Stephanie -- it was interesting that the NYT took comments on that article -- they do that now (never used to of course, only took comments to op-eds and blog entries), but still only occasionally
One day .. one day .. it's amazing to read that even asthma is taken as a preexisting illness for denial of insurance at an affordable price, so many including me would have been stuffed since early childhood .. and 22% increase in a year in a premium!
Everyone here says if traveling don't get sick in the USA, they all have heard stories
Hospital emergency rooms, particularly those serving the urban poor, are closing at an alarming rate even as emergency visits are rising, according to a report published on Tuesday.
Urban and suburban areas have lost a quarter of their hospital emergency departments over the last 20 years [ http://jama.ama-assn.org/content/305/19/1978.short ], according to the study, in The Journal of the American Medical Association. In 1990, there were 2,446 hospitals with emergency departments in nonrural areas. That number dropped to 1,779 in 2009, even as the total number of emergency room visits nationwide increased by roughly 35 percent.
Emergency departments were most likely to have closed if they served large numbers of the poor, were at commercially operated hospitals, were in hospitals with skimpy profit margins or operated in highly competitive markets, the researchers found.
Although the study did not examine emergency care at the remaining facilities, the closings take a toll on the quality of care in all emergency rooms, said Dr. Renee Y. Hsia, an assistant professor of emergency medicine at the University of California, San Francisco, and the lead author of the study.
“Some people think, ‘As long as my emergency room isn’t closing, I feel O.K. and protected,’ ” said Dr. Hsia, whose research was financed by the Robert Wood Johnson Foundation. “But even if they don’t lose the E.R. in their own neighborhood, they do experience the effect of fewer emergency rooms — the waits get longer and longer, and people’s outcomes get worse.”
New York City lost three hospital emergency rooms in 2008, two in 2009 and two more last year, when St. Vincent’s Hospital Manhattan in Greenwich Village closed, followed by North General Hospital in Harlem. St. Vincent’s had handled more than 60,000 emergency visits a year, while North General’s E.R. had recorded 36,000 annual visits.
A 24-hour emergency care and ambulatory surgery center [ http://www.nytimes.com/2011/03/11/nyregion/11vincents.html ], operated by North Shore-Long Island Jewish Health System, is planned for Greenwich Village. Neighborhood advocates have expressed concern that the free-standing emergency room will not be able to deliver adequate care without the backing of a full-service acute-care hospital.
The new study warns of delays in emergency care that are already playing out in the community, said Dr. David L. Kaufman, a member of the Coalition for a New Village Hospital who worked at St. Vincent’s for more than 30 years. Patients who would have sought care at St. Vincent’s, he said, “take longer to get to nearby hospitals in New York City traffic. They’re waiting many, many hours to be seen and managed, and if they require admission, they have to wait another 12 to 24 hours because there are no beds.”
The aim of the analysis was to figure out what characteristics make a hospital emergency department likely to close, Dr. Hsia said. Rural hospitals were excluded because some are designated “critical access hospitals” and operate under federal mandate.
Emergency rooms at commercially operated hospitals and those with low profit margins were almost twice as likely as other hospitals to close, Dr. Hsia and her colleagues found. So-called safety-net hospitals that serve disproportionate numbers of Medicaid patients and hospitals serving a large share of the poor were 40 percent more likely to close.
In addition, hospital emergency rooms in the most competitive markets were 30 percent more likely than others to close.
“This suggests market forces play a larger role in the distribution and availability of care” in the United States, Dr. Hsia said, especially emergency care. “We can’t expect the market to allocate critical resources like these in an equitable way.”
Conditions in emergency rooms may be worsened by the new health care law, several experts said. The law will expand eligibility for Medicaid, the government health plan for the poor. Often beneficiaries turn to emergency rooms for care, because many physicians do not accept Medicaid payments, said Dr. Sandra M. Schneider, president of the American College of Emergency Physicians.
Emergency rooms are required by law to provide treatment regardless of ability to pay. “People will have coverage, but there’s a concern that there will be nowhere for them to go,” Dr. Schneider said.
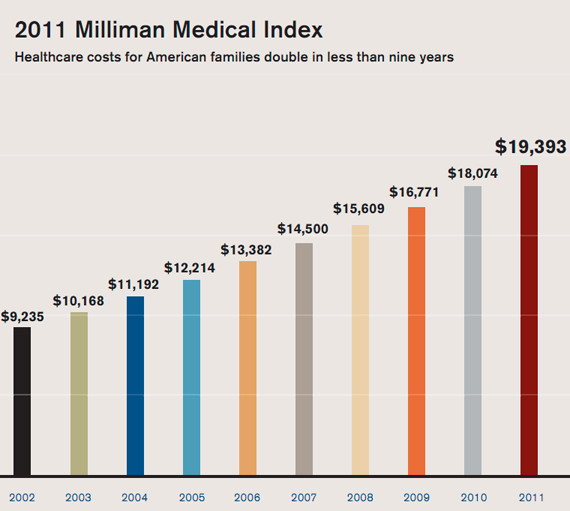
That might be only 7.3 percent higher than last year's average cost of $18.074, which is the smallest year-over-year increase in almost a decade. But it's also the highest year-over-year increase in total dollars spent per family at $1,319.
Trends over the last decade more completely illustrate the toll taken on the average American by rising healthcare costs.
"In 2002, American families had healthcare costs of $9,235, and those costs have now doubled in fewer than nine years," said Lorraine Mayne, Milliman principal and consulting actuary, in a press release. "As costs continue to grow -- and even as the cost trend decelerates -- the total cost of care for American families constitutes a larger and larger portion of the household budget."
Of that $1,319 increase, employers were paid for 48.6 percent of the increase, while the additional 51.6 percent was the responsibility of employees.
That's only slightly different from trends of the last five years. Over that period, employers have absorbed $3,023 in additional healthcare costs, employees themselves absorbing only slightly less, at $2,988.
Take away costs paid by employers, and the employee's share of costs has still doubled. In 2010, the average employee paid $8,008 for his family's healthcare, up from $3,634 in 2002.
Gordon Smith of the Maine Medical Association, testifying, says he's "less comfortable" with Republican positions on health care. Craig Dilger for The New York Times
By GARDINER HARRIS Published: May 30, 2011
AUGUSTA, Me. — With Republicans in complete control of Maine’s state government for the first time since 1962, State Senator Lois A. Snowe-Mello offered a bill in February to limit doctors’ liability [(items linked in) http://investorshub.advfn.com/boards/read_msg.aspx?message_id=39738694 and preceding and following] that she was sure the powerful doctors’ lobby would cheer. Instead, it asked her to shelve the measure.
“It was like a slap in the face,” said Ms. Snowe-Mello, who describes herself as a conservative Republican. “The doctors in this state are increasingly going left.”
Doctors were once overwhelmingly male and usually owned their own practices. They generally favored lower taxes and regularly fought lawyers to restrict patient lawsuits. Ronald Reagan came to national political prominence in part by railing against “socialized medicine” on doctors’ behalf.
But doctors are changing. They are abandoning their own practices and taking salaried jobs in hospitals, particularly in the North, but increasingly in the South as well. Half of all younger doctors are women, and that share is likely to grow.
There are no national surveys that track doctors’ political leanings, but as more doctors move from business owner to shift worker, their historic alliance with the Republican Party is weakening from Maine as well as South Dakota, Arizona and Oregon, according to doctors’ advocates in those and other states.
That change could have a profound effect on the nation’s health care debate. Indeed, after opposing almost every major health overhaul proposal for nearly a century, the American Medical Association supported President Obama’s legislation last year because the new law would provide health insurance to the vast majority of the nation’s uninsured, improve competition and choice in insurance, and promote prevention and wellness, the group said.
Because so many doctors are no longer in business for themselves, many of the issues that were once priorities for doctors’ groups, like insurance reimbursement, have been displaced by public health and safety concerns, including mandatory seat belt use and chemicals in baby products.
Even the issue of liability, while still important to the A.M.A. and many of its state affiliates, is losing some of its unifying power because malpractice insurance is generally provided when doctors join hospital staffs.
“It was a comfortable fit 30 years ago representing physicians and being an active Republican,” said Gordon H. Smith, executive vice president of the Maine Medical Association. “The fit is considerably less comfortable today.”
Mr. Smith, 59, should know. The child of a prominent Republican family, he canvassed for Barry Goldwater in 1964, led the state’s Youth for Nixon and College Republicans chapters, served on the Republican National Committee and proudly called himself a Reagan Republican — one reason he got the job in 1979 representing the state’s doctors’ group.
But doctors in Maine have abandoned the ownership of practices en masse, and their politics and points of view have shifted dramatically. The Maine doctors’ group once opposed health insurance mandates because they increase costs to employers, but it now supports them, despite Republican opposition, because they help patients.
Three years ago, Mr. Smith found himself leading an effort to preserve a beverage tax — a position anathema to his old allies at the Maine State Chamber of Commerce and the Republican Party but supported by doctors because it paid for a health program. The doctors lost by a wide margin, and the tax was overturned.
Mr. Smith still goes to the State Capitol wearing gray suits, black wingtips and a gold name badge, but he increasingly finds himself among allies far more casually dressed, including the liberal Maine People’s Alliance [ http://www.mainepeoplesalliance.org/ ] and labor groups. And while he still greets old Republican friends — he is a lobbyist, after all — he spends much of his time strategizing with Democrats.
Representative Sharon Anglin Treat, a powerful Democrat who was first elected in 1990, said that she and Mr. Smith were once bitter foes. “But Gordon’s become like a consumer activist,” she said with a big smile. “I’ve seen him more times in the last few years than I can count.”
Dr. Nancy Cummings, a 51-year-old orthopedic surgeon in Farmington, is the kind of doctor who has changed Mr. Smith’s life. She trained at Harvard, but after her first son was born she began rethinking 18-hour workdays. “My husband used to drive my son to the hospital so that I could nurse him,” she said. “I decided that I really wanted to be a good surgeon, but also wanted to raise healthy, well-adjusted kids I would actually see.”
So she went to work for a hospital, sees health care as a universal right and believes profit-making businesses should have no role in either insuring people or providing their care. She said she was involved with the Maine Medical Association, for the most part, to increase patients’ access to care.
Dr. Lee Thibodeau, 59, a neurosurgeon from Portland, still calls himself a conservative but says he has changed, too. He used to pay nearly $85,000 a year for malpractice insurance and was among the most politically active doctors in the state on the issue of liability. Then, in 2006, he sold his practice, took a job with a local health care system, stopped paying the insurance premiums and ended his advocacy on the issue.
“It’s not my priority anymore,” Dr. Thibodeau said. “I think Gordon and I are now fighting for all of the same things, and that’s to optimize the patient experience.”
Many of Mr. Smith’s counterparts in other states told similar stories of change.
“When I came here, it was an old boys’ club of conservative Republicans,” said Joanne K. Bryson, the executive director of the Oregon Medical Association since 2004.
Now her group lobbies for public health issues that it long ignored, like insurance coverage for people with disabilities.
Even in Texas, where three-quarters of doctors said last year that they opposed the new health law, doctors who did not have their own practices were twice as likely as those who owned a practice to support the overhaul, as were female doctors.
Dr. Cecil B. Wilson, the president of the A.M.A., said that changes in doctors’ practice-ownership status do not necessarily lead to changes in their politics. And some leaders of state medical associations predicted that the changes would be fleeting.
Dr. Kevin S. Flanigan, a former president of the Maine Medical Association, described himself as “very conservative” and said he was fighting to bring the group “back to where I think it belongs.” Dr. Flanigan was recently forced to close his own practice, and he now works for a company with hundreds of urgent-care centers. He said that in his experience, conservatives prefer owning their own businesses.
“People who are conservative by nature are not going to go into the profession,” he said, “because medicine is not about running your own shop anymore.”
 News
News  Market Data
Market Data  Discover
Discover