverse merger with another private company
Okay, I'm not an expert here but I usually thing of Dilution as being the share count going up. Shares outstanding are currently 482K I think in the last 8 years or so that share count has barely moved. Or at least not much compared to other stocks on the pink sheets.
Would you please explain/elaborate what you are indicating as an IMUN 400,000 share range of dilution for as long as you remember. Thank you.
I don't have any of that. I pretty much wrote the shares off as worthless. I'm just happy they will have value and be trading again soon. I'm looking forward to conference call 7.6. Maybe we will get some answers.
It has been in the 400K share range for as long as I remember. If there was some dilution like 10 years ago fine.
Good luck to you. As an owner of cyto, it certainly would be enlightening if you could share their financial info, you know, things like a balance sheet, revenues and burn rate. Any helpful stuff like that to help give a better picture of what the merged shares might be worth.
What?? In the entire history of IMUN and going back to when it was previously named TNI Biotech, Inc (TNIB) there has NEVER been dilution?? Really!
IMUN has never had dilution before. I would almost encourage it if the money raised was going to be put to good use but I will watch as the story unfolds. I am in this stock because of LDN. I also own CBLI and CYTO. If the IMUN story starts heading in a direction I don't agree with I will move on but right now this is just a shell company with an investment in CYTO that I'm hopeful will do well with a current market cap of 2.4 million. Again, there has never been dilution.
So $5 is the bottom for imun, is that what you are saying?
Careful now, remember all those shares available for dilution because of the reverse split.
Maybe the worst RS I have ever seen. No reason to do it and the shareprice is down 70-80% since.
Great job IMUN management!
I'm talking about selling at $5, big mistake
Huge mistake? Like buying at 30 or 23, or predicting imun at 160 or 240? Now those were huge, documented, proven mistakes. Time will tell about current trading action.
Nah, its just investors making a huge mistake.
imun $4.50 down from $30. Looks like their ceo isn't disclosing the whole picture.
CBLI nice run today and 1 week from completion of the merger
Is dwarren still around, I’m interested to hear his take on everything that has happened?
Try to buy any large quantity of shares and you will see where the price is.
Try selling any large quantity of shares and you will see where the price is. But let's say ok, under $6, and down from $30 with predictions of $160. Does that sound better?
proof that the price is ABOVE 5.00

Price under $5, volume 2 shares. Looks like most people have figured it out.
No dilution has occurred
483,714 OS as of 06/23/2021
2.7M MCAP
Current CYTO equity stake $12M-15M
you are right imo
"IMUN is tremendously undervalued and is perfect target for reverse merger or acquire new assets."
Yes, even if the combined market cap of CYTO is 80 million and no new press releases with positive news after merger, IMUN is cheap right now IMO.
Yep… I picked up another 1,500 shares. Should be about 36M shares total after the merger. IMUN should get a little over 2.5M shares. This is pretty cheap right here.
I bought some at $4.75. My first purchase in almost 2 years. Loving it!
|
Followers
|
136
|
Posters
|
|
|
Posts (Today)
|
0
|
Posts (Total)
|
18220
|
|
Created
|
03/09/06
|
Type
|
Free
|
| Moderators | |||
IMUN - Immune Therapeutics
| Shareholders of Record | 808 | a/o Apr 16, 2019 |
|
| Authorized Shares | 750,000,000 | a/o May 4, 2020 | |
| Outstanding Shares | 457,577,799 | a/o May 4, 2020 |
Quick Links:
www.immunetherapeutics.com
www.cytocom.com (subsidiary of IMUN - Cytocom will get eventual U.S. sales - if that ever happens - hopefully in 2-3 years?? IMUN owns 16.95% of Cytocom as of June 30, 2018. LDN has already received various Phase 2 approvals in the United States, see www.cytocom.com/investors/)
www.fidson.com (partner in Nigeria for marketing and distribution)
http://www.acromaxdominicana.com/ (partner for manufacturing in Dominican Republic - contract in 8-k)
http://www.omaera.com/ (partner in Kenya for marketing and distribution)
www.aharpharma.com (partner in Nigeria)
Important Links:
HIV Eradication 7 minute video, Oyagen
Kevin Phelps, CFO of Oyagen
Kevin Phelps (already on board of IMUN) becomes Interim CEO of IMUN, Michael Handley focusing on role as CEO of Cytocom and Forte Biotechechnology
https://m.youtube.com/watch?v=iydWaAmHblM
Youtube Video on Covid19 and low dose naltrexone
IMUN and Cytocom will collaborate to develop therapies for COVID19
IMUN provides guidance on reverse stock split and name change (reverse stock split first announced in 2018)
ImQuest Biosciences
Patent
IMUN appoints Michael Sander to board
Michael Handley is new CEO and president of IMUN
IMUN adds Kevin Phelps to the Board of Directors
Research on Lodonal in A & U Magazine
10-q from Q3 2018: IMUN ships first 250k pills to Fidson Healthcare (pg 25)
Ambassador Jack Brewer joins IMUN's board of directors
IMUN labeled as Pioneer in article in Forbes magazine
Dr Gary Blick, renown HIV specialist, joins IMUN's scientific advisory board
IMUN adds former US Assistant Surgeon General, Dr Roscoe Moore, as the new Chairman of the Board
Video from AIDS 2018 conference - starts at 59:58
IMUN acquires 10% stake in Cytocom
Research on Lodonal for HIV featured in Plus Magazine
Link to HIV Plus Magazine article on Lodonal
IMUN announces publication of White Paper on Lodonal
8-k from 5/22/18: Fidson Healthcare accepts its appointment as the sole distributor of Lodonal in Nigeria
CNN Video interviewing Fidelis Ayebae, CEO of Fidson Healthcare
Form SC 13G from 5/15/18: Iliad Research and Trading owns 9.99% stake in Immune Therapeutics
8-k from 4/27/18: Kenya Pharmacy and Poison board files NDA for Lodonal for final review
IMUN received minutes from FDA Meeting for Lodonal for Crohn's Disease
First order shipped. First revenues for IMUN for $195k from AHAR Pharma
System for Award Management (companies need to register here to qualify for UNAIDS and other goverment grants) - Click on search records, then type in Immune Therapeutics.
8-k from 12/1/17: Shareholder letter - AHAR issues IMUN its first ever purchase order of $195,000
10-Q from 11/14/17: IMUN lists $214k in inventory. First time ever listing having inventory on a 10-q or 10-k in IMUN's history
8-k from 11/2/17 - Note with Iliad Research and Trading
8-k from 9/8/17: IMUN announces exclusive agreement with Omaera Pharmaceuticals for Lodonal in Kenya - valued at a minimum of $31m in revenue over 3 years - first purchase order contractually guaranteed by 11/22/17
Kenya Agriculture, Fish, and Food Authorities: Approved List of Suppliers, Human Drugs and Medicine - Omaera Pharmaceuticals is on the list
8-k from 8/25/17: IMUN hires new COO Rudy Williams and hires new CEO of Cytocom Dr. John H Abeles (Dr. John H Abeles will also be new senior executive advisor of IMUN)
10-Q from 8/14/17: IMUN records first GAIN ever in shareholder equity for a quarter, and achieves this on NO REVENUE (due to elimination of toxic debt)
8-k from 4/27/16: LDN is approved in Nigeria
"The NAFDAC approval follows the successful completion of a 90-day bridging study conducted by AHAR Pharma on behalf of the Company in conjunction with State Specialist Hospital in Asubiaro. That study, “ A Bridging Study to Evaluate the Effects of ‘Lodonal’ as an Immune-System regulating Agent in Subjects in which Their Immune System is Compromised: Lodonal in the Treatment of Subjects with Human Immuno-Deficiency virus (HIV), ” met the primary and secondary endpoints for both efficacy and safety.
Breakthrough Lodonal Results on HIV Patients:
The 90-Day Bridging Study was undertaken at the State Specialist Hospital in Asubiaro, Osogbo, Osun State, Nigeria and the primary objective of this Bridging trial was to confirm that Lodonal had a beneficial effect on the immune system of immune deficient patients and safety. This was a single center, open labeled, randomized, bridging study of a 150 people. The Treatment Group was treated with 4.5 mg of Lodonal nightly in conjunction with antiretroviral. The Control Group was treated with antiretroviral plus placebo . The primary endpoints were efficacy and safety determined by a minimum increase of 25% in the CD4 count with no adverse effects on quality of life.
The results yielded an average 44% increase in CD4 count in the Treatment Group compared with 11% increase for the Control Group and there was no adverse effect on quality of life or opportunistic infections during the trial. The Nigeria trial’s results were consistent with previous clinical trials of LDN.
Due to its favorable cost/benefit, the Company believes Lodonal has large market potential to be the first affordable non-toxic therapy of its kind. It is administered in a single oral dose daily making medical and drug compliance much easier and is designed to produce a significant reduction in opportunistic infections. In addition to affordably improving the quality of patients’ lives, it offers a compelling economic benefit to health care systems."
8-k from 5/23/17: LDN gets marketing approval in Nigeria
CNN interviews Fidson Healthcare CEO, Fidelis Ayebae
8-k from 11/2/16: Contract with IMUN's manufacturer in the Domincan Republic, Acromax Dominicana
8-k from 4/13/17: Debt restructuring to eliminate a very "toxic" note.
8-k from 3/14/17 - Debt restructuring with Florida Hedge fund
8-k/a from 3/17/17 - Debt restructuring with Florida Hedge fund - ammendment
8-k from 11/15/16 - Debt restructuring
8-k from 4/28/17: IMUN files NDA for LDN for HIV and Cancer in Kenya
PR from 5/31/17: IMUN signs MoU with Ivory Coast for LDN
PR from 10/26/16: IMUN files NDA for LDN for HIV, Cancer and as an Immune Booster with Senegal
PR from August 2015: Letter of Intent from Fidson Healthcare PLC - this publishing popped IMUN to just over $0.30 briefly
Stock Quote of Fidson Healthcare PLC - IMUN's supposed partner (LOI) for marketing / distribution in Nigeria - notice how the ticker has shot up since April
8-k from 4/13/16: IMUN Provides Drug Development Status on MENK (Methionine-Enkelphine) in China
8-k from 4/21/16: IMUN signs binding LOI to acquire Chinese CAR-T Technology and Clinical data
Nigeria Clinical Trials Registry - Lodonal - note that it still says "Pending". According to 8-k's, the drug is officially approved, so IMUN should be good on this
Low Dose Naltrexone Forum - Proboards
LDN Clinical Trials via ldninfo.org (has not been updated since 2013, but still a very nice list)
List of Clinical Trial Publications for LDN via clinicaltrials.gov
www.lowdosenaltrexone.org
11 Facts about HIV in Africa
http://www.ldnafricaaids.org/ (has not been updated since late 2012)
http://www.ldnafricaaids.org/wp-content/uploads/2011/08/Traore-et-al-1.pdf (clinical study on LDN in Mali)
https://www.usaid.gov/work-usaid/get-grant-or-contract/grant-and-contract-process
http://data.unaids.org/publications/irc-pub05/jc431-stratplan4_en.pdf
http://www.ldnafricaaids.org/?page_id=3 (the story of LDN and the late Dr. Bernard Bihari (passed away May 2010), the pioneer of low dose naltrexone - TNIB / IMUN acquired patents in late 2012/early 2013 - see 10-k)
The medicine your doctor never told you about (but should have)
Low-Dose Naltrexone (LDN): One of the RARE Drugs that Actually Helps Your Body to Heal Itself
My experience with Low Dose Naltrexone By David Gluck, MD (the story of a lifelong friend of Dr. Bernard Bihari, the pioneer of LDN)
We now have a NEW Senior Regulatory Advisor (see last page of powerpoint) who is (or was?) ALSO the Senior Regulatory Officer for the GATES FOUNDATION! - other than the powerpoint presentation from the LD Micro conference, there has not yet been any 8-k recognizing any of these new additions (Dr. John H Abeles, Rufus (Rudy) Williams, Vincent Ahonkhai).
Speeding Access to Low and Middle Income Countries: by Vincent Ahonkhai
PEPFAR - Department of Defense
http://naca.gov.ng/
http://www.nascop.or.ke/
http://pharmacyboardkenya.org/
http://www.croiconference.org/search/node/naltrexone
https://www.ldnscience.org/research
Videos to watch on Low Dose Naltrexone
https://www.youtube.com/watch?v=Kz52KK5IhOc&t=1s (4 mins, CBS News - Wonder drug Low Dose Naltrexone?...very uplifting encouraging video about a woman's story on LDN)
In this 4 min video above, it states that no Big Pharma companies are backing LDN. This is correct, because it is off-label: 50-mg Naltrexone was approved by the FDA in the 80's. Thus, making it cheap because 50-mg Naltrexone is generic (50mg Naltrexone didn't work well for what it was approved for - heroin addicts, therefore it ended up becoming generic). Low dose naltrexone, 4.5mg, however, is patented, and studies have shown its effectiveness (44% increase in CD4 count in Nigerian trials, when they were searching for a minimum of 25% increase in CD4 count). And it's safe - very little side effects except for possible lucid dreams. But still, it's "cheap". Noreen says it will costs patients in Nigeria $.84 per day, $0.24 of which will be profit. The low cost is the reason why big pharma did not WANT to fund this drug. Because there has always been little research done on LDN, big pharma was happy keeping it that way. They knew that if LDN did ever gain traction as the go-to therapy for any given disease, it would make big pharma lose billions of dollars, if in fact LDN can replace more expensive drugs that the big pharma companies are selling. This could potentially make IMUN a potential acquisition target by big pharma in the future.
https://www.youtube.com/watch?v=FDCn0JWv6Io (59 mins; very informative documentary telling the story of LDN)
https://www.youtube.com/watch?v=pg1T0bKxx9E [11 mins; a woman gives a detailed explanation of how LDN has helped her - 4 month update (not doing so well) and 1 year update (doing much better)]
https://www.youtube.com/watch?v=rll1A3aFhjc (79 mins; "[the late] Dr Bihari [the pioneer of low dose naltrexone] is Interviewed about Low Dose Naltrexone LDN for Normalizing Immune System Function")
https://www.youtube.com/watch?v=r4quvjDiXcY (60 mins; LDN & Cancer - The Game Changer)
https://www.youtube.com/watch?v=l8sWzoLtop4 (29 mins; LDN as a treatment for Autoimmune disease)
https://www.youtube.com/watch?v=Aaqa50lcoeA&t=133s (Dr. Jill Smith from Penn State talks about Low Dose Naltrexone for Crohn's disease)
Books on Low Dose Naltrexone (great reviews on Amazon)
https://www.amazon.com/Promise-Low-Dose-Naltrexone-Therapy/dp/0786437154/ref=sr_1_2?ie=UTF8&qid=1497648079&sr=8-2&keywords=low+dose+naltrexone
https://www.amazon.com/LDN-Book-Little-Known-Naltrexone-Revolutionize/dp/1603586644/ref=pd_bxgy_14_img_2?_encoding=UTF8&pd_rd_i=1603586644&pd_rd_r=GPZPCV3F5HAS56V1CT2F&pd_rd_w=NLw9g&pd_rd_wg=ExBQX&psc=1&refRID=GPZPCV3F5HAS56V1CT2F
https://www.amazon.com/Honest-Medicine-Time-Tested-Inexpensive-Life-Threatening/dp/0982969015/ref=sr_1_1?ie=UTF8&qid=1500958081&sr=8-1&keywords=honest+medicine
Upcoming Catalysts (expected)
- Contracts with Fidson Healthcare and other distributors in Nigeria and potentially other African nations.
- Approval from NACA, NASCOP.
- Revenues beginning with Fidson Healthcare (Nigeria) and other distributors.
- Revenues beginning with Omaera Pharmaceuticals (Kenya).
- Completion of Lodonal White paper.
- Lodonal expected to be included on UNAIDS essential medicines list.
- Approval in Ivory Coast.
- Grant approvals from UNAIDS and / or other goverment organizations such as USAID / Gates / PEPFAR (not exactly clear what is going on with this), but IMUN is indeed registered with sam.gov (System for Award Management), which is where a company must register to get goverment grants. They registered in January 2018.

Clinical Trials: Crohn’s Disease
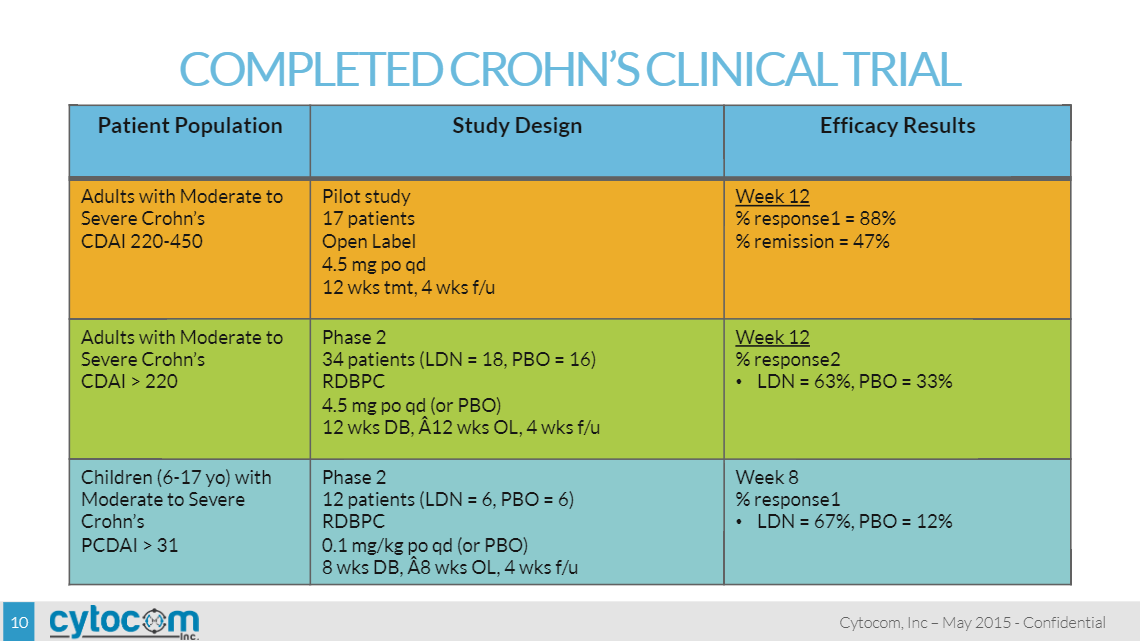
The first clinical trial results with LDN for immune disorders were published only recently in a peer-reviewed medical journal in 2007 which evaluated LDN treatment in a pilot Phase II study of 17 patients with moderate to severe, active Crohn’s disease. The open-label pilot study was conducted by Penn State University to evaluate LDN response, safety and toxicity. Patients were treated with LDN orally each evening at a dose of 4.5 mg for 3 months. A total of 17 patients were enrolled, 16 of whom completed the study. No laboratory abnormalities were noted. The most common side effect was sleep disturbances (occurred when dosing at night, at about bed-time), occurring in seven patients (41%). Two-thirds of patients in this study went into remission after 4.5 mg daily LDN treatment (p < 0.001), with 89% of patients overall showing some degree of response. Blood inflammatory markers were also analyzed, specifically c-reactive protein, or c-RP and erythrocyte sedimentation rate, or ESR. C-RP levels decreased from a median value of 2.6 (normal <0.8) at baseline to a value of 0.9 by the twelfth week of treatment, which was statistically significant (p = 0.03). The ESR decreased from a mean baseline value of 23.3 ± 0.4 mm/h to 17.9 ± 0.3 mm/h, which was also significant (p = 0.04). Baseline plasma enkephalin levels were 9.5 ± 2.8 pg/mL, and decreased to a value of 3.6±1.0 pg/mL at week 12 of LDN therapy.
A second clinical study was conducted by Penn State University as a randomized double-blind, placebo-controlled study to test the efficacy and safety of LDN for 12 weeks in adults with moderate to severe active Crohn’s disease. Forty subjects were enrolled in the study. Randomized patients received daily oral administration of LDN (4.5 mg/day) or placebo. Fatigue was the only side effect reported of statistical significance, and it was greater in subjects receiving placebo. Thirty percent of patients in this study went into remission (defined as a Crohn’s Disease Activity Index (“CDAI”) score ≤ 150), with 88% of patients overall showing some degree of response. Blood inflammatory markers, c-RP and ESR, were analyzed. Patients who exhibited a 70-point drop in CDAI scores with LDN had higher c-RP values at baseline (2.0 ± 0.5 mg/dl) compared to those subjects on LDN who did not exhibit a response (0.8 ± 0.3 mg/dl); however, this difference was not statistically significant (all values were included in the analysis including those subjects who flared during the study). Based upon this data, patients with high c-RP levels may be more likely to demonstrate a clinical response to treatment with LDN.
| 13 | P a g e |
A pilot Phase II clinical trial was conducted by Penn State University in children with moderate to severe active Crohn’s disease. Fourteen subjects were enrolled, 12 subjects were randomized and treated with a mean age of 12.3 years (range 8-17 years). Children were randomized to placebo or LDN (0.1 mg/kg or a maximum dose of 4.5 mg) orally for 8 weeks followed by open-label treatment for an additional 8 weeks of LDN at the same dose of 0.1 mg/kg or 4.5 mg. Results showed a significantly greater reduction of baseline pain in those taking LDN than in those taking placebo (28.8% reduction versus 18.0% reduction; p = 0.016). LDN was also associated with improved general satisfaction with life (p = 0.045) and with improved mood (p = 0.039), but not improved fatigue or sleep. Thirty-two percent of participants met the criteria for response (defined as a significant reduction in pain plus a significant reduction in either fatigue or sleep problems) during LDN therapy, as contrasted with an 11% response rate during placebo therapy p = 0.05). LDN was rated equally tolerable as placebo and no serious side effects were reported. Laboratory parameters for inflammation, specifically white blood count, c-RP and ESR all improved from baseline to Week eight; however, the results were not significant.
An open-label Phase II trial was conducted for Naltrexone as Therapy for Inflammatory Bowel Disease: Ulcerative Colitis and Crohn’s Disease Twelve patients received naltrexone 4.5 mg/day. Duration (mean ±SD) of naltrexone treatment was 46 ±75 weeks (maximum 270 weeks). One patient withdrew after 8 weeks owing to insomnia. Positive clinical responses were reported in 6/12 patients. Two clinical responders had colonoscopy before and after naltrexone and each had complete mucosal healing. (Leonard B. Weinstock, MD, FACG Journal of Clinical Gastroenterology: September 2014 - Volume 48 - Issue 8 - p 742)
Low Dose Naltrexone Reduces In Vitro Endoplasmic Reticulum Stress and Stimulates Wound Healing in Intestinal Epithelial Cells: A total, 40 patients (43% male, median age 40y, IQR 28–52 years) were treated with 5 mg NTX/day. Response was seen in 23 patients (13 CD; 10 UC), with a median duration of 2 months Conclusion
Low Dose Naltrexone may have a beneficial effect in the treatment of IBD by directly stimulating epithelial wound healing and reducing intestinal ER stress. G. Fuhler*, M. Lie, P. Dimitrijevic, C. J. van der Woude, M. Peppelenbosch Erasmus MC University Medical Centre Rotterdam, Gastroenterology and Hepatology, Rotterdam, Netherlands
Low Dose Naltrexone in the treatment of Crohn’s Disease open label 17 patients were treated with LDN for 12 weeks and showed a 70% reduction in CDAI score with endoscopy 88% in the LDN group and 28% in the control group endoscopic remission 33% in the LDN group 8% in the control group with no adverse events. 10 Dig Dis Sci 2011 Jul;56(7):2088-9 7Michael Arata, MD.
Low Dose Naltrexone in the Treatment of Crohn’s Disease: A Case Series 56 patients on 4.5mg IBS patients show clinical response to LDN (54%) and should be considered as an adjunct to conventional therapy in patients with resistant disease or as a bridge while another treatment plan is formulated. Further studies are required to evaluate the degree of mucosal healing while on LDN. University of Florida http://www.gastrojournal.org/article/S0016-5085(15)32952-8/abstract.
Clinical Trials: HIV/AIDS
A single blind 90 day with 4 week f/u randomized completed a 90-day bridging trial for the treatment of patients with HIV AIDS. The National Agency for Food and Drug Administration and Control (NAFDAC) approval is based on previous clinical data and the Nigeria Bridging Trial. The trial was a single center, open labeled, randomized, bridging study consisting of one hundred and fifty [150] patients of both genders between the ages of 18-60, each of whom was infected with the human immunodeficiency virus (HIV).
The 90-Day Bridging Trial was undertaken at the State Specialist Hospital in Asubiaro, Osogbo, Osun State, Nigeria with the primary objective to confirm Lodonal™ has a beneficial effect on the immune system of immune deficient patients and that it is safe. The trial separated the patients into a Control (placebo) Group and a Treatment Group (which was administered Lodonal™). The efficacy of increasing CD4 count [cell/mm3] between Day-1 and Day-90 by at least 25% was set as the criteria for demonstrating beneficial effect on the immune system. Safety was demonstrated through quality of life assessment and vitals both of which were not adversely affected. Treatment Group patients were given a daily dose of 4.5-mg/kg of Lodonal™.
| 14 | P a g e |
The results yielded an average increase of 44% increase in CD4 count in the Lodonal™ Treatment Group compared to an 11% increase in the Control Group. Additionally, there were no reported opportunistic infections and no toxicity levels uncovered. Liver function remained normal and there was no negative impact on other systems based on blood results. No significant sleep disturbance or vivid dreams were present enough to justify trial discontinuation. No significant adverse CNS, renal, cardiac, hepatic, musculoskeletal, hematopoietic side effects were present. NAFDAC issued drug and marketing approval of Lodonal™ in July of 2017 in the management of HIV/AID’s and immune dysfunction.
A single blind nine-month randomize clinical trial and a single prospective cohort study were conducted in Mali to evaluate the impact of LDN on asymptomatic HIV+ adults. Results of the nine-month study showed an improvement in cluster of differentiation 4 (“CD4”) count in the treatment groups that was significantly greater than the control group at 6 months (p = 0.041) and marginally at 9 months (p = 0.067). Results of the single prospective cohort study showed 71% of subjects that completed the study did not show any indication of clinical AIDS symptoms, side effects or a loss of CD4 count that would warrant initiation of antiretroviral therapy (“ART”) medication.
A 12-week, placebo-controlled trial of LDN was conducted from 1985-1986 in 38 patients with AIDS by Dr. Bihari and his colleagues. Patients who participated in this trial showed a significant difference in the incidence of opportunistic infections with 5 out of 16 patients (31%) on placebo developing opportunistic infections in comparison to 0 of the 22 patients in the LDN group. Other differences between placebo and LDN treated patients included: lymphocyte mitogen responses declined on placebo and not on LDN; pathologically elevated levels of acid-labile alpha interferon declined significantly in the patients on LDN and not in those patients on placebo.
After the conclusion of the above clinical trial, Dr. Bihari began to use LDN in his own medical practice. Of 158 patients in his practice that were evaluated, only ten (6%) were on antivirals. Patients of Dr. Bihari who had taken the drug regularly as prescribed showed no drop in CD4 cells. The average CD4 number in these patients before starting LDN was 358, and the average 18 months later increased to 368. There were 55 patients who had not taken the drug, or had taken it only sporadically (non-compliant). These patients showed a drop of CD4 cells from an average of 297 to 176 in 18 months. This represented a drop in CD4 of approximately 80 per year, which corresponds to the average drop observed in patients with HIV receiving no treatment. The stabilization of CD4 cells in patients who were administered LDN was also accompanied by disease stabilization. The 55 patients who were non-compliant experienced 25 opportunistic infections, in comparison to the 103 compliant patients who only experienced eight. Survival between the two groups was also significantly different, 13 deaths occurred in the 55 non-compliant patients compared to only one death in the compliant group of 103. At the time of this referenced article (Bihari et al., Sept 1996), patients in Dr. Bihari’s practice had been on LDN for seven to eight years, with no disease progression, no drop in CD4 levels and no evidence of resistance to the beneficial effects of LDN. None of the patients experienced side effects while on LDN.
Dr. Bihari also examined CD4 changes in 19 patients who were on the combination treatment regimen of 3TC (Epivir), azidothymidine (“AZT”), and LDN. The rise in CD4 counts at 6 months in Dr. Bihari’s patients was compared with the rise in CD4 counts reported by an investigator working for Glaxo Smith Kline. In both groups, none of the patients had taken AZT previously; however, Dr. Bihari’s patients simultaneously were treated with LDN, which the Glaxo Smith Kline group did not receive. The patients on LDN had an average baseline CD4 count of 88 while the Glaxo Smith Kline group had an average baseline value of 352. The Glaxo Smith Kline patients experienced an average rise in CD4 of 40 at six months; or an increase of 11.3%. The LDN patients experienced an average rise of 106 CD4’s at 6 months, representing a 128% increase. Of the 19 LDN patients, each patient experienced an increase of at least 30%. In 18 of the 19 LDN patients, a significant increase in energy, appetite and mood was observed. In those LDN patients who were severely underweight, weight gains of ten to 50 pounds were observed in the first two months of treatment.
| 15 | P a g e |
Clinical Trials: Fibromyalgia
LDN has been utilized in a number of trials to investigate its use for the treatment of fibromyalgia. Studies conducted to date in adult patients have typically used an LDN dose of 4.5 mg/day in comparison to placebo.
LDN was assessed for the treatment of fibromyalgia, in a single-blind, crossover trial in which ten women were enrolled. This study utilized the following treatment schedule: Baseline (2 weeks) →Placebo (2 weeks) → LDN 4.5 mg/day (8 weeks) →Washout (2 weeks) LDN reduced fibromyalgia symptoms in the entire cohort, with a greater than 30% reduction of symptoms over placebo. As observed in other studies with LDN, side effects were rare, minor and transient, and included sleep disturbances such as insomnia and vivid dreams.
In a second study, 31 women with fibromyalgia participated in a randomized, double-blind, placebo-controlled, counterbalanced, crossover study. During the active drug phase of the study, participants were administered oral LDN at a dose of 4.5 mg daily. This study showed a benefit with LDN in comparison to placebo for the treatment of fibromyalgia. A significantly greater reduction of baseline pain was observed in those taking LDN in comparison with those taking placebo (28.8% reduction versus 18.0% reduction). LDN was also associated with improved general satisfaction with life and with improved mood. Thirty-two percent (32%, n=9) of participants met the criteria for response (defined by the study as at least a 30% reduction in pain, plus a 30% reduction in fatigue or a 30% improvement in sleep) during LDN therapy, as contrasted with an 11% (n=3) response rate during placebo therapy. Both LDN and placebo were tolerated equally and no serious adverse events were reported.
Clinical Trials: MS
A PILOT TRIAL OF LOW-DOSE NALTREXONE IN PRIMARY PROGRESSIVE MULTIPLE SCLEROSIS was run at the University of Pennsylvania by Dr. Ian Zagon and Pat McLaughlin:
OBJECTIVE: To evaluate the efficacy of 4.5mg nightly naltrexone on the quality of life of multiple sclerosis (MS) patients.
METHOD: A sixth month phase II multicenter-pilot trial with a low dose of the opiate antagonist Naltrexone (LDN) has been carried out in 40 patients with primary progressive multiple sclerosis (PPMS). The primary end points were safety and tolerability. Secondary outcomes were efficacy on spasticity, pain, fatigue, depression, and quality of life. Clinical and biochemical evaluations were serially performed. Protein concentration of beta-endorphins (BE) and mRNA levels and allelic variants of the mu-opioid receptor gene (OPRM1) were analyzed.
RESULTS: Five dropouts and two major adverse events occurred. The remaining adverse events did not interfere with daily living. Neurological disability progressed in only one patient. A significant reduction of spasticity was measured at the end of the trial. BE concentration increased during the trial, but no association was found between OPRM1 variants and improvement of spasticity. The data indicates that LDN is safe and well tolerated in patients with PPMS.
PILOT TRIAL ON LOW-DOSE NALTREXONE AND QUALITY OF LIFE IN MULTIPLE SCLEROSIS:
OBJECTIVE: evaluate the efficacy of 4.5mg nightly naltrexone on the quality of life of multiple sclerosis (MS) patients.
METHODS: This single-center, double-masked, placebo-controlled, crossover study evaluated the efficacy of 8 weeks of treatment with 4.5mg nightly naltrexone (low-dose naltrexone, LDN) on self-reported quality of life of MS patients.
| 16 | P a g e |
RESULTS: Eighty subjects with clinically definite MS were enrolled, and 60 subjects completed the trial. Ten withdrew before completing the first trial period: 8 for personal reasons, 1 for a non-MS-related adverse event, and 1 for perceived benefit. Database management errors occurred in 4 other subjects, and quality of life surveys were incomplete in 6 subjects for unknown reasons. The high rate of subject dropout and data management errors substantially reduced the trial’s statistical power. LDN was well tolerated, and serious adverse events did not occur. LDN was associated with significant improvement on the following mental health quality of life measures: a 3.3-point improvement on the Mental Component Summary score of the Short Form-36 General Health Survey (p = 0.04), a 6-point improvement on the Mental Health Inventory (p < 0.01), a 1.6-point improvement on the Pain Effects Scale (p =. 04), and a 2.4-point improvement on the Perceived Deficits Questionnaire (p = 0.05). LDN significantly improved mental health quality of life indices. Further studies with LDN in MS are warranted.
A PILOT TRIAL OF LOW-DOSE NALTREXONE IN PRIMARY PROGRESSIVE MULTIPLE SCLEROSIS:
OBJECTIVE: To evaluate the efficacy of 4.5mg nightly naltrexone on the quality of life of multiple sclerosis (MS) patients some with relapsing-remitting MS and some with secondary progressive MS.
METHODS: This single-center, placebo-controlled, study evaluated the efficacy of 17 weeks of treatment with 4.5mg nightly naltrexone (low-dose naltrexone, LDN) on self-reported quality of life of MS patients.
RESULTS: The results on LDN’s effect on quality of life (as measured by physical and mental health) was not clearly proven, with no statistically significant differences shown between the LDN-dosed group and the placebo group many have argued the reason for the problem with this trial was the crossover design which have shown in the past not to provide good results when treating with LDN. Data indicates that LDN is safe and well tolerated in patients with PPMS.
RETROSPECTIVE CHART REVIEW OF MS PATIENTS RECEIVING LOW DOSE NALTREXONE (LDN) TO ASSESS SAFETY, TOLERABILITY, AND EFFECT ON FATIGUE:
OBJECTIVE: This study investigated the safety, tolerability, and benefits (fatigue, reduction) of LDN in patients with MS. It reviewed the number of patients who stopped taking LDN and if there were specific reasons for stopping the LDN. The frequency and variety of side effects that were specific to LDN use are reported.
METHODS: A retrospective review was performed on 435 charts of MS patients who were seen in the Penn State Hershey out- patient Multiple Sclerosis Clinic between 1/1/2005 and 5/31/2012. There were 215 MS patients having exposure to LDN during the time of this study. RESULTS: The study confirmed an improvement in quality of life with the use of LDN over a long period of time. In addition to the assessment we review Brain MRIs and Spinal Cord MRIs that were obtained as part of the clinical status of the patient and standard of care. There were essentially no MRIs obtained immediately before LDN was started as would have been ideal in a prospective study. The average number of days of the Brain MRI before treatment with LDN was started was 444 days with a maximum of 4751 days. The average number of days to the latest Brain MRI after LDN was started was 708 with a maximum of 1772 days of 215 patients on LDN 113 MRI scans showed stable, 14 showed improvement, 28 slightly worse. The Slightly Worse MRI series indicated that new but inactive lesion(s) were identified when compared to the pretreatment study MRI. On the quality of life surveys showed 83 patients said they had improved, 92 patients said they were stable and 9 worse. The remainder of the patients did not continue on LDN.
Despite the number of small studies conducted to date, as well as all of the antidotal evidence from patients and doctors that either take LDN for MS or prescribe LDN for MS, Cytocom believes that results are promising, which the Company feels could bode well in larger studies as existing treatments are not every effective.
| 17 | P a g e |
Our Clinical Trial Program for Lodonal™/LDN
The Company held a Type C meeting in January 2018 with the FDA to discuss clinical protocol design and to seek guidance for the clinical development program in the treatment of adult and pediatric patients with Crohn’s disease using a 505(b)(2) pathway to support an NDA. Use of the 505(b)(2) pathway will allow us to seek FDA approval of Lodonal TM without the need to conduct a full development program consisting of both safety and efficacy trials. This will help us to shorten our development pathway and time to NDA submission. We plan to rely on the two drugs using naltrexone that have been approved by the FDA. The first drug approved 50 mg product as the reference listed drug, published literature and historical data and all of the historical data from the 50mg trials and to leverage recent Contrave® approval for safety/PK support at 4mg, 6mg and 8mg with approval granted for Naltrexone at 16mg with Wellbutrin to support the Phase II/III clinical trials and the ultimate filing of the NDA as a 505(b)(2) submission to the FDA. To date, nonclinical pharmacology and toxicology data and clinical safety data has been established from these sources, in addition to multiple Phase I/II studies conducted under our INDs.
To support the NDA filing, we plan to conduct the following pivotal studies:
| ? | Phase IIb, dose-response study/ies in patients with specific autoimmune disease(s); that will rollover into our |
| ? | Phase III, randomized, double-blind study/ies based upon Phase IIB results. |
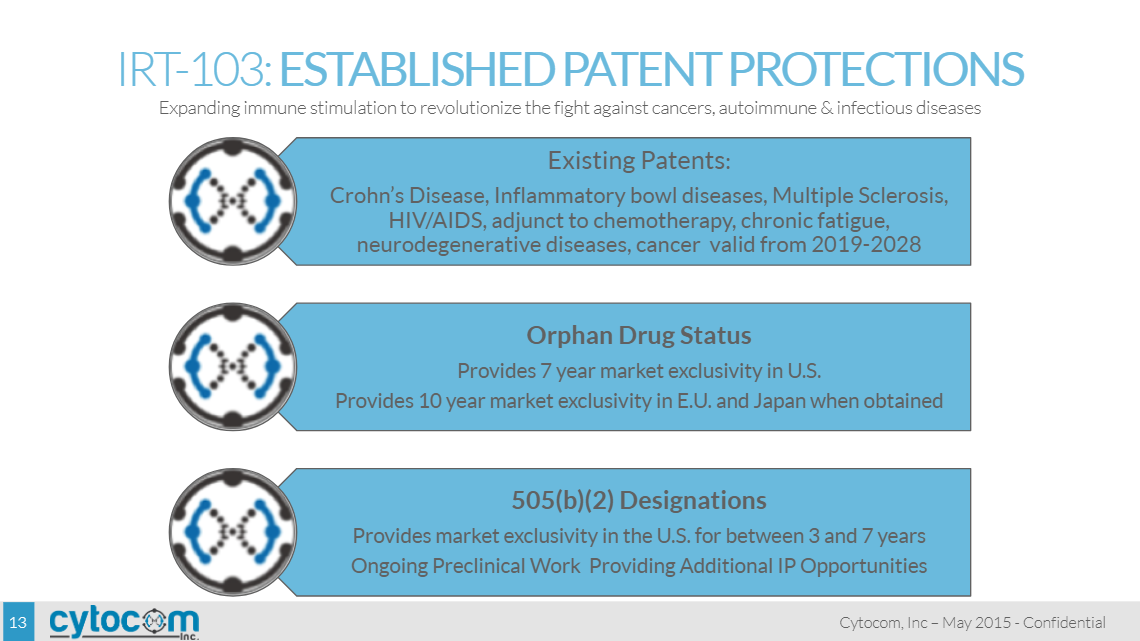
If NDA approval of Lodonal is granted, in addition to the patents the FDA grants three-year marketing exclusivity granted by law, we expect this product to be protected by patents that extend through at least 2023 for adults 7 year exclusive rights from date of approval for pediatric Crohn’s disease due to orphan indication. During which time it should not be subject to generic substitution. We plan to continue to support the Lodonal program with new patent applications as we obtain data from the clinical evaluation of our new formulation in healthy human subjects and in patients.
If the Phase 2B study of Lodonal is successful, we expect to quickly rollover into the Phase 3 confirmatory study to support product registration.
Based upon the indication chosen, the FDA has stated that a long-term (approximately 1 year) safety study of Lodonal™ will need to be conducted; however, all nonclinical studies to support the safety of the product and NDA submission are complete.
Developing LDN using the 505(b)(2) regulatory pathway lowers the hurdle for FDA approval. Because naltrexone is an FDA-approved product for alcohol or opiate dependence, the FDA’s 505(b)(2) pathway for approval is available and opens the door for us to gain FDA approval of LDN for new diseases. With the opportunity to use previous findings of safety, we intend to use the 505(b)(2) pathway to study and gain approval for our own product.
Patent and Subsidiary Acquisition (from the 10-k)
The Company entered into a share exchange agreement on April 24, 2012 to acquire all of the outstanding shares of TNI BioTech IP, Inc. (“TNI IP”), a biotechnology firm incorporated in Florida and formed to acquire patents related to the treatment of cancer and HIV/AIDS and autoimmune diseases, using Met-enkephalin (“MENK”) and Naltrexone (“LDN”). The goal of TNI IP’s management was to enable mankind and civilization to combat fatal diseases by activating and mobilizing the body’s own immune system using TNI IP’s patented use of MENK. The first patents acquired by TNI IP were acquired from Dr. Nicholas P. Plotnikoff and Professor Fengping Shan in 2012. TNI IP was acquired in exchange for 20,250,000 shares of the Company’s common stock, of which 8,000,000 shares were issued to Dr. Plotnikoff for the acquisition of patents and the remaining 12,250,000 shares were issued to the founders of TNI IP in exchange for all of their right, title and interest in their TNI IP shares. The goodwill arising on the acquisition of TNI BioTech IP, Inc. was valued at $98,000,000 and license agreements arising from the acquisition of TNI IP were valued at $16,006,000.
Intellectual Property
The Company has been developing active forms of immunotherapies through the acquisition of patents, IND Applications, clinical data and all proprietary technical information, know-how, procedures, protocols, methods, prototypes, designs, data and reports which are not readily available to others through public means, and which were owned, generated or developed through experiments or testing by Dr. Plotnikoff, Professor Shan, Dr. Bernard Bihari, Dr. Ian S. Zagon, Dr. Jill Smith, Dr. Patricia J. McLaughlin and Moshe Rogosnitzky.
The Company’s management believes that to be successful, it was imperative to not only acquire all of the intellectual property and patents but also the scientist(s) behind their development. To date, the Company has been able to acquire many of the patents and intellectual property it was seeking, and has also been able to team up with some of the leaders in the field of immunology, experts such as the late Dr. Ronald Herberman (1940-2013), Dr. Angus Dalgleish and Dr. Joseph Fortunak.
Dr. Plotnikoff is the inventor behind a number of patents granted for cancer treatments and an adjunct to patents for autoimmune diseases including: European Patent United Kingdom, Germany, France, Ireland EP 1401471 BI Methods for inducing sustained immune response; Russian Patent Russian Federation patent number 2313364; The Patent Office of the People’s Republic of China, Application No.: 200810165784.8 China Patent CN1015113407 A The Patent Office of the People’s Republic of China ISSN: 1006-2858 CN 21-1349/R; Patent Agencies Government of India Patent, Application number 1627/KOLNP/2003 number 220265 an Enkephalin Peptide Composition; and the US Patent Pending, US Patent Application 10/146.999 e (the “Plotnikoff Patents”). The Patent Cooperation Treaty (“PCT”) enables a U.S. applicant to file a single application, known as “an international application,” in a standardized format in English in the U.S. Receiving Office (the U.S. Patent and Trademark Office) that is acknowledged as a regular national or regional filing in any state or region that is party to the PCT.
The Company entered into a Sale of Technology Agreement with Dr. Nicholas P. Plotnikoff on March 4, 2012, wherein Dr. Plotnikoff agreed to transfer and assign all of his rights, title and interest in the Plotnikoff Patents to the Company. The Company received all the production formulations and technology designs from Dr. Plotnikoff necessary for the manufacturing, formulation, production and protocols of the MENK treatment of cancer and HIV/AIDS. As consideration for entering into the Sale of Technology Agreement, Dr. Plotnikoff received 8,000,000 shares of common stock, a royalty of a single-digit percentage on all sales of MENK and was granted the position of Non-Executive Chairman of the Board of Directors.
In addition to the above patents, we also signed an exclusive licensing agreement for all of the intellectual property developed at Pennsylvania State University by Dr. Ian S. Zagon, Dr. Patricia J. McLaughlin and Dr. Jill P. Smith for the treatment of cancer. The patents cover methods and formulations related to the treatment and prevention of cancers. More specifically, the present inventions describe the use of drugs that interact with opioid receptors (naltrexone, naloxone and the pentapeptide MENK) to inhibit and arrest the growth of cancer. Such efficacy has been discovered to be partially due to the functional manipulation of the zeta opioid receptor through exogenous and endogenous MENK. This receptor has been determined to be present in a variety of cancers, including pancreatic, ovarian, liver, head and neck, and colon cancer. US Patent Numbers 6,737,397, CA 2,557,504, US 20010046968 , US 6737397 , US 6136780 , US 20080015211 , US 20070053838 , US 8003630 ,US 20110123437 , US 7807368 , US 7576180 , US 7517649 , US 20080146512 , US 7122651 , US 20060073565 , US 20050191241 , Patent No 8,003,630.
We also acquired the licensing rights to the patent portfolio and intellectual property developed by Dr. Bernard Bihari relating to treatments with drugs that interact with opioid receptors such as LDN and MENK for a variety of diseases and conditions including malignant lymphoma, chronic lymphocyctic leukemia, Hodgkin’s lymphoma, and non-Hodgkin’s lymphoma, chronic herpes virus infections, and chronic infections due to the Epstein-Barr virus and a treatment method for humans infected with HTLV-III (AIDS) virus including patients clinically diagnosed as suffering from HIV/AIDS and those suffering from ARC. The licensed rights include all reissues or modifications, reexaminations, or other related U.S. patent filings directed to the same subject matter and the use of U.S. Patent Number 6,586,443 , U.S. Patent Number 6,384,044 , U.S. Patent Number 6,288,074 , U.S. Patent Number 5,356,900 , U.S. Patent Number 5,013,739 , U.S. Patent Number 4,888,346 .
Once the Company acquired the above patents, it was then able to sign a licensing agreement to acquire the exclusive patent rights for the intellectual property of the licensors, Dr. Jill Smith and LDN Research Group, LLC, whose members include Dr. Ian S. Zagon, Dr. Patricia J. McLaughlin and Moshe Rogosnitzky. The patents cover methods and formulations for the treatment of the inflammatory and ulcerative diseases of the bowel, using naltrexone in low doses as an opioid antagonist. Endogenous opioids and opioid antagonists at low doses have been shown to play a role in stimulating and rebalancing the immune system and the healing and repair of tissues. US Patent No. 6,136,780, Patent No. US 7879870. The Company then negotiated with Dr. Jill Smith to arrange the transfer of the Orphan Drug Designation for the use of naltrexone for the treatment of pediatric Crohn’s disease with the FDA. Dr. Smith has since transferred the IND to the Company, and the FDA acknowledged that the Company is now the sponsor for this IND. In September 2014, the Company and the licensors jointly agreed to terminate the license agreement, and in place thereof, have the licensors grant a similar license in their patent rights to Cytocom Inc. pursuant to a Patent License Agreement between the licensors, Cytocom Inc. and the Company with substantially similar terms as set forth in the original license agreement. Pursuant to this agreement, the Company issued 1,000,000 shares of its common stock to the licensors and the Company guaranteed the obligations of Cytocom Inc. to the licensors under the agreement.
The Company originally acquired the patents and intellectual property from Dr. Smith and LDN Research Group, LLC because management believed clinical trials involving LDN held great promise for the millions of people worldwide with autoimmune diseases or disorders, central nervous system disorders or those who face cancer. Management also believed it could be the first low-cost, easy to administer therapy with minimal to no side-effects for the treatment of HIV/AIDS, autoimmune diseases and immune disorders, in particular Crohn’s disease, multiple sclerosis, and/or fibromyalgia.
Dr. Nicholas Plotnikoff, Professor Fenping Shan and Noreen Griffin recently filed a Provisional Application for a Utility Patent US Application No. 62/296,759 Method for Inducing a Sustained Immune Response, which was assigned to the Company in March 2016. U.S. Patent and Trademark Office has issued the Official Filing Receipt in connection with this application, and accorded a filing date of February 18, 2016 during its pendency in the USPTO.
...The Company is working with the agencies to obtain local approval for the therapies for each modality that we intend to market for. We believe this will reduce our risk due to The Agreement on Trade Related Aspects of Intellectual Property Rights (“TRIPS”) which is an international agreement administered by the World Trade Organization (“WTO”). TRIPS allows emerging nations to manufacture drugs around existing patents.
https://en.wikipedia.org/wiki/TRIPS_Agreement
Quote from Wikipedia article:
The most visible conflict has been over AIDS drugs in Africa. Despite the role that patents have played in maintaining higher drug costs for public health programs across Africa, this controversy has not led to a revision of TRIPS. Instead, an interpretive statement, the Doha Declaration, was issued in November 2001, which indicated that TRIPS should not prevent states from dealing with public health crises. After Doha, PhRMA, the United States and to a lesser extent other developed nations began working to minimize the effect of the declaration.[8]
A 2003 agreement loosened the domestic market requirement, and allows developing countries to export to other countries where there is a national health problem as long as drugs exported are not part of a commercial or industrial policy.[9] Drugs exported under such a regime may be packaged or colored differently in order to prevent them from prejudicing markets in the developed world.
In 2003, the Bush administration also changed its position, concluding that generic treatments might in fact be a component of an effective strategy to combat HIV. Bush created the PEPFAR program, which received $15 billion from 2003–2007, and was reauthorized in 2008 for $48 billion over the next five years. Despite wavering on the issue of [compulsory licensing], PEPFAR began to distribute generic drugs in 2004-5.
From 3/15/17 publishing...
"Immune Therapeutics CEO Applauds President Trump’s Initiatives for Pharmaceutical Reform
The Company noted that the characteristics of Lodonal, namely its affordability and ability to receive regulatory approval in countries like Kenya, Nigeria and Senegal can provide, the type of solutions that President Trump would like to see implemented by pharmaceutical companies around the globe.
“I applaud President Trump and the measures he is taking to ensure the cost of drugs decrease first by increasing competition and second hopefully reducing the time it takes for a potential drug to hit the market. Immune Therapeutic’s goal since its inception has always been to provide affordable non-toxic therapies and we are proud to have been one of the first biotech companies at the forefront of this movement. We believe our strategy of providing affordable non-toxic sustainable health care therapies for autoimmune diseases as well as HIV and cancer, could propel Immune Therapeutics as an innovative, disruptive, player in the pharmaceutical industry. It is finally time for a change and we are looking forward to supporting President Trump’s and Congress’s initiatives in this arena,” concluded Ms. Griffin."
Recent News from PEPFAR (that should hopefully be related to IMUN, but there is no indication of that in the article)
https://www.pepfar.gov/press/ias2017/index.htm
















| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |



