 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.





Replies to post #87412 on Avid Bioservices Inc (CDMO)
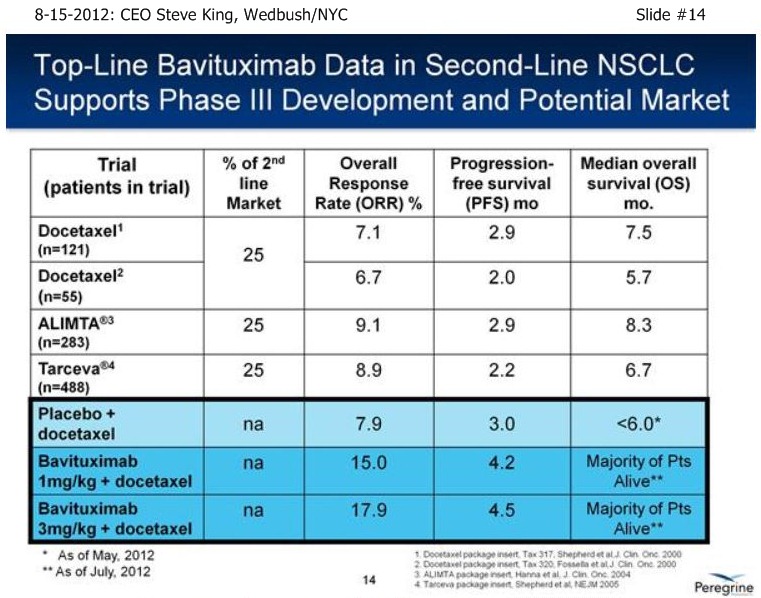
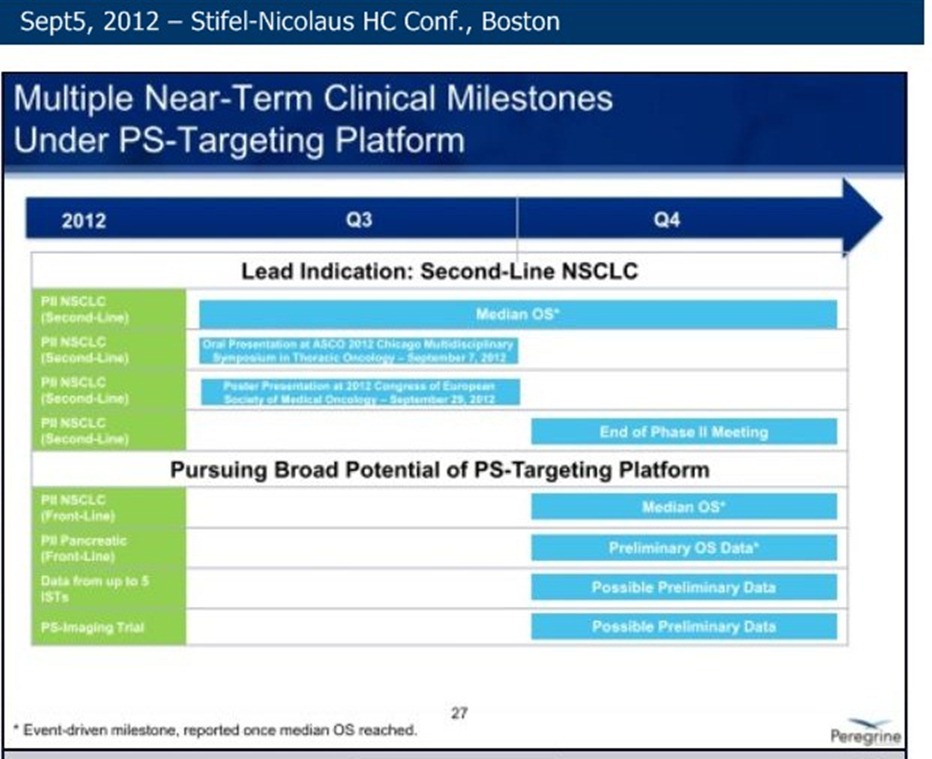
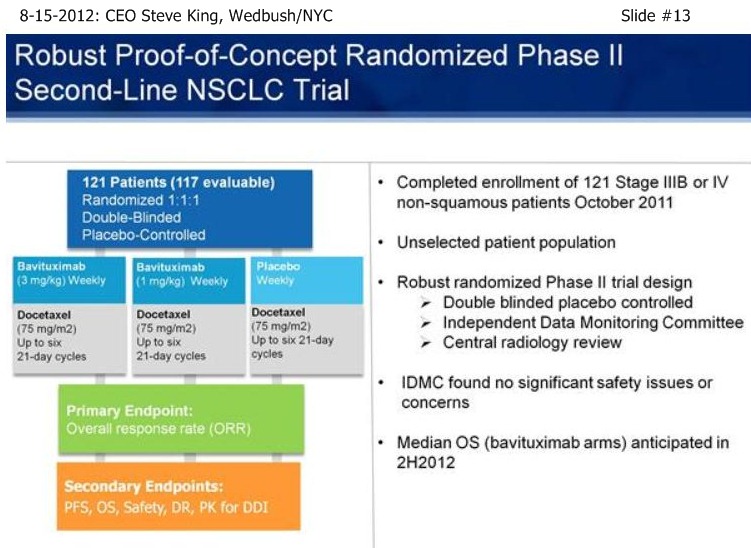
As we’re sitting here today, we have still not reached the # of events for MOS in either of the Bavituximab arms – and, in fact, we still have patients that are on treatments.







| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |

