







Tuesday, September 11, 2012 2:29:50 PM
9-10-12 Qtly CC Transcript (Q1FY’13 q/e 7-31-12)
((( Orig. transcript from SeekingAlpha.com [ http://tinyurl.com/8prvsbn ], with numerous corrections made. )))
Link to webcast replay: http://ir.peregrineinc.com/eventdetail.cfm?eventid=118444
NOTE: 9-10-12 Financials Press Release is included at the end of this post.
C.C. EXCERPTS:
…STEVE KING (CEO): “The exclamation point for these milestones came just last Friday [9-7-12] with a report that patients receiving Bavi+chemo in our proof-of-concept study in 2nd-Line NSCLC had doubled the MOS compared to patients receiving chemotherapy+placebo. These are truly remarkable results that are not only great for the program, providing a clear signal to proceed toward a Phase III clinical trial, providing proof-of-concept that bavituximab is an active drug when given with docetaxel, but also great news for the NSCLC patients in the trial…”
…ROB GARNICK (HEAD/REGULATORY): “As you have just heard from Joe, the data we announced last week [9-7-12/Gerber/Chicago] has far exceeded our expectations, and I hope that you're as excited as I am with bavituximab's potential. I feel strongly that Peregrine should be recognized for having the corporate courage to conduct the rigorous, randomized placebo-controlled Phase II trial that provided these robust data and that provide the basis for us to plan for a pivotal Phase III program. We took an extraordinary amount of care in developing this Phase II trial design and conferred with clinical experts & regulatory agencies, including the FDA, in the design of this rigorous clinical trial. Peregrine chose to conduct this trial to definitively establish the proof of concept to bavituximab and now plans to potentially include this data as part of a registrational package. Having personally been involved in the evaluation of over 30 Phase II trials over my career, none of which ever achieved statistical significance, including many of today's blockbuster biotech products, I am personally extremely pleased with the quality of this data and the clarity with respect to advancing bavituximab in Phase III trials which it provides. Our next steps are to present the data you saw last week to global regulatory authorities as part of the formal End of Phase II [EOP2] meetings from which we anticipate gaining concurrence into the planning & execution of a pivotal trial program. Normally, it takes approx. 60 days to arrange such EOP2 meetings, and following these meetings to submit IND amendments for the Phase III and initiate the trial by mid-2013. . .Q&A: “I think the regulators will be very excited [about the 2nd-Line NSCLC data]. Certainly, the FDA had a lot of input into our trial design, and I think they gave us some a very wise counsel and I think this is exactly the kind of study that they would like to see. And certainly it provides for us the clarity, which you rarely have in Phase II trials, to decide to go clearly into a Phase III study and to actually really focus on replicating what we've just done. And I think that de-risks the program enormously, and really gives us a lot of confidence in how to go forward...”
FULL TRANSCRIPT…
9-10-2012 Q1 FY’13 Earnings Conf. Call (q/e 4-30-12)
WELCOME & FWD-LOOKING STATEMENTS: Jay Carlson (IR) http://www.peregrineinc.com
Speakers: Steve King, Joe Shan, Robert Garnick, Paul Lytle; Q&A session at end.
CEO Steve King – OPENING COMMENTS:
Since the beginning of last quarter, it has been an exceptional time for Peregrine, as we have seen 2 of the most important milestones in the company history achieved, transitioning the company toward late-stage drug development. The exclamation point for these milestones came just last Friday [9-7-12] with a report that patients receiving bavituximab + chemotherapy in our proof-of-concept study in 2nd-Line NSCLC had doubled the Median Overall Survival (MOS) compared to patients receiving chemotherapy + placebo. These are truly remarkable results that are not only great for the program, providing a clear signal to proceed toward a Phase III clinical trial, providing proof-of-concept that bavituximab is an active drug when given with docetaxel, but also great news for the NSCLC patients in the trial. While moving toward this important data, we also strengthened our balance sheet with a $30 million debt financing at favorable terms and continued to see good performance at our mfg. subsidiary, Avid Bioservices, successfully navigating regulatory inspections and posting another solid quarter of revenues. We are continuing to deliver on the milestones laid out earlier in the year and have more important events coming throughout the rest of this year, including our continuing bavituximab partnering discussions and due diligence, which remains a highly active area, preparing for an End of Phase II meeting for the bavituximab program and waiting additional clinical results from 8 ongoing clinical trials that will help further shape the program. With that, I will now turn the call over to Joe for a recap of the exciting clinical data that was presented last week.
JOE SHAN (VP/Clin.&Reg. Affairs) – CLINICAL TRIALS:
I'd like to start by reviewing important details of the clinical data from our Phase II 2nd-Line bavituximab NSCLC trial that was just presented last Friday [9-7-12 http://tinyurl.com/8oxwk6v ] in the Plenary session of the 2012 Chicago Multidisciplinary Symposium In Thoracic Oncology. I also encourage everyone to listen to the prerecorded webcast that can be found on our website for a more detailed discussion of the data presentation.
So trial file for our lead indication is a randomized, double-blinded placebo-controlled Phase II trial evaluating docetaxel with or without bavituximab as 2nd-Line treatment in patients with Stage IIIb or IV non-squamous NSCLC [ http://clinicaltrials.gov/ct2/show/NCT01138163 ]. On study, all patients received std. 2nd-Line chemotherapy of up 6 to 21 day cycles of docetaxel at 75ml/m2. In addition, patients were randomly assigned to receive a blinded weekly infusion of placebo, which we refer to as the controlled group, or 1 of 2 bavituximab doses studied, either 1 or 3 mg/kg until progression or toxicity. The primary endpoint of this trial is Overall Response Rate (ORR) and secondary endpoints include PFS, Overall Survival (OS), and safety. Between Oct.2010 and Oct.2011, 121 patients were enrolled at 40 global trial centers. No single center enrolled a substantial number of patients and approx. 50% of the patients enrolled were enrolled in U.S. centers with the remainder enrolled in Europe & India. All patients were previously treated with 1 prior platinum containing doublet regimen. Patient & disease characteristics were well-balanced across the 3 study groups with no differences in age, gender, race, ECOG or performance status, stage of disease, or prior treatments which could have significantly impacted the study results. Bavituximab continues to demonstrate a favorable safety profile with the combination of docetaxel + bavituximab being well tolerated, with no increase in frequency or nature of adverse events compared to the control arm. Notably, no increase in bleeding or clotting adverse events were reported with the addition of bavituximab, unlike the experience with other compounds which target blood vessels.
In terms of efficacy outcomes, let me start with a primary endpoint, ORR, which was determined by indep. central radiology reviews, according to RECIST criteria or Response Evaluation Criteria In Solid Tumors. As reported in May’12 when the study was initially unblinded, the ORR in the docetaxel+placebo arm was 8% compared to 15% in the bavituximab 1mg/kg arm; and 18% in the bavituximab 3mg/kg arm; and 16.5% in the pooled bavituximab arm. Though the response rate of the bavituximab-containing arms was double that of the control group, this trend favoring bavituximab did not reach the statistical significance, with P-values in the 0.2 to 0.3 range. This was expected as this trial has power to detect an 8% vs. 26% response rate, which is more than a 3-fold difference at a significance level of 0.15, not 0.05. This is expected also in a Phase II setting, as the main purpose of a trial of this size is to determine whether a drug candidate is promising enough to move into a larger Phase III trial with more statistical power.
Next, PFS also favored both bavituximab-containing arms with P-values approaching significance levels. Again, based on indep. central radiology review, median PFS and the docetaxel+placebo arm was 3.0 mos. In the docetaxel+bavituximab 1mg/kg arm, median PFS was 4.2 mos., corresponding to a Hazard Ratio (HR) of 0.57 with a P-value 0.08. In the docetaxel+bavituximab 3mg/kg arm, median PFS was 4.5 mos., corresponding to a HR of 0.65 with a P-value 0.19. In the docetaxel+pooled bavituximab arms, median PFS was 4.2 mos. with a HR of 0.6 and a P-value of 0.07.
Now, turning to Overall Survival (OS), another secondary endpoint in the trial, but the preferred efficacy endpoint, which represents direct clinical benefit. At the time of this analysis, over 70% of patients in the control group had died, while less than 50% had died in either bavituximab arm, and survival follow-up is continuing. The Kaplan–Meier [K-M] graph illustrates a clear and persistent separation of the survival curves favoring both bavituximab arms, demonstrating that OS is clinically and statistically significantly prolonged in the bavituximab arms. Specifically, in the docetaxel+placebo arm, the MOS estimate is 5.6 mos., while in the docetaxel+bavituximab 1mg/kg, the MOS estimate is 11.1 mos., with a HR of 0.51 and a significant P-value of 0.029. In the docetaxel+bavituximab 3mg/kg arm, the MOS estimate is 13.1 mos., with a HR of 0.54 and a P-value of 0.071. In the pooled bavituximab arm, the MOS estimate is 12.1 mos. with a HR 0.52 and a significant P-value of 0.015.
We have performed extensive subgroup analyses on these data and in both the 1mg & 3mg bavituximab arms subgroup analysis by age, gender, race, performance status and histologic subgroups showed a positive trend toward improved survival with bavituximab. Also, the survival results were comparable between patients from the U.S., Europe and India, suggesting treatment benefit does not appear to be limited to a subset of particular patients or where they were enrolled. Based on the positive outcome in OS, we're in the process of collecting available data of subsequent treatment at progression and so far, there does not appear to be any differences across the groups.
It is important, at this point, to reiterate that was a randomized, blinded placebo-controlled trial, in which no one knew what the patients were receiving in addition to docetaxel, and the treatment & procedure schedules were identical in all 3 arms. We could not have conducted a less-biased trial. The fact that the groups were well-balanced coming into the study, and both bavituximab arms showed similar benefit compared to the control arm, and that these significant interim survival results were not limited to a subset of patients, strongly support that bavituximab is an active agent which should be advanced into Phase III development. As you can imagine, we are very pleased with these interim results and look forward to announcing final results when available. Meanwhile, we are working towards the previously stated goals of meeting with the FDA before the end of this year in order to initiate a confirmatory Phase III trial by the middle of next year. I would now like to turn the call over to Rob for a regulatory update.
Dr. Robert Garnick (Head of Regulatory Affairs)
As you have just heard from Joe, the data we announced last week [9-7-12/Gerber/Chicago] has far exceeded our expectations, and I hope that you're as excited as I am with bavituximab's potential. I feel strongly that Peregrine should be recognized for having the corporate courage to conduct the rigorous, randomized placebo-controlled Phase II trial that provided these robust data and that provide the basis for us to plan for a pivotal Phase III program. We took an extraordinary amount of care in developing this Phase II trial design and conferred with clinical experts & regulatory agencies, including the FDA, in the design of this rigorous clinical trial. Peregrine chose to conduct this trial to definitively establish the proof of concept to bavituximab and now plans to potentially include this data as part of a registrational package. Having personally been involved in the evaluation of over 30 Phase II trials over my career, none of which ever achieved statistical significance, including many of today's blockbuster biotech products, I am personally extremely pleased with the quality of this data and the clarity with respect to advancing bavituximab in Phase III trials which it provides. Our next steps are to present the data you saw last week to global regulatory authorities as part of the formal End of Phase II [EOP2] meetings from which we anticipate gaining concurrence into the planning & execution of a pivotal trial program. Normally, it takes approx. 60 days to arrange such EOP2 meetings, and following these meetings to submit IND amendments for the Phase III and initiate the trial by mid-2013.
Touching on Cotara for a moment, Peregrine and the FDA are continuing to have positive discussions about the design & execution of a pivotal trial in GBM. We appreciate your patience as we just strive to gain the most advantageous strategy for both parties for this novel and potentially important drug candidate.
CFO Paul Lytle:
I'd like to spend the next few moments covering a few financial highlights and our related financial goals. As I mentioned on the last call, it's important to understand that we operate a hybrid business model that includes a revenue-generating contract mfg., business and an advancing drug dev. business.
Let me first focus on our contract mfg. business. During the last quarter, Avid generated $4.1 million in contract mfg. revenue, and we reiterate our revenue guidance of least $15mm for FY 2013. In addition to the non-diluted revenue we received from Avid, on the last earnings call [7-16-12 http://tinyurl.com/cs7spbz ], we mentioned that our next immediate focus was to secure a less dilutive debt financing vehicle similar to a term loan, in the range of $20-30mm. We recently executed on our stated milestone and closed on a $30 million term loan with 3 extremely well-respected institutions: Oxford Finance, MidCap Financial and Silicon Valley Bank. Under the loan facility, we received initial funding of $15mm on 8-30-12, and we have an option to receive an addl. $15mm in funding. This 2nd tranche becomes available to us upon the attainment of certain predetermined milestones, one of which was just achieved last Friday [9-7-12] with the announcement of the positive OS data from our 2nd-Line lung cancer trial. The 2nd related milestone pertains to having a positive EOP2 meeting with the FDA, defined as our ability to move into the Phase III trial design, and we plan to have that end of Phase II meeting with the FDA before the end of this year.
Another potential source of capital we are focused on pertains to our unencumbered pipeline. As you can imagine, given the bavituximab results that we shared with you on Friday, our partnering activities are continuing at a very active pace as we move closer towards the end of Phase II meeting with the FDA. Our stated goal is to have a partner on board before we start the Phase III trial and, preferably, before the EOP2 meeting with the FDA, as we would like our future partner to be a part of that important meeting. These are very exciting times for Peregrine and we have been diligent in executing against our stated milestones. We look forward to keeping you updated on our progress, and we will now open the call up to your questions.
Q&A: [21:15 mark]
1. Joe Pantginis – Roth Capital Partners: [ http://www.roth.com & https://roth2.bluematrix.com/docs/pdf/BLUE.pdf ]
JP: First, I just wanted to confirm something that I heard on Friday when Dr. Gerber presented the data. Can you confirm, did they say that the IDMC was the group that recommended pooling the data?
Joe Shan: Yes, that's true. So, typical on these sort of blinded studies, you have an IDMC who can independently look at some of the results in advance of being unblinded, and a central analysis plan is typical where you want to look at each group compared to the control separately. But because those 2 dose levels performed so similarly from each other, but better than the control group, it was recommended that we do a pro [indiscernible] exploratory pooled analysis.
JP: Thanks for providing the geographical breakdown update (earlier) - that was really helpful. If you could maybe further breakdown a couple of nuances here. Have you or will you be looking at any of the potential mutation statuses of the patients in this study? And also, have you looked at the outcomes of the patients that was a range from 15-20% of patients that received prior Avastin?
Joe Shan: Geographically, I think we mentioned that there were really no differences, and the reason why we couldn't get into all the details is there was a limited amount of time for Dr. David Gerber. As far as mutation status, that was not a requirement to enter the study, and recall, PS is a broadly-expressed target across multiple tumor types, so we did not collect that information on genetic mutations. In terms of outcomes, we did look at, for example, the % of patients who received prior Avastin as part of their frontline therapy, and there were no differences in outcomes with respect to that. There really were no other large enough groups to subset out.
JP: Two more quick questions. Obviously, you just alluded to part of the moa for bavi. For this study or any of the current ISTs, and even the planned Phase III, what particular immune parameters will you be looking at, such as, say, infiltration of cytotoxic T-lymphocytes or any other parameters?
Steve King: We're trying to build in some of that analysis, particularly into our ISTs. They're a little bit cumbersome to build into large studies, especially large blinded studies, as we might be running in the future. But, you’re on the right track, the immune status of the particular immune cells that are inside the tumors through tumor biopsies. We're also building in tumor blood flow measurements - that's particularly in one of our other NSCLC studies. When you think about the moa and how it relates to preclinical studies, we're trying to really build in those same sort of analysis into some more clinical studies.
JP: Lastly, Rob, you mentioned the fact that with your broad experience with multiple Phase II studies, highlighting the fact that Phase II studies are, obviously, not powered for statistical significance, and now you see these data here today; how do you think these data will affect the tenor based on your multiple interactions with the FDA in the past with your upcoming EOP2 meeting?
Robert Garnick: I think the regulators will be very excited. Certainly, the FDA had a lot of input into our trial design, and I think they gave us some a very wise counsel and I think this is exactly the kind of study that they would like to see. And certainly it provides for us the clarity, which you rarely have in Phase II trials, to decide to go clearly into a Phase III study and to actually really focus on replicating what we've just done. And I think that de-risks the program enormously, and really gives us a lot of confidence in how to go forward.
2. Charles Duncan (JMP Securities): [8-30-11 coverage init: http://tinyurl.com/3crdwqz ]
CD: I'm wondering about the control arm experience. There’s been lots bantering about in terms of the MOS, it does seem like it's within the range. But do you think that 5.6 month number is low, and is it driven by the % of patients that are really Stage IV vs. IIIb? What’s your perspective on that?
Steve King: With regard to the Stage of patients, I think in all the arms, it was around 90% Stage IV, so I don't think it's in any way related to that. If you look historically at the experience of docetaxel, that we are within the range at that 5.6 months, maybe on the low end of the range, but it's certainly consistent with some of the prior clinical trial results. In effect, if you look at some of the interim data that's been presented from some of the other trials involving docetaxel, it's very consistent with those results as well. And I think it's important that, while there's talk about well, it’s on the low-end, keep in mind that this is the reason the gold std. type of study to run is a double-blinded placebo-controlled study, because this is a patient population that is consistent with the entry criteria for all the arms; it's meant to be a solid control for this particular study. Otherwise, you could compare with historical results for docetaxel and say that, "Well, we beat the previous record for docetaxel and so it must be a good result." But really, this is the gold std. study – it’s meant to remove all the bias, make sure you have a similar patient population receiving the same dosing regimen with the same criteria and the same SOC. With that said, I think it's a clear result. I think it's actually remarkable that it's readout as a statistically significant result in OS. But again, it's what the FDA would expect, and as we think about what's the next trial going to look like, the Phase III, well, obviously, it's going to look very, very similar to this trial. In fact, with as few deviations from this trial design as possible because that is what will give us the highest probability of success.
Joe Shan: Steve, you already sort of hit the nail on the head. I mean, this is the reason why randomized clinical trials are conducted; you really shouldn't compare across studies. You do that early on when you have limited experience just as a benchmarking exercise, but you have to run randomized clinical trials and interpret the data in that context of that study, that subgroup. And we've already said that this is a smallish trial, it's not statistically-powered to show major significance. But, we did see that, and when we looked at the subgroups and the balance of patients coming into the study, it was well-balanced. So, there really isn't anything else we can say in trying to compare the number we saw on the docetaxel arm to other published studies. If you run enough studies and you can do some sort of meta-analysis, it certainly would fit in on the control results.
CD: I absolutely agree & appreciate the rigor of the design, and clearly, compelling and at least in my mind, clinical proof-of-concept. I'm wondering what you would do if anything different as as you go into Phase III. I know you haven't had your EOP2 meetings yet with the agency, but can you share with us, in terms of powering, how much would you discount these results in terms of the magnitude of benefit that you would look for in Phase III, and what would you do different if anything in terms of geography or the entry criteria that Steve mentioned with regard to defining these patients and what they have?
Joe Shan: As we stated, we feel the results from this Phase II are so clear & compelling that we want to change as little as possible going to a Phase III and really replicate hopefully these results. And, recognizing that usually Phase II data look better than Phase III, and so it's a little chip on the egg. We are not going to be overly ambitious in the statistical assumptions going into Phase III. We've stated before that we'd like to keep the Phase III study in the 300 to 500 patient range, and, working backwards, you can imagine it's going to be a Hazard Ratio of less than 0.8, but not as low as 0.5, so somewhere in between there. And, of course, significance of at least 0.05, with probably 8% or 9% power. These are very standard assumptions for Phase III, and I think we have the Phase II data to really support that type of assumption.
Robert Garnick: Just a quick follow-on to what Joe said, I think the std. for approval for a drug in 2nd-Line NSCLC will be another trial that would replicate this one, and as Steve said, as closely as possible. I'm not sure what else we would do different other than increase the “N” of the patients. And once we have that data, the combination of information between this trial and the next one, the pivotal Phase III - the plan would be that, that would be the data that we'll need to achieve an approval. I think if we achieve anywhere near the degree of clarity that we just obtained, I think this will be a pretty straightforward approval process. I'm sure the FDA would agree with me; the FDA as well as other global regulatory authorities would agree, that this is a pretty straightforward design and we really just need to obtain concurrence on it and then to begin our execution by mid-2013.
Joe Shan: Charles, I forgot to address your comment about the geography in the Phase III. I think clearly, we want as many of the patients in the Phase III to be enrolled in where we would like to eventually market the product, so obviously, U.S. & Europe. We recognize that the skepticism of clinical trial results coming out of emerging clinical trial regions such as India or Eastern Europe. However, I think we demonstrated in the study that there were really no differences. But, of course, we're going to keep a close eye on actual enrollment and perhaps, to sort of cap the enrollment, if any particular country is enrolling a lot faster than others.
Steve King: The thing about partnering discussions, and one of the reasons we feel it will be a big benefit to have a potential partner on board in time for the EOP2 meeting is, it really gives you an opportunity to think through the strategy because again, we are viewing this as a global registration trial and certainly the U.S., Europe and potentially, other territories will be involved naturally. But, it's the benefit of being able to ask all the questions that you want to ask in that EOP2 meeting and to think through things like where you want to enroll the patients, as Joe mentioned. Because ideally, you want the majority of those patients to come from the territories in which you are actually seeking approval, and that's, obviously, a big benefit. So, it's one of the reasons we're really trying to move along the partnering discussions and at the same sort of tempo as we are in the EOP2 meeting preparations.
CD: Can you provide any additional color in terms of partnering strategy? Would you ideally seek an indication-specific partner? Or do you think that this could prove to be a broader platform accessing-type partnership that might result in development of the drug across different indications?
Steve King: We view this is as an oncology partnering exercise. So clearly, there is bavituximab, in which we have the clinical data and the program worked generally as it relates to treating cancer. Essentially, our strategy hasn't really changed - it's ideally an ex-U.S. partnership. I think it will be all indications within oncology. It's just too difficult to try to split up different oncology indications. But certainly, geography is a way to split up the partnering exercise. We think at the least, having some sort of a co-promote at the end of the day, so we still have a considerable upside left for Peregrine as we continue to advance this program toward, hopefully, eventual product approval. So, I'm still primarily focused on ex-U.S. partnering, but with the realization that we're going to achieve our broader goal of also bringing in the capital that allows the company to be financially secure through the end of Phase III readout, we think is an important part of that partnering discussion. So like I said, probably ex-U.S. partnering, with some sort of a co-promote in the U.S., is a reasonable outcome, and there's been quite a number of good comparables out there for deals recently.
3. George Zavoico (MLV): [ 2-8-10 coverage init: http://tinyurl.com/yech7gz ]
GZ: Let me add to the congratulations of the results of the Phase IIB trial; it is really quite extraordinary. My question relates to the platform technology that bavituximab represents. The moa actually suggests that it could be effective in many other cancers. But, Peregrine had to choose to do the trials in those that were most likely to succeed based on prior data. And now you're pursuing some of these other leads with ISTs. These [2nd-Line NSCLC] results obviously provide considerable confidence, certainly in the lung cancer. But, could you speak to how it affects your plans for other indications? Are you, in the partnering discussions for example, are you looking for companies that might expand on the indication, or just want to do the Phase III trial? So could you speak to that, please?
Steve King: I think that clearly our goal is to bring on a partner with the partnership to them, move the program not just into a Phase III study, but a Phase III study with addl. clinical trials that will help explore the broader potential of the technology platform. Because you're right, from our preclinical modeling, and what we believe will extrapolate to the clinic, we believe most solid tumors, if not all solid tumors, will be PS-positive, and that chemotherapy again, across many different types of chemotherapy, will up-regulate that target. The other aspect of running as broad a program as we can and, as you alluded to, we have currently 8 ongoing studies to look at many different combinations & indications. More than likely, we're going to find combinations that work better than others, and those are kind of the ones we want to really follow-on. So, as you can imagine, as we're thinking about future clinical trials, additional trials combining docetaxel are attractive because we had the earlier Phase IIa results with docetaxel in which we had the very nice OS data in the breast-cancer patients. The data from this study [2nd-Line NSCLC] is, obviously, extremely positive, we couldn't be happier with that. But, we think that there will be other combinations and indications that are particularly hot areas for development. And, the other counterpoint of that is the fact that we'll probably find some combinations that just don't look as attractive, and that’s part of the purpose of running the clinical trials we’re running, is to really guide the program into those areas we're going to have the best benefits. So, we're going to continue to cast a wide net, find all those indications & combinations that are particularly attractive and then, really take advantage of those. I think it's a very similar approach to what it's been used for other highly successful drugs - Avastin is one that comes to mind, and Rob might be able to add a little color to that. But, the bottomline is, we're really trying to follow a strategy we think is the best shot at having multiple indications for this drug at the end of the day.
Robert Garnick: Following on to what Steve said, one of the things that's always attracted me to bavituximab is the fact that it does have such a potential plethora of possible indications. And as you pointed out, we really went into NSCLC based on the signal-seeking data that we had originally gotten in early Phase I & II studies. I think that was a very wise way to go forward. Just like Avastin, as you'll remember, Avastin was first developed in colorectal cancer and then, having a broad anti-angiogenesis moa, we then were able to develop that drug into multiple other cancers where, theoretically, its moa would still apply. And of course, Avastin has gone on to become an extremely profitable and valuable drug in the oncology arena. So, we're thinking about a very, very similar strategy for bavituximab - basically, using these ISTs to guide you in terms of where you're most likely to succeed and in what combination of drugs to combine with bavituximab. I think, luckily, we're seeing very good safety signals with the drug, and that's really an important aspect that helps us to decide how broad the drug action can be applied. So using the ISTs and then potentially other signal-seeking Phase IIs, we plan to really maximize the benefit of this particular product. And I think we've got a broad potential and a bright future.
GZ: As a follow-on to that, one of the things you guys pointed out a little bit earlier was, that this was broadly Stage IIIb, IV and non-squamous NSCLC - you didn't really need to have any mutational status prerequisites here, and which also suggests sort of a broader implication for this drug. And maybe you can speak to that as well, but not only that, it also suggests that it might also be active in the frontline setting - you had equivocal results earlier this year. But the hard data coming out of the frontline is OS, which I guess we expect later this year. So, how does that change your view, and does this give you added confidence that perhaps the frontline data will also turn out to be more positive than first reported this year?
Steve King: Obviously, as we're thinking about the moa, the immunomodulatory activity of bavituximab, its ability to turn on the immune system that, clearly, that's something that could, at the end of the day, show the biggest benefit in OS as patients who are on treatment long enough were able to elicit a strong immune response, which then helps hold the disease in check for an extended period of time. Certainly, that factor fits right in with the 2nd-Line NSCLC data, where we're having the biggest impact on OS. And again, it's not unexpected with immunotherapies and it's been seen with other immunotherapies that are in the clinic or earlier reported results. So, I think that's something we could see across-the-board. I think every clinical trial is an individual study in order to look at a particular combination in a particular stage of disease. Some are going to work and undoubtedly, if we run enough studies, some are not going to have positive results. We're anxious, like everybody else is, to see the data from the frontline study. In addition to the carboplatin & paclitaxel combination randomized study, we're also be exploring, pemetrexed in a frontline setting, and so we do believe that frontline NSCLC should be a target and still has a good probability of success for the company. It's just a matter of now, again, studying it in these individual studies and taking the hot lead into a pivotal trial at the end of the day. And we'll take the same approach with other solid tumor indications also, where often the shortest route to the market is in the high unmet medical need, which is typically in a 2nd+ line of therapy as we've done in NSCLC, and we want to continue explore that in other indications as well.
Joe Shan: George, you're right, we did not select based on that [mutational status]. However, I think bavituximab, in theory, could work though even with some of these ultra-targeted molecular drugs. It's just that was not the purpose of this particular study. In the future that's something I think we'll be interested in studying, those combinations as well. As far as differences across different studies, even in our own, Steve already mentioned that every study is a different experiment and they share some similar traits & trial design. But, at the end of the day, you just have to see what the data says. In our frontline study, I think the, surrogate readouts of response rates and PFS weren’t very clear in terms of any difference, but those are surrogates and not direct clinical benefit. So, we are hopeful that we might see something in OS – we’ve not yet reached that point. But, I think that's certainly a possibility and at this point, it’s just [indiscernible].
GZ: On your Imaging Program, I124-PGN650, you're enrolling patients in this trial, could this be also a part of the pivotal Phase III? Do you think you could track tumor response in the Phase III with I124-PGN650?
Steve King: Given the current timetable of the EOP2 meeting and beginning the study, it's just probably not in the cards for the Phase III. Certainly, I think as we think about future development, and I think this is something that also partners like very much, is it [I124-PGN650 Imaging] could be a very valuable tool as we go forward in selecting the right combinations and the right stage of disease, and being able to have, almost like a biomarker, that would allow us to guide the development of the bavituximab program, rather than having to run hundreds of randomized Phase II studies to pick the hot leads. We may be able to get an early read on that through the imaging program and the utilization of that in our bavituximab program in the future. But, as far as being ready for the Phase III, unfortunately, the time line is too tight and that ship is already kind of sailing along.
Joe Shan: And quite frankly, with the survival results we're seeing in "unselected population", there really is not a need to select patients in order to enrich results in the future. That's often a strategy that's not necessary if across-the-board you're not seeing a lot of activity, but maybe in a particular subset, for example, some mutational status - that sort of makes sense. But I think bavituximab is broad enough that's not a requirement. But we are developing an imaging platform, as Steve said, as potentially a tool for selecting different combinations or such.
4. Gregory R. Wade (Wedbush: [ http://www.wedbush.com/services/cmg/equities-division/research ]
GW: Let me add my congratulations on the very strong data set. Joe, with respect to concordance with disease control & response, can you tell us whether you had a chance to interrogate the data to see whether there is some concordance there with Response and OS?
Joe Shan: No, we have not looked at that extensively because again, historically, response rates are a very poor prognosticator for survival. In this case and obviously, we had seen overall across groups, a similar trend of increased response rates in a prolonged PFS, and now, certainly the survival prolongation. The short answer is no, we have not really tried to correlate those 2 because it's not necessarily a shrinking of tumors on radiograph that leads to this. In fact, an interesting point is that there was a comment from the session chair [9-7-12 Gerber/Chicago] about applicability of RECIST-based definitions, and if you evaluate the drugs such as bavituximab, that might have an immune sort of component and that may not be the best way to evaluate. And certainly, again, we are looking at the survival end point as really the one that determines the activity, the meaningful activity, and not merely relying on a surrogate.
GW: And with respect to time to best response, there's been some observations that other immunologically active agents have a much delayed time to best response. Was there any difference in the time to best response in either the control or the bavi arms?
Joe Shan: I don't know the exact results at the moment, but I can say that, by and large, no, there were no differences in when patients responded. Keep in mind, they were only on chemotherapy for up to 6 cycles and that's one of the reasons why, in a study of this design, that you actually cap it, otherwise, there could be imbalances in the number of chemotherapy cycles. [indiscernible] So, for responses, they have to basically achieve them very quickly in the first few cycles.
GW: Lastly, with respect to survival, have you had a chance to review the narratives around death? Do you see any differences in the side of failure or ultimate cause of the demises of the patients between the control and the bavi arms that might be informative as to how the drug is working in the study?
Joe Shan: Sure. No, we haven't done statistical analysis. Certainly, we view all SAEs that result in death - generally, disease progression is the primary cause of death. So, it's an outcome of their disease process and not so much of toxicity or such.
MR. KING’S CLOSING COMMENTS:
I would like to thank everyone, again, for participating today's quarterly conference call. We certainly look forward as we continue to advance the bavituximab program and make other advancements in our overall corporate activities, and look forward to discussing that at our next earnings call in December. Thank you very much.
*end*
.
.
= = = = = = = = = = = = =
Latest 10K 4-30-12 iss. 7-16-12: http://tinyurl.com/79o57b2 PR: http://tinyurl.com/c8nytow (Cash 4-30-12 $18.0mm)
Latest 10Q 7-31-12 iss. 9-10-12: http://tinyurl.com/9sd8nua PR: http://tinyurl.com/9f85fdo (Cash 7-31-12 $19.0mm)
ALL SEC filings for PPHM: http://tinyurl.com/6d4jw8
.
.

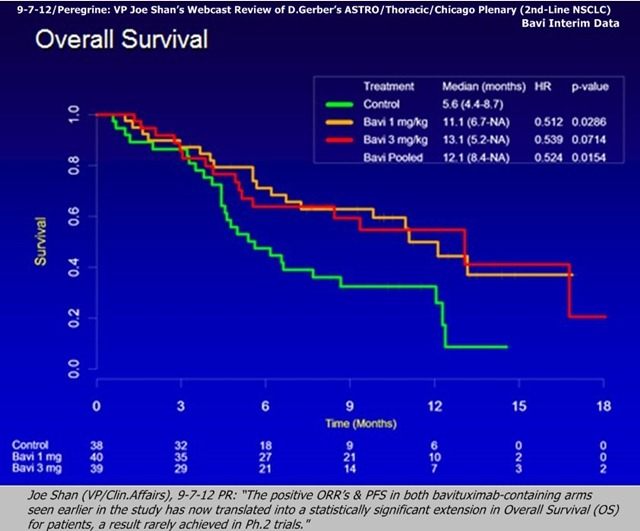
• 9-7-12: Press Release about Dr. Gerber's plenary at ASTRO/Thoracic/Chicago: http://tinyurl.com/8oxwk6v - "The interim data showed a statistically significant improvement in OS (Hazard Ratio 0.524, p-value .0154) and a doubling of MOS (12.1/13.1mos. vs. 5.6mos.) in the Bavituximab-containing arms compared to the [Docetaxel] ctl-arm."
• VP Joe Shan's 15min. Webcast & Slideshow recapping Dr. David Gerber's 9-7-12 ASTRO/Chicago Plenary: http://tinyurl.com/8cn87la
8-2012: Compare Bavi+Doce's MOS=13.1mos (Bavi/3mg) to the 4 Curr-Approved 2Line/NSCLC Drugs http://tinyurl.com/cgnkvpa
• Taxotere/docetaxel => MOS=6.3mos (meta-analysis of 5 trials, 865 pts)
• Altima/pemetrexed=> No diff. vs. Docetaxel (Ph.3 non-inferiority vs. Doce, 571 pts)
• Tarceva/erlotinib => MOS=5.3mos (TITAN Ph.III n=424 trial - see http://tinyurl.com/8w8lo93 )
• Iressa (gefitinib )=> "Iressa does not improve OS"
= = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = =
PR 9-10-12: FY’13/Q1 Financials & Devs (q/e 7-31-12)
Peregrine Pharmaceuticals Reports First Quarter Fiscal Year 2013 Financial Results and Recent Developments
• Interim Data Show Doubling of Median Overall Survival in Bavituximab-Treated Patients from Double-Blind, Placebo-Controlled Phase II Trial in 2nd-Line NSCLC
• Recent Data Strongly Support Advancing Bavituximab Program Into Phase III Clinical Development
http://ir.peregrineinc.com/releasedetail.cfm?ReleaseID=705887
TUSTIN, 9/10/2012: Peregrine Pharmaceuticals, Inc. (NASDAQ: PPHM), a biopharmaceutical company developing first-in-class monoclonal antibodies focused on the treatment and diagnosis of cancer, today announced financial results for the first quarter ended July 31, 2012 of fiscal year (FY) 2013 and provided an update on its advancing clinical pipeline and other corporate developments.
"We have achieved major milestones since the end of last quarter with the unblinding of our proof-of-principle bavituximab study in 2nd-Line NSCLC in May and the recent announcement of overall survival data from the study being the most significant. The statistically significant overall survival seen in that study is an obvious green light for us to begin plans to advance the program into Phase III and goes a long way toward validating the technology platform," said Steven W. King, president and CEO of Peregrine. "Following these exciting developments, the upcoming milestones for the program include additional clinical data from 8 ongoing bavituximab clinical trials, an end of Phase II meeting with the FDA expected by year end, and potential partnership as the result of ongoing discussions. This is truly an exciting time at Peregrine and we look forward to advancing the bavituximab program as well as the rest of our business operations."
BAVITUXIMAB ONCOLOGY PROGRAM HIGHLIGHTS
Lead Indication: 2nd-Line NSCLC
Last week, in a late-breaker, oral plenary presentation at the 2012 Chicago Multidisciplinary Symposium in Thoracic Oncology meeting, interim data was presented [ 9-7-12: http://tinyurl.com/8oxwk6v ] from a randomized, double-blind, placebo-controlled Phase IIb trial evaluating two dose levels of bavituximab (bavituximab-containing arms) plus docetaxel versus docetaxel plus placebo (control arm) in 2nd-Line Stage IIIb/IV NSCLC (NSCLC). This trial enrolled 121 patients with 2nd-Line Stage IIIb or Stage IV non-squamous NSCLC following one prior chemotherapy regimen and patients were equally randomized to 1 of the 3 treatment arms, with 117 of the enrolled patients being evaluable per the clinical protocol. Patients received up to 6 cycles of docetaxel (75mg/m2) plus either placebo, 1 mg/kg bavituximab, or 3 mg/kg bavituximab until disease progression. Recent data from the trial showed a doubling of median overall survival (OS) in both bavituximab-containing arms compared to the control arm and a statistically significant improvement in overall survival. In addition, bavituximab continues to be well-tolerated. Given the magnitude of this data, Peregrine is preparing for an End-of-Phase II meeting with the U.S. Food and Drug Administration (FDA) by the end of calendar year 2012 that should allow us to initiate Phase III by mid-2013.
"The unique immune directed attack of bavituximab and preliminary survival advantage of far greater magnitude than what has been observed historically with anti-angiogenesis agents provide potentially yet another example of clinically relevant immune directed therapy moving forward," said John Nemunaitis, M.D., executive director of the Mary Crowley Cancer Research Centers and an investigator in Peregrine's Phase II bavituximab 2nd-Line NSCLC clinical trial.
Additional Bavituximab Clinical Trials
Peregrine currently has 7 additional ongoing clinical trials as follows:
• A randomized, open-label, Phase II clinical trial evaluating bavituximab plus carboplatin and paclitaxel versus carboplatin and paclitaxel alone in 83 evaluable patients with previously untreated [Front-Line] Stage IIIb or Stage IV NSCLC patients completed enrollment in September of 2011 and the event-driven median overall survival data will be available upon maturation.
• A randomized, open-label, Phase II clinical trial evaluating bavituximab plus gemcitabine versus gemcitabine alone in 70 patients with previously untreated [Front-Line] Stage IV Pancreatic Cancer completed enrollment in June 2012. The primary endpoint, median OS, is an event-driven endpoint and will be reported once reached.
• Phase I/II Investigator Sponsored Trial (IST) investigating bavituximab in combination with sorafenib in patients with Advanced Hepatocellular Carcinoma (Liver Cancer). The Phase I portion of the trial has completed patient enrollment.
• A Phase I/II IST evaluating bavituximab in combination with cabazitaxel in patients with 2nd-Line Castration-Resistant Prostate Cancer [CRPC].
• A Phase Ib IST evaluating bavituximab in combination with carboplatin and pemetrexed in patients with previously untreated [Front-Line] Stage IV NSCLC.
• A Phase I IST evaluating bavituximab in combination with paclitaxel in up to 14 patients with HER2-negative Metastatic Breast Cancer.
• A Phase I IST evaluating bavituximab in combination with capecitabine and radiation therapy in patients with Stage II or III Rectal Adenocarcinoma.
COTARA PROGRAM HIGHLIGHTS
Peregrine's single-administration approach to treating recurrent glioblastoma multiforme (GBM) has shown encouraging 9.3 month median overall survival data from a Phase II trial in 41 patients. Peregrine and the FDA continue to advance discussions surrounding the negotiation of a pivotal trial design. The company plans to seek partners both in the U.S. and internationally to support the development of Cotara for this deadly form of brain cancer.
IMAGING PROGRAM HIGHLIGHTS
PS-Targeting Molecular Imaging Program
In April 2012, Peregrine launched its experimental phosphatidylserine (PS)-targeting molecular imaging candidate, 124I-PGN650, into clinical development for the imaging of multiple solid tumor types. The primary goal of the trial [ http://clinicaltrials.gov/ct2/show/NCT01632696 ] is to estimate radiation dosimetry in critical and non-critical organs. Secondary objectives of the trial are tumor imaging and safety. Patients are currently being enrolled in the trial.
FINANCIAL RESULTS
Total revenues for the first quarter of FY 2013 were $4,251,000, compared to $5,655,000 for the same quarter of the prior fiscal year. This decrease was primarily attributable to lower contract manufacturing revenue generated by Peregrine's biomanufacturing subsidiary Avid Bioservices, which generated contract manufacturing revenue of $4,135,000 for the first quarter of FY 2013, compared to $5,439,000 for the same quarter of the prior fiscal year. The decrease in contract manufacturing revenue was primarily due to a decrease in the number of completed manufacturing runs released and shipped during the current quarter, which can be attributed to the timing of services provided to Avid's third-party clients. However, based on current manufacturing commitments from Avid's third-party clients for services to be provided during the remainder of FY 2013, we expect contract manufacturing revenue to be at least $15 million for FY 2013. In addition, Avid will continue to utilize available capacity and resources to continue its preparation for later stage clinical development and potential commercialization of bavituximab and Cotara, while also seeking to grow its services from third-party clients.
Total costs and expenses decreased $1,784,000 to $11,922,000 in the first quarter of FY 2013 from $13,706,000 in the first quarter of FY 2012. This decrease was primarily attributable to lower contract manufacturing costs incurred by Avid combined with lower research and development expenses associated with lower clinical trial costs. For the first quarter of FY 2013, cost of contract manufacturing and R&D expenses were $2,024,000 and $6,981,000, respectively, compared to $3,017,000 and $7,760,000, respectively, for the first quarter of FY 2012. Selling, general and administrative expenses for the first quarter of FY 2013 were $2,917,000 and were in-line with the first quarter of FY 2012.
Peregrine's consolidated net loss was $7,664,000, or $0.07 per basic and diluted share, for the first quarter of FY 2013, compared to a net loss of $8,092,000, or $0.11 per basic and diluted share, for the same quarter of the prior year.
Peregrine reported $18,991,000 in cash and cash equivalents at July 31, 2012, compared to $18,033,000 at April 30, 2012. Subsequent to July 31, 2012, Peregrine announced that it had secured a $30 million term loan from Oxford Finance, MidCap Financial, and Silicon Valley Bank. Under the loan agreement, the company received initial funding of $15 million upon closing on August 30, 2012, and has an option to receive an additional $15 million, provided, on or before March 31, 2013, Peregrine meets certain predefined milestones, as described in loan agreement.
More detailed financial information and analysis may be found in Peregrine's Quarterly Report on Form 10-Q, which will be filed with the Securities and Exchange Commission today. [10-Q 7-31-12 iss. 9-10-12: http://tinyurl.com/9sd8nua ]
Conference Call
Peregrine will host a conference call and webcast this morning, September 10, 2012, at 11:00 AM ET (8:00 AM PDT). To listen to the conference call, please dial (877) 312-5443 or (253) 237-1126 and request the Peregrine Pharmaceuticals conference call. A replay of the call will be available starting approximately two hours after the conclusion of the call through Sept. 24, 2012 by calling (855) 859-2056, or (404) 537-3406 and using passcode 27367274 . To listen to the live webcast, or access the archived webcast, please visit: http://ir.peregrineinc.com/events.cfm
ABOUT PEREGRINE PHARMACEUTICALS, INC.
Peregrine Pharmaceuticals, Inc. is a biopharmaceutical company with a portfolio of innovative monoclonal antibodies in clinical trials focused on the treatment and diagnosis of cancer. The company is pursuing multiple clinical programs in cancer with its lead product candidate bavituximab and novel brain cancer agent Cotara®. Peregrine also has in-house cGMP manufacturing capabilities through its wholly-owned subsidiary Avid Bioservices, Inc. ( http://www.avidbio.com ), which provides development and biomanufacturing services for both Peregrine and outside customers. Additional information about Peregrine can be found at http://www.peregrineinc.com .
Safe Harbor *snip*
PEREGRINE PHARMACEUTICALS, INC.
CONDENSED CONSOLIDATED STATEMENTS OF OPERATIONS AND COMPREHENSIVE LOSS
THREE MONTHS ENDED
----------------------------
July 31, 2012 July 31, 2011
------------- -------------
Unaudited Unaudited
REVENUES:
Contract manufacturing revenue $ 4,135,000 $ 5,439,000
License revenue 116,000 216,000
------------- -------------
Total revenues 4,251,000 5,655,000
COSTS AND EXPENSES:
Cost of contract manufacturing 2,024,000 3,017,000
Research and development 6,981,000 7,760,000
Selling, general and administrative 2,917,000 2,929,000
------------- -------------
Total costs and expenses 11,922,000 13,706,000
------------- -------------
LOSS FROM OPERATIONS (7,671,000) (8,051,000)
------------- -------------
OTHER INCOME (EXPENSE):
Interest and other income 8,000 13,000
Interest and other expense (1,000) (54,000)
------------- -------------
NET LOSS $ (7,664,000) $ (8,092,000)
============= =============
WEIGHTED AVERAGE COMMON SHARES OUTSTANDING
Basic and diluted 103,283,937 70,656,568
============= =============
BASIC AND DILUTED LOSS PER COMMON SHARE $ (0.07) $ (0.11)
============= =============
COMPREHENSIVE LOSS $ (7,664,000) $ (8,092,000)
============= =============
PEREGRINE PHARMACEUTICALS, INC.
CONDENSED CONSOLIDATED BALANCE SHEETS
JULY 31, APRIL 30,
2012 2012
------------- -------------
Unaudited
ASSETS
CURRENT ASSETS:
Cash and cash equivalents $ 18,991,000 $ 18,033,000
Trade and other receivables, net 2,271,000 2,353,000
Inventories, net 5,744,000 3,611,000
Prepaid expenses and other current assets,
net 887,000 795,000
------------- -------------
Total current assets 27,893,000 24,792,000
Property, net 2,868,000 2,900,000
Other assets 745,000 570,000
------------- -------------
TOTAL ASSETS $ 31,506,000 $ 28,262,000
============= =============
LIABILITIES AND STOCKHOLDERS' EQUITY
CURRENT LIABILITIES:
Accounts payable $ 4,151,000 $ 3,492,000
Accrued clinical trial and related fees 1,909,000 2,111,000
Accrued payroll and related costs 2,908,000 2,468,000
Deferred revenue 6,056,000 3,651,000
Customer deposits 10,224,000 4,865,000
Other current liabilities 1,308,000 1,052,000
------------- -------------
Total current liabilities 26,556,000 17,639,000
Deferred revenue 284,000 361,000
Other long-term liabilities 742,000 779,000
Commitments and contingencies
STOCKHOLDERS' EQUITY:
Preferred stock-$0.001 par value; authorized
5,000,000 shares; non-voting; nil shares
outstanding - -
Common stock-$0.001 par value; authorized
325,000,000 shares; outstanding - 104,178,431
and 101,421,365, respectively 104,000 101,000
Additional paid-in capital 349,608,000 347,506,000
Accumulated deficit (345,788,000) (338,124,000)
------------- -------------
Total stockholders' equity 3,924,000 9,483,000
------------- -------------
TOTAL LIABILITIES AND STOCKHOLDERS' EQUITY $ 31,506,000 $ 28,262,000
============= =============
Contact: Christopher Keenan or Jay Carlson
Peregrine Pharmaceuticals, Inc., (800) 987-8256, info@peregrineinc.com
= = = = = = = = = = = = =
Latest 10K 4-30-12 iss. 7-16-12: http://tinyurl.com/79o57b2 PR: http://tinyurl.com/c8nytow (Cash 4-30-12 $18.0mm)
Latest 10Q 7-31-12 iss. 9-10-12: http://tinyurl.com/9sd8nua PR: tp://tinyurl.com/9f85fdo (Cash 7-31-12 $19.0mm)
ALL SEC filings for PPHM: http://tinyurl.com/6d4jw8
((( Orig. transcript from SeekingAlpha.com [ http://tinyurl.com/8prvsbn ], with numerous corrections made. )))
Link to webcast replay: http://ir.peregrineinc.com/eventdetail.cfm?eventid=118444
NOTE: 9-10-12 Financials Press Release is included at the end of this post.
C.C. EXCERPTS:
…STEVE KING (CEO): “The exclamation point for these milestones came just last Friday [9-7-12] with a report that patients receiving Bavi+chemo in our proof-of-concept study in 2nd-Line NSCLC had doubled the MOS compared to patients receiving chemotherapy+placebo. These are truly remarkable results that are not only great for the program, providing a clear signal to proceed toward a Phase III clinical trial, providing proof-of-concept that bavituximab is an active drug when given with docetaxel, but also great news for the NSCLC patients in the trial…”
…ROB GARNICK (HEAD/REGULATORY): “As you have just heard from Joe, the data we announced last week [9-7-12/Gerber/Chicago] has far exceeded our expectations, and I hope that you're as excited as I am with bavituximab's potential. I feel strongly that Peregrine should be recognized for having the corporate courage to conduct the rigorous, randomized placebo-controlled Phase II trial that provided these robust data and that provide the basis for us to plan for a pivotal Phase III program. We took an extraordinary amount of care in developing this Phase II trial design and conferred with clinical experts & regulatory agencies, including the FDA, in the design of this rigorous clinical trial. Peregrine chose to conduct this trial to definitively establish the proof of concept to bavituximab and now plans to potentially include this data as part of a registrational package. Having personally been involved in the evaluation of over 30 Phase II trials over my career, none of which ever achieved statistical significance, including many of today's blockbuster biotech products, I am personally extremely pleased with the quality of this data and the clarity with respect to advancing bavituximab in Phase III trials which it provides. Our next steps are to present the data you saw last week to global regulatory authorities as part of the formal End of Phase II [EOP2] meetings from which we anticipate gaining concurrence into the planning & execution of a pivotal trial program. Normally, it takes approx. 60 days to arrange such EOP2 meetings, and following these meetings to submit IND amendments for the Phase III and initiate the trial by mid-2013. . .Q&A: “I think the regulators will be very excited [about the 2nd-Line NSCLC data]. Certainly, the FDA had a lot of input into our trial design, and I think they gave us some a very wise counsel and I think this is exactly the kind of study that they would like to see. And certainly it provides for us the clarity, which you rarely have in Phase II trials, to decide to go clearly into a Phase III study and to actually really focus on replicating what we've just done. And I think that de-risks the program enormously, and really gives us a lot of confidence in how to go forward...”
FULL TRANSCRIPT…
9-10-2012 Q1 FY’13 Earnings Conf. Call (q/e 4-30-12)
WELCOME & FWD-LOOKING STATEMENTS: Jay Carlson (IR) http://www.peregrineinc.com
Speakers: Steve King, Joe Shan, Robert Garnick, Paul Lytle; Q&A session at end.
CEO Steve King – OPENING COMMENTS:
Since the beginning of last quarter, it has been an exceptional time for Peregrine, as we have seen 2 of the most important milestones in the company history achieved, transitioning the company toward late-stage drug development. The exclamation point for these milestones came just last Friday [9-7-12] with a report that patients receiving bavituximab + chemotherapy in our proof-of-concept study in 2nd-Line NSCLC had doubled the Median Overall Survival (MOS) compared to patients receiving chemotherapy + placebo. These are truly remarkable results that are not only great for the program, providing a clear signal to proceed toward a Phase III clinical trial, providing proof-of-concept that bavituximab is an active drug when given with docetaxel, but also great news for the NSCLC patients in the trial. While moving toward this important data, we also strengthened our balance sheet with a $30 million debt financing at favorable terms and continued to see good performance at our mfg. subsidiary, Avid Bioservices, successfully navigating regulatory inspections and posting another solid quarter of revenues. We are continuing to deliver on the milestones laid out earlier in the year and have more important events coming throughout the rest of this year, including our continuing bavituximab partnering discussions and due diligence, which remains a highly active area, preparing for an End of Phase II meeting for the bavituximab program and waiting additional clinical results from 8 ongoing clinical trials that will help further shape the program. With that, I will now turn the call over to Joe for a recap of the exciting clinical data that was presented last week.
JOE SHAN (VP/Clin.&Reg. Affairs) – CLINICAL TRIALS:
I'd like to start by reviewing important details of the clinical data from our Phase II 2nd-Line bavituximab NSCLC trial that was just presented last Friday [9-7-12 http://tinyurl.com/8oxwk6v ] in the Plenary session of the 2012 Chicago Multidisciplinary Symposium In Thoracic Oncology. I also encourage everyone to listen to the prerecorded webcast that can be found on our website for a more detailed discussion of the data presentation.
So trial file for our lead indication is a randomized, double-blinded placebo-controlled Phase II trial evaluating docetaxel with or without bavituximab as 2nd-Line treatment in patients with Stage IIIb or IV non-squamous NSCLC [ http://clinicaltrials.gov/ct2/show/NCT01138163 ]. On study, all patients received std. 2nd-Line chemotherapy of up 6 to 21 day cycles of docetaxel at 75ml/m2. In addition, patients were randomly assigned to receive a blinded weekly infusion of placebo, which we refer to as the controlled group, or 1 of 2 bavituximab doses studied, either 1 or 3 mg/kg until progression or toxicity. The primary endpoint of this trial is Overall Response Rate (ORR) and secondary endpoints include PFS, Overall Survival (OS), and safety. Between Oct.2010 and Oct.2011, 121 patients were enrolled at 40 global trial centers. No single center enrolled a substantial number of patients and approx. 50% of the patients enrolled were enrolled in U.S. centers with the remainder enrolled in Europe & India. All patients were previously treated with 1 prior platinum containing doublet regimen. Patient & disease characteristics were well-balanced across the 3 study groups with no differences in age, gender, race, ECOG or performance status, stage of disease, or prior treatments which could have significantly impacted the study results. Bavituximab continues to demonstrate a favorable safety profile with the combination of docetaxel + bavituximab being well tolerated, with no increase in frequency or nature of adverse events compared to the control arm. Notably, no increase in bleeding or clotting adverse events were reported with the addition of bavituximab, unlike the experience with other compounds which target blood vessels.
In terms of efficacy outcomes, let me start with a primary endpoint, ORR, which was determined by indep. central radiology reviews, according to RECIST criteria or Response Evaluation Criteria In Solid Tumors. As reported in May’12 when the study was initially unblinded, the ORR in the docetaxel+placebo arm was 8% compared to 15% in the bavituximab 1mg/kg arm; and 18% in the bavituximab 3mg/kg arm; and 16.5% in the pooled bavituximab arm. Though the response rate of the bavituximab-containing arms was double that of the control group, this trend favoring bavituximab did not reach the statistical significance, with P-values in the 0.2 to 0.3 range. This was expected as this trial has power to detect an 8% vs. 26% response rate, which is more than a 3-fold difference at a significance level of 0.15, not 0.05. This is expected also in a Phase II setting, as the main purpose of a trial of this size is to determine whether a drug candidate is promising enough to move into a larger Phase III trial with more statistical power.
Next, PFS also favored both bavituximab-containing arms with P-values approaching significance levels. Again, based on indep. central radiology review, median PFS and the docetaxel+placebo arm was 3.0 mos. In the docetaxel+bavituximab 1mg/kg arm, median PFS was 4.2 mos., corresponding to a Hazard Ratio (HR) of 0.57 with a P-value 0.08. In the docetaxel+bavituximab 3mg/kg arm, median PFS was 4.5 mos., corresponding to a HR of 0.65 with a P-value 0.19. In the docetaxel+pooled bavituximab arms, median PFS was 4.2 mos. with a HR of 0.6 and a P-value of 0.07.
Now, turning to Overall Survival (OS), another secondary endpoint in the trial, but the preferred efficacy endpoint, which represents direct clinical benefit. At the time of this analysis, over 70% of patients in the control group had died, while less than 50% had died in either bavituximab arm, and survival follow-up is continuing. The Kaplan–Meier [K-M] graph illustrates a clear and persistent separation of the survival curves favoring both bavituximab arms, demonstrating that OS is clinically and statistically significantly prolonged in the bavituximab arms. Specifically, in the docetaxel+placebo arm, the MOS estimate is 5.6 mos., while in the docetaxel+bavituximab 1mg/kg, the MOS estimate is 11.1 mos., with a HR of 0.51 and a significant P-value of 0.029. In the docetaxel+bavituximab 3mg/kg arm, the MOS estimate is 13.1 mos., with a HR of 0.54 and a P-value of 0.071. In the pooled bavituximab arm, the MOS estimate is 12.1 mos. with a HR 0.52 and a significant P-value of 0.015.
We have performed extensive subgroup analyses on these data and in both the 1mg & 3mg bavituximab arms subgroup analysis by age, gender, race, performance status and histologic subgroups showed a positive trend toward improved survival with bavituximab. Also, the survival results were comparable between patients from the U.S., Europe and India, suggesting treatment benefit does not appear to be limited to a subset of particular patients or where they were enrolled. Based on the positive outcome in OS, we're in the process of collecting available data of subsequent treatment at progression and so far, there does not appear to be any differences across the groups.
It is important, at this point, to reiterate that was a randomized, blinded placebo-controlled trial, in which no one knew what the patients were receiving in addition to docetaxel, and the treatment & procedure schedules were identical in all 3 arms. We could not have conducted a less-biased trial. The fact that the groups were well-balanced coming into the study, and both bavituximab arms showed similar benefit compared to the control arm, and that these significant interim survival results were not limited to a subset of patients, strongly support that bavituximab is an active agent which should be advanced into Phase III development. As you can imagine, we are very pleased with these interim results and look forward to announcing final results when available. Meanwhile, we are working towards the previously stated goals of meeting with the FDA before the end of this year in order to initiate a confirmatory Phase III trial by the middle of next year. I would now like to turn the call over to Rob for a regulatory update.
Dr. Robert Garnick (Head of Regulatory Affairs)
As you have just heard from Joe, the data we announced last week [9-7-12/Gerber/Chicago] has far exceeded our expectations, and I hope that you're as excited as I am with bavituximab's potential. I feel strongly that Peregrine should be recognized for having the corporate courage to conduct the rigorous, randomized placebo-controlled Phase II trial that provided these robust data and that provide the basis for us to plan for a pivotal Phase III program. We took an extraordinary amount of care in developing this Phase II trial design and conferred with clinical experts & regulatory agencies, including the FDA, in the design of this rigorous clinical trial. Peregrine chose to conduct this trial to definitively establish the proof of concept to bavituximab and now plans to potentially include this data as part of a registrational package. Having personally been involved in the evaluation of over 30 Phase II trials over my career, none of which ever achieved statistical significance, including many of today's blockbuster biotech products, I am personally extremely pleased with the quality of this data and the clarity with respect to advancing bavituximab in Phase III trials which it provides. Our next steps are to present the data you saw last week to global regulatory authorities as part of the formal End of Phase II [EOP2] meetings from which we anticipate gaining concurrence into the planning & execution of a pivotal trial program. Normally, it takes approx. 60 days to arrange such EOP2 meetings, and following these meetings to submit IND amendments for the Phase III and initiate the trial by mid-2013.
Touching on Cotara for a moment, Peregrine and the FDA are continuing to have positive discussions about the design & execution of a pivotal trial in GBM. We appreciate your patience as we just strive to gain the most advantageous strategy for both parties for this novel and potentially important drug candidate.
CFO Paul Lytle:
I'd like to spend the next few moments covering a few financial highlights and our related financial goals. As I mentioned on the last call, it's important to understand that we operate a hybrid business model that includes a revenue-generating contract mfg., business and an advancing drug dev. business.
Let me first focus on our contract mfg. business. During the last quarter, Avid generated $4.1 million in contract mfg. revenue, and we reiterate our revenue guidance of least $15mm for FY 2013. In addition to the non-diluted revenue we received from Avid, on the last earnings call [7-16-12 http://tinyurl.com/cs7spbz ], we mentioned that our next immediate focus was to secure a less dilutive debt financing vehicle similar to a term loan, in the range of $20-30mm. We recently executed on our stated milestone and closed on a $30 million term loan with 3 extremely well-respected institutions: Oxford Finance, MidCap Financial and Silicon Valley Bank. Under the loan facility, we received initial funding of $15mm on 8-30-12, and we have an option to receive an addl. $15mm in funding. This 2nd tranche becomes available to us upon the attainment of certain predetermined milestones, one of which was just achieved last Friday [9-7-12] with the announcement of the positive OS data from our 2nd-Line lung cancer trial. The 2nd related milestone pertains to having a positive EOP2 meeting with the FDA, defined as our ability to move into the Phase III trial design, and we plan to have that end of Phase II meeting with the FDA before the end of this year.
Another potential source of capital we are focused on pertains to our unencumbered pipeline. As you can imagine, given the bavituximab results that we shared with you on Friday, our partnering activities are continuing at a very active pace as we move closer towards the end of Phase II meeting with the FDA. Our stated goal is to have a partner on board before we start the Phase III trial and, preferably, before the EOP2 meeting with the FDA, as we would like our future partner to be a part of that important meeting. These are very exciting times for Peregrine and we have been diligent in executing against our stated milestones. We look forward to keeping you updated on our progress, and we will now open the call up to your questions.
Q&A: [21:15 mark]
1. Joe Pantginis – Roth Capital Partners: [ http://www.roth.com & https://roth2.bluematrix.com/docs/pdf/BLUE.pdf ]
JP: First, I just wanted to confirm something that I heard on Friday when Dr. Gerber presented the data. Can you confirm, did they say that the IDMC was the group that recommended pooling the data?
Joe Shan: Yes, that's true. So, typical on these sort of blinded studies, you have an IDMC who can independently look at some of the results in advance of being unblinded, and a central analysis plan is typical where you want to look at each group compared to the control separately. But because those 2 dose levels performed so similarly from each other, but better than the control group, it was recommended that we do a pro [indiscernible] exploratory pooled analysis.
JP: Thanks for providing the geographical breakdown update (earlier) - that was really helpful. If you could maybe further breakdown a couple of nuances here. Have you or will you be looking at any of the potential mutation statuses of the patients in this study? And also, have you looked at the outcomes of the patients that was a range from 15-20% of patients that received prior Avastin?
Joe Shan: Geographically, I think we mentioned that there were really no differences, and the reason why we couldn't get into all the details is there was a limited amount of time for Dr. David Gerber. As far as mutation status, that was not a requirement to enter the study, and recall, PS is a broadly-expressed target across multiple tumor types, so we did not collect that information on genetic mutations. In terms of outcomes, we did look at, for example, the % of patients who received prior Avastin as part of their frontline therapy, and there were no differences in outcomes with respect to that. There really were no other large enough groups to subset out.
JP: Two more quick questions. Obviously, you just alluded to part of the moa for bavi. For this study or any of the current ISTs, and even the planned Phase III, what particular immune parameters will you be looking at, such as, say, infiltration of cytotoxic T-lymphocytes or any other parameters?
Steve King: We're trying to build in some of that analysis, particularly into our ISTs. They're a little bit cumbersome to build into large studies, especially large blinded studies, as we might be running in the future. But, you’re on the right track, the immune status of the particular immune cells that are inside the tumors through tumor biopsies. We're also building in tumor blood flow measurements - that's particularly in one of our other NSCLC studies. When you think about the moa and how it relates to preclinical studies, we're trying to really build in those same sort of analysis into some more clinical studies.
JP: Lastly, Rob, you mentioned the fact that with your broad experience with multiple Phase II studies, highlighting the fact that Phase II studies are, obviously, not powered for statistical significance, and now you see these data here today; how do you think these data will affect the tenor based on your multiple interactions with the FDA in the past with your upcoming EOP2 meeting?
Robert Garnick: I think the regulators will be very excited. Certainly, the FDA had a lot of input into our trial design, and I think they gave us some a very wise counsel and I think this is exactly the kind of study that they would like to see. And certainly it provides for us the clarity, which you rarely have in Phase II trials, to decide to go clearly into a Phase III study and to actually really focus on replicating what we've just done. And I think that de-risks the program enormously, and really gives us a lot of confidence in how to go forward.
2. Charles Duncan (JMP Securities): [8-30-11 coverage init: http://tinyurl.com/3crdwqz ]
CD: I'm wondering about the control arm experience. There’s been lots bantering about in terms of the MOS, it does seem like it's within the range. But do you think that 5.6 month number is low, and is it driven by the % of patients that are really Stage IV vs. IIIb? What’s your perspective on that?
Steve King: With regard to the Stage of patients, I think in all the arms, it was around 90% Stage IV, so I don't think it's in any way related to that. If you look historically at the experience of docetaxel, that we are within the range at that 5.6 months, maybe on the low end of the range, but it's certainly consistent with some of the prior clinical trial results. In effect, if you look at some of the interim data that's been presented from some of the other trials involving docetaxel, it's very consistent with those results as well. And I think it's important that, while there's talk about well, it’s on the low-end, keep in mind that this is the reason the gold std. type of study to run is a double-blinded placebo-controlled study, because this is a patient population that is consistent with the entry criteria for all the arms; it's meant to be a solid control for this particular study. Otherwise, you could compare with historical results for docetaxel and say that, "Well, we beat the previous record for docetaxel and so it must be a good result." But really, this is the gold std. study – it’s meant to remove all the bias, make sure you have a similar patient population receiving the same dosing regimen with the same criteria and the same SOC. With that said, I think it's a clear result. I think it's actually remarkable that it's readout as a statistically significant result in OS. But again, it's what the FDA would expect, and as we think about what's the next trial going to look like, the Phase III, well, obviously, it's going to look very, very similar to this trial. In fact, with as few deviations from this trial design as possible because that is what will give us the highest probability of success.
Joe Shan: Steve, you already sort of hit the nail on the head. I mean, this is the reason why randomized clinical trials are conducted; you really shouldn't compare across studies. You do that early on when you have limited experience just as a benchmarking exercise, but you have to run randomized clinical trials and interpret the data in that context of that study, that subgroup. And we've already said that this is a smallish trial, it's not statistically-powered to show major significance. But, we did see that, and when we looked at the subgroups and the balance of patients coming into the study, it was well-balanced. So, there really isn't anything else we can say in trying to compare the number we saw on the docetaxel arm to other published studies. If you run enough studies and you can do some sort of meta-analysis, it certainly would fit in on the control results.
CD: I absolutely agree & appreciate the rigor of the design, and clearly, compelling and at least in my mind, clinical proof-of-concept. I'm wondering what you would do if anything different as as you go into Phase III. I know you haven't had your EOP2 meetings yet with the agency, but can you share with us, in terms of powering, how much would you discount these results in terms of the magnitude of benefit that you would look for in Phase III, and what would you do different if anything in terms of geography or the entry criteria that Steve mentioned with regard to defining these patients and what they have?
Joe Shan: As we stated, we feel the results from this Phase II are so clear & compelling that we want to change as little as possible going to a Phase III and really replicate hopefully these results. And, recognizing that usually Phase II data look better than Phase III, and so it's a little chip on the egg. We are not going to be overly ambitious in the statistical assumptions going into Phase III. We've stated before that we'd like to keep the Phase III study in the 300 to 500 patient range, and, working backwards, you can imagine it's going to be a Hazard Ratio of less than 0.8, but not as low as 0.5, so somewhere in between there. And, of course, significance of at least 0.05, with probably 8% or 9% power. These are very standard assumptions for Phase III, and I think we have the Phase II data to really support that type of assumption.
Robert Garnick: Just a quick follow-on to what Joe said, I think the std. for approval for a drug in 2nd-Line NSCLC will be another trial that would replicate this one, and as Steve said, as closely as possible. I'm not sure what else we would do different other than increase the “N” of the patients. And once we have that data, the combination of information between this trial and the next one, the pivotal Phase III - the plan would be that, that would be the data that we'll need to achieve an approval. I think if we achieve anywhere near the degree of clarity that we just obtained, I think this will be a pretty straightforward approval process. I'm sure the FDA would agree with me; the FDA as well as other global regulatory authorities would agree, that this is a pretty straightforward design and we really just need to obtain concurrence on it and then to begin our execution by mid-2013.
Joe Shan: Charles, I forgot to address your comment about the geography in the Phase III. I think clearly, we want as many of the patients in the Phase III to be enrolled in where we would like to eventually market the product, so obviously, U.S. & Europe. We recognize that the skepticism of clinical trial results coming out of emerging clinical trial regions such as India or Eastern Europe. However, I think we demonstrated in the study that there were really no differences. But, of course, we're going to keep a close eye on actual enrollment and perhaps, to sort of cap the enrollment, if any particular country is enrolling a lot faster than others.
Steve King: The thing about partnering discussions, and one of the reasons we feel it will be a big benefit to have a potential partner on board in time for the EOP2 meeting is, it really gives you an opportunity to think through the strategy because again, we are viewing this as a global registration trial and certainly the U.S., Europe and potentially, other territories will be involved naturally. But, it's the benefit of being able to ask all the questions that you want to ask in that EOP2 meeting and to think through things like where you want to enroll the patients, as Joe mentioned. Because ideally, you want the majority of those patients to come from the territories in which you are actually seeking approval, and that's, obviously, a big benefit. So, it's one of the reasons we're really trying to move along the partnering discussions and at the same sort of tempo as we are in the EOP2 meeting preparations.
CD: Can you provide any additional color in terms of partnering strategy? Would you ideally seek an indication-specific partner? Or do you think that this could prove to be a broader platform accessing-type partnership that might result in development of the drug across different indications?
Steve King: We view this is as an oncology partnering exercise. So clearly, there is bavituximab, in which we have the clinical data and the program worked generally as it relates to treating cancer. Essentially, our strategy hasn't really changed - it's ideally an ex-U.S. partnership. I think it will be all indications within oncology. It's just too difficult to try to split up different oncology indications. But certainly, geography is a way to split up the partnering exercise. We think at the least, having some sort of a co-promote at the end of the day, so we still have a considerable upside left for Peregrine as we continue to advance this program toward, hopefully, eventual product approval. So, I'm still primarily focused on ex-U.S. partnering, but with the realization that we're going to achieve our broader goal of also bringing in the capital that allows the company to be financially secure through the end of Phase III readout, we think is an important part of that partnering discussion. So like I said, probably ex-U.S. partnering, with some sort of a co-promote in the U.S., is a reasonable outcome, and there's been quite a number of good comparables out there for deals recently.
3. George Zavoico (MLV): [ 2-8-10 coverage init: http://tinyurl.com/yech7gz ]
GZ: Let me add to the congratulations of the results of the Phase IIB trial; it is really quite extraordinary. My question relates to the platform technology that bavituximab represents. The moa actually suggests that it could be effective in many other cancers. But, Peregrine had to choose to do the trials in those that were most likely to succeed based on prior data. And now you're pursuing some of these other leads with ISTs. These [2nd-Line NSCLC] results obviously provide considerable confidence, certainly in the lung cancer. But, could you speak to how it affects your plans for other indications? Are you, in the partnering discussions for example, are you looking for companies that might expand on the indication, or just want to do the Phase III trial? So could you speak to that, please?
Steve King: I think that clearly our goal is to bring on a partner with the partnership to them, move the program not just into a Phase III study, but a Phase III study with addl. clinical trials that will help explore the broader potential of the technology platform. Because you're right, from our preclinical modeling, and what we believe will extrapolate to the clinic, we believe most solid tumors, if not all solid tumors, will be PS-positive, and that chemotherapy again, across many different types of chemotherapy, will up-regulate that target. The other aspect of running as broad a program as we can and, as you alluded to, we have currently 8 ongoing studies to look at many different combinations & indications. More than likely, we're going to find combinations that work better than others, and those are kind of the ones we want to really follow-on. So, as you can imagine, as we're thinking about future clinical trials, additional trials combining docetaxel are attractive because we had the earlier Phase IIa results with docetaxel in which we had the very nice OS data in the breast-cancer patients. The data from this study [2nd-Line NSCLC] is, obviously, extremely positive, we couldn't be happier with that. But, we think that there will be other combinations and indications that are particularly hot areas for development. And, the other counterpoint of that is the fact that we'll probably find some combinations that just don't look as attractive, and that’s part of the purpose of running the clinical trials we’re running, is to really guide the program into those areas we're going to have the best benefits. So, we're going to continue to cast a wide net, find all those indications & combinations that are particularly attractive and then, really take advantage of those. I think it's a very similar approach to what it's been used for other highly successful drugs - Avastin is one that comes to mind, and Rob might be able to add a little color to that. But, the bottomline is, we're really trying to follow a strategy we think is the best shot at having multiple indications for this drug at the end of the day.
Robert Garnick: Following on to what Steve said, one of the things that's always attracted me to bavituximab is the fact that it does have such a potential plethora of possible indications. And as you pointed out, we really went into NSCLC based on the signal-seeking data that we had originally gotten in early Phase I & II studies. I think that was a very wise way to go forward. Just like Avastin, as you'll remember, Avastin was first developed in colorectal cancer and then, having a broad anti-angiogenesis moa, we then were able to develop that drug into multiple other cancers where, theoretically, its moa would still apply. And of course, Avastin has gone on to become an extremely profitable and valuable drug in the oncology arena. So, we're thinking about a very, very similar strategy for bavituximab - basically, using these ISTs to guide you in terms of where you're most likely to succeed and in what combination of drugs to combine with bavituximab. I think, luckily, we're seeing very good safety signals with the drug, and that's really an important aspect that helps us to decide how broad the drug action can be applied. So using the ISTs and then potentially other signal-seeking Phase IIs, we plan to really maximize the benefit of this particular product. And I think we've got a broad potential and a bright future.
GZ: As a follow-on to that, one of the things you guys pointed out a little bit earlier was, that this was broadly Stage IIIb, IV and non-squamous NSCLC - you didn't really need to have any mutational status prerequisites here, and which also suggests sort of a broader implication for this drug. And maybe you can speak to that as well, but not only that, it also suggests that it might also be active in the frontline setting - you had equivocal results earlier this year. But the hard data coming out of the frontline is OS, which I guess we expect later this year. So, how does that change your view, and does this give you added confidence that perhaps the frontline data will also turn out to be more positive than first reported this year?
Steve King: Obviously, as we're thinking about the moa, the immunomodulatory activity of bavituximab, its ability to turn on the immune system that, clearly, that's something that could, at the end of the day, show the biggest benefit in OS as patients who are on treatment long enough were able to elicit a strong immune response, which then helps hold the disease in check for an extended period of time. Certainly, that factor fits right in with the 2nd-Line NSCLC data, where we're having the biggest impact on OS. And again, it's not unexpected with immunotherapies and it's been seen with other immunotherapies that are in the clinic or earlier reported results. So, I think that's something we could see across-the-board. I think every clinical trial is an individual study in order to look at a particular combination in a particular stage of disease. Some are going to work and undoubtedly, if we run enough studies, some are not going to have positive results. We're anxious, like everybody else is, to see the data from the frontline study. In addition to the carboplatin & paclitaxel combination randomized study, we're also be exploring, pemetrexed in a frontline setting, and so we do believe that frontline NSCLC should be a target and still has a good probability of success for the company. It's just a matter of now, again, studying it in these individual studies and taking the hot lead into a pivotal trial at the end of the day. And we'll take the same approach with other solid tumor indications also, where often the shortest route to the market is in the high unmet medical need, which is typically in a 2nd+ line of therapy as we've done in NSCLC, and we want to continue explore that in other indications as well.
Joe Shan: George, you're right, we did not select based on that [mutational status]. However, I think bavituximab, in theory, could work though even with some of these ultra-targeted molecular drugs. It's just that was not the purpose of this particular study. In the future that's something I think we'll be interested in studying, those combinations as well. As far as differences across different studies, even in our own, Steve already mentioned that every study is a different experiment and they share some similar traits & trial design. But, at the end of the day, you just have to see what the data says. In our frontline study, I think the, surrogate readouts of response rates and PFS weren’t very clear in terms of any difference, but those are surrogates and not direct clinical benefit. So, we are hopeful that we might see something in OS – we’ve not yet reached that point. But, I think that's certainly a possibility and at this point, it’s just [indiscernible].
GZ: On your Imaging Program, I124-PGN650, you're enrolling patients in this trial, could this be also a part of the pivotal Phase III? Do you think you could track tumor response in the Phase III with I124-PGN650?
Steve King: Given the current timetable of the EOP2 meeting and beginning the study, it's just probably not in the cards for the Phase III. Certainly, I think as we think about future development, and I think this is something that also partners like very much, is it [I124-PGN650 Imaging] could be a very valuable tool as we go forward in selecting the right combinations and the right stage of disease, and being able to have, almost like a biomarker, that would allow us to guide the development of the bavituximab program, rather than having to run hundreds of randomized Phase II studies to pick the hot leads. We may be able to get an early read on that through the imaging program and the utilization of that in our bavituximab program in the future. But, as far as being ready for the Phase III, unfortunately, the time line is too tight and that ship is already kind of sailing along.
Joe Shan: And quite frankly, with the survival results we're seeing in "unselected population", there really is not a need to select patients in order to enrich results in the future. That's often a strategy that's not necessary if across-the-board you're not seeing a lot of activity, but maybe in a particular subset, for example, some mutational status - that sort of makes sense. But I think bavituximab is broad enough that's not a requirement. But we are developing an imaging platform, as Steve said, as potentially a tool for selecting different combinations or such.
4. Gregory R. Wade (Wedbush: [ http://www.wedbush.com/services/cmg/equities-division/research ]
GW: Let me add my congratulations on the very strong data set. Joe, with respect to concordance with disease control & response, can you tell us whether you had a chance to interrogate the data to see whether there is some concordance there with Response and OS?
Joe Shan: No, we have not looked at that extensively because again, historically, response rates are a very poor prognosticator for survival. In this case and obviously, we had seen overall across groups, a similar trend of increased response rates in a prolonged PFS, and now, certainly the survival prolongation. The short answer is no, we have not really tried to correlate those 2 because it's not necessarily a shrinking of tumors on radiograph that leads to this. In fact, an interesting point is that there was a comment from the session chair [9-7-12 Gerber/Chicago] about applicability of RECIST-based definitions, and if you evaluate the drugs such as bavituximab, that might have an immune sort of component and that may not be the best way to evaluate. And certainly, again, we are looking at the survival end point as really the one that determines the activity, the meaningful activity, and not merely relying on a surrogate.
GW: And with respect to time to best response, there's been some observations that other immunologically active agents have a much delayed time to best response. Was there any difference in the time to best response in either the control or the bavi arms?
Joe Shan: I don't know the exact results at the moment, but I can say that, by and large, no, there were no differences in when patients responded. Keep in mind, they were only on chemotherapy for up to 6 cycles and that's one of the reasons why, in a study of this design, that you actually cap it, otherwise, there could be imbalances in the number of chemotherapy cycles. [indiscernible] So, for responses, they have to basically achieve them very quickly in the first few cycles.
GW: Lastly, with respect to survival, have you had a chance to review the narratives around death? Do you see any differences in the side of failure or ultimate cause of the demises of the patients between the control and the bavi arms that might be informative as to how the drug is working in the study?
Joe Shan: Sure. No, we haven't done statistical analysis. Certainly, we view all SAEs that result in death - generally, disease progression is the primary cause of death. So, it's an outcome of their disease process and not so much of toxicity or such.
MR. KING’S CLOSING COMMENTS:
I would like to thank everyone, again, for participating today's quarterly conference call. We certainly look forward as we continue to advance the bavituximab program and make other advancements in our overall corporate activities, and look forward to discussing that at our next earnings call in December. Thank you very much.
*end*
.
.
= = = = = = = = = = = = =
Latest 10K 4-30-12 iss. 7-16-12: http://tinyurl.com/79o57b2 PR: http://tinyurl.com/c8nytow (Cash 4-30-12 $18.0mm)
Latest 10Q 7-31-12 iss. 9-10-12: http://tinyurl.com/9sd8nua PR: http://tinyurl.com/9f85fdo (Cash 7-31-12 $19.0mm)
ALL SEC filings for PPHM: http://tinyurl.com/6d4jw8
.
.


• 9-7-12: Press Release about Dr. Gerber's plenary at ASTRO/Thoracic/Chicago: http://tinyurl.com/8oxwk6v - "The interim data showed a statistically significant improvement in OS (Hazard Ratio 0.524, p-value .0154) and a doubling of MOS (12.1/13.1mos. vs. 5.6mos.) in the Bavituximab-containing arms compared to the [Docetaxel] ctl-arm."
• VP Joe Shan's 15min. Webcast & Slideshow recapping Dr. David Gerber's 9-7-12 ASTRO/Chicago Plenary: http://tinyurl.com/8cn87la
8-2012: Compare Bavi+Doce's MOS=13.1mos (Bavi/3mg) to the 4 Curr-Approved 2Line/NSCLC Drugs http://tinyurl.com/cgnkvpa
• Taxotere/docetaxel => MOS=6.3mos (meta-analysis of 5 trials, 865 pts)
• Altima/pemetrexed=> No diff. vs. Docetaxel (Ph.3 non-inferiority vs. Doce, 571 pts)
• Tarceva/erlotinib => MOS=5.3mos (TITAN Ph.III n=424 trial - see http://tinyurl.com/8w8lo93 )
• Iressa (gefitinib )=> "Iressa does not improve OS"
= = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = =
PR 9-10-12: FY’13/Q1 Financials & Devs (q/e 7-31-12)
Peregrine Pharmaceuticals Reports First Quarter Fiscal Year 2013 Financial Results and Recent Developments
• Interim Data Show Doubling of Median Overall Survival in Bavituximab-Treated Patients from Double-Blind, Placebo-Controlled Phase II Trial in 2nd-Line NSCLC
• Recent Data Strongly Support Advancing Bavituximab Program Into Phase III Clinical Development
http://ir.peregrineinc.com/releasedetail.cfm?ReleaseID=705887
TUSTIN, 9/10/2012: Peregrine Pharmaceuticals, Inc. (NASDAQ: PPHM), a biopharmaceutical company developing first-in-class monoclonal antibodies focused on the treatment and diagnosis of cancer, today announced financial results for the first quarter ended July 31, 2012 of fiscal year (FY) 2013 and provided an update on its advancing clinical pipeline and other corporate developments.
"We have achieved major milestones since the end of last quarter with the unblinding of our proof-of-principle bavituximab study in 2nd-Line NSCLC in May and the recent announcement of overall survival data from the study being the most significant. The statistically significant overall survival seen in that study is an obvious green light for us to begin plans to advance the program into Phase III and goes a long way toward validating the technology platform," said Steven W. King, president and CEO of Peregrine. "Following these exciting developments, the upcoming milestones for the program include additional clinical data from 8 ongoing bavituximab clinical trials, an end of Phase II meeting with the FDA expected by year end, and potential partnership as the result of ongoing discussions. This is truly an exciting time at Peregrine and we look forward to advancing the bavituximab program as well as the rest of our business operations."
BAVITUXIMAB ONCOLOGY PROGRAM HIGHLIGHTS
Lead Indication: 2nd-Line NSCLC
Last week, in a late-breaker, oral plenary presentation at the 2012 Chicago Multidisciplinary Symposium in Thoracic Oncology meeting, interim data was presented [ 9-7-12: http://tinyurl.com/8oxwk6v ] from a randomized, double-blind, placebo-controlled Phase IIb trial evaluating two dose levels of bavituximab (bavituximab-containing arms) plus docetaxel versus docetaxel plus placebo (control arm) in 2nd-Line Stage IIIb/IV NSCLC (NSCLC). This trial enrolled 121 patients with 2nd-Line Stage IIIb or Stage IV non-squamous NSCLC following one prior chemotherapy regimen and patients were equally randomized to 1 of the 3 treatment arms, with 117 of the enrolled patients being evaluable per the clinical protocol. Patients received up to 6 cycles of docetaxel (75mg/m2) plus either placebo, 1 mg/kg bavituximab, or 3 mg/kg bavituximab until disease progression. Recent data from the trial showed a doubling of median overall survival (OS) in both bavituximab-containing arms compared to the control arm and a statistically significant improvement in overall survival. In addition, bavituximab continues to be well-tolerated. Given the magnitude of this data, Peregrine is preparing for an End-of-Phase II meeting with the U.S. Food and Drug Administration (FDA) by the end of calendar year 2012 that should allow us to initiate Phase III by mid-2013.
"The unique immune directed attack of bavituximab and preliminary survival advantage of far greater magnitude than what has been observed historically with anti-angiogenesis agents provide potentially yet another example of clinically relevant immune directed therapy moving forward," said John Nemunaitis, M.D., executive director of the Mary Crowley Cancer Research Centers and an investigator in Peregrine's Phase II bavituximab 2nd-Line NSCLC clinical trial.
Additional Bavituximab Clinical Trials
Peregrine currently has 7 additional ongoing clinical trials as follows:
• A randomized, open-label, Phase II clinical trial evaluating bavituximab plus carboplatin and paclitaxel versus carboplatin and paclitaxel alone in 83 evaluable patients with previously untreated [Front-Line] Stage IIIb or Stage IV NSCLC patients completed enrollment in September of 2011 and the event-driven median overall survival data will be available upon maturation.
• A randomized, open-label, Phase II clinical trial evaluating bavituximab plus gemcitabine versus gemcitabine alone in 70 patients with previously untreated [Front-Line] Stage IV Pancreatic Cancer completed enrollment in June 2012. The primary endpoint, median OS, is an event-driven endpoint and will be reported once reached.
• Phase I/II Investigator Sponsored Trial (IST) investigating bavituximab in combination with sorafenib in patients with Advanced Hepatocellular Carcinoma (Liver Cancer). The Phase I portion of the trial has completed patient enrollment.
• A Phase I/II IST evaluating bavituximab in combination with cabazitaxel in patients with 2nd-Line Castration-Resistant Prostate Cancer [CRPC].
• A Phase Ib IST evaluating bavituximab in combination with carboplatin and pemetrexed in patients with previously untreated [Front-Line] Stage IV NSCLC.
• A Phase I IST evaluating bavituximab in combination with paclitaxel in up to 14 patients with HER2-negative Metastatic Breast Cancer.
• A Phase I IST evaluating bavituximab in combination with capecitabine and radiation therapy in patients with Stage II or III Rectal Adenocarcinoma.
COTARA PROGRAM HIGHLIGHTS
Peregrine's single-administration approach to treating recurrent glioblastoma multiforme (GBM) has shown encouraging 9.3 month median overall survival data from a Phase II trial in 41 patients. Peregrine and the FDA continue to advance discussions surrounding the negotiation of a pivotal trial design. The company plans to seek partners both in the U.S. and internationally to support the development of Cotara for this deadly form of brain cancer.
IMAGING PROGRAM HIGHLIGHTS
PS-Targeting Molecular Imaging Program
In April 2012, Peregrine launched its experimental phosphatidylserine (PS)-targeting molecular imaging candidate, 124I-PGN650, into clinical development for the imaging of multiple solid tumor types. The primary goal of the trial [ http://clinicaltrials.gov/ct2/show/NCT01632696 ] is to estimate radiation dosimetry in critical and non-critical organs. Secondary objectives of the trial are tumor imaging and safety. Patients are currently being enrolled in the trial.
FINANCIAL RESULTS
Total revenues for the first quarter of FY 2013 were $4,251,000, compared to $5,655,000 for the same quarter of the prior fiscal year. This decrease was primarily attributable to lower contract manufacturing revenue generated by Peregrine's biomanufacturing subsidiary Avid Bioservices, which generated contract manufacturing revenue of $4,135,000 for the first quarter of FY 2013, compared to $5,439,000 for the same quarter of the prior fiscal year. The decrease in contract manufacturing revenue was primarily due to a decrease in the number of completed manufacturing runs released and shipped during the current quarter, which can be attributed to the timing of services provided to Avid's third-party clients. However, based on current manufacturing commitments from Avid's third-party clients for services to be provided during the remainder of FY 2013, we expect contract manufacturing revenue to be at least $15 million for FY 2013. In addition, Avid will continue to utilize available capacity and resources to continue its preparation for later stage clinical development and potential commercialization of bavituximab and Cotara, while also seeking to grow its services from third-party clients.
Total costs and expenses decreased $1,784,000 to $11,922,000 in the first quarter of FY 2013 from $13,706,000 in the first quarter of FY 2012. This decrease was primarily attributable to lower contract manufacturing costs incurred by Avid combined with lower research and development expenses associated with lower clinical trial costs. For the first quarter of FY 2013, cost of contract manufacturing and R&D expenses were $2,024,000 and $6,981,000, respectively, compared to $3,017,000 and $7,760,000, respectively, for the first quarter of FY 2012. Selling, general and administrative expenses for the first quarter of FY 2013 were $2,917,000 and were in-line with the first quarter of FY 2012.
Peregrine's consolidated net loss was $7,664,000, or $0.07 per basic and diluted share, for the first quarter of FY 2013, compared to a net loss of $8,092,000, or $0.11 per basic and diluted share, for the same quarter of the prior year.
Peregrine reported $18,991,000 in cash and cash equivalents at July 31, 2012, compared to $18,033,000 at April 30, 2012. Subsequent to July 31, 2012, Peregrine announced that it had secured a $30 million term loan from Oxford Finance, MidCap Financial, and Silicon Valley Bank. Under the loan agreement, the company received initial funding of $15 million upon closing on August 30, 2012, and has an option to receive an additional $15 million, provided, on or before March 31, 2013, Peregrine meets certain predefined milestones, as described in loan agreement.
More detailed financial information and analysis may be found in Peregrine's Quarterly Report on Form 10-Q, which will be filed with the Securities and Exchange Commission today. [10-Q 7-31-12 iss. 9-10-12: http://tinyurl.com/9sd8nua ]
Conference Call
Peregrine will host a conference call and webcast this morning, September 10, 2012, at 11:00 AM ET (8:00 AM PDT). To listen to the conference call, please dial (877) 312-5443 or (253) 237-1126 and request the Peregrine Pharmaceuticals conference call. A replay of the call will be available starting approximately two hours after the conclusion of the call through Sept. 24, 2012 by calling (855) 859-2056, or (404) 537-3406 and using passcode 27367274 . To listen to the live webcast, or access the archived webcast, please visit: http://ir.peregrineinc.com/events.cfm
ABOUT PEREGRINE PHARMACEUTICALS, INC.
Peregrine Pharmaceuticals, Inc. is a biopharmaceutical company with a portfolio of innovative monoclonal antibodies in clinical trials focused on the treatment and diagnosis of cancer. The company is pursuing multiple clinical programs in cancer with its lead product candidate bavituximab and novel brain cancer agent Cotara®. Peregrine also has in-house cGMP manufacturing capabilities through its wholly-owned subsidiary Avid Bioservices, Inc. ( http://www.avidbio.com ), which provides development and biomanufacturing services for both Peregrine and outside customers. Additional information about Peregrine can be found at http://www.peregrineinc.com .
Safe Harbor *snip*
PEREGRINE PHARMACEUTICALS, INC.
CONDENSED CONSOLIDATED STATEMENTS OF OPERATIONS AND COMPREHENSIVE LOSS
THREE MONTHS ENDED
----------------------------
July 31, 2012 July 31, 2011
------------- -------------
Unaudited Unaudited
REVENUES:
Contract manufacturing revenue $ 4,135,000 $ 5,439,000
License revenue 116,000 216,000
------------- -------------
Total revenues 4,251,000 5,655,000
COSTS AND EXPENSES:
Cost of contract manufacturing 2,024,000 3,017,000
Research and development 6,981,000 7,760,000
Selling, general and administrative 2,917,000 2,929,000
------------- -------------
Total costs and expenses 11,922,000 13,706,000
------------- -------------
LOSS FROM OPERATIONS (7,671,000) (8,051,000)
------------- -------------
OTHER INCOME (EXPENSE):
Interest and other income 8,000 13,000
Interest and other expense (1,000) (54,000)
------------- -------------
NET LOSS $ (7,664,000) $ (8,092,000)
============= =============
WEIGHTED AVERAGE COMMON SHARES OUTSTANDING
Basic and diluted 103,283,937 70,656,568
============= =============
BASIC AND DILUTED LOSS PER COMMON SHARE $ (0.07) $ (0.11)
============= =============
COMPREHENSIVE LOSS $ (7,664,000) $ (8,092,000)
============= =============
PEREGRINE PHARMACEUTICALS, INC.
CONDENSED CONSOLIDATED BALANCE SHEETS
JULY 31, APRIL 30,
2012 2012
------------- -------------
Unaudited
ASSETS
CURRENT ASSETS:
Cash and cash equivalents $ 18,991,000 $ 18,033,000
Trade and other receivables, net 2,271,000 2,353,000
Inventories, net 5,744,000 3,611,000
Prepaid expenses and other current assets,
net 887,000 795,000
------------- -------------
Total current assets 27,893,000 24,792,000
Property, net 2,868,000 2,900,000
Other assets 745,000 570,000
------------- -------------
TOTAL ASSETS $ 31,506,000 $ 28,262,000
============= =============
LIABILITIES AND STOCKHOLDERS' EQUITY
CURRENT LIABILITIES:
Accounts payable $ 4,151,000 $ 3,492,000
Accrued clinical trial and related fees 1,909,000 2,111,000
Accrued payroll and related costs 2,908,000 2,468,000
Deferred revenue 6,056,000 3,651,000
Customer deposits 10,224,000 4,865,000
Other current liabilities 1,308,000 1,052,000
------------- -------------
Total current liabilities 26,556,000 17,639,000
Deferred revenue 284,000 361,000
Other long-term liabilities 742,000 779,000
Commitments and contingencies
STOCKHOLDERS' EQUITY:
Preferred stock-$0.001 par value; authorized
5,000,000 shares; non-voting; nil shares
outstanding - -
Common stock-$0.001 par value; authorized
325,000,000 shares; outstanding - 104,178,431
and 101,421,365, respectively 104,000 101,000
Additional paid-in capital 349,608,000 347,506,000
Accumulated deficit (345,788,000) (338,124,000)
------------- -------------
Total stockholders' equity 3,924,000 9,483,000
------------- -------------
TOTAL LIABILITIES AND STOCKHOLDERS' EQUITY $ 31,506,000 $ 28,262,000
============= =============
Contact: Christopher Keenan or Jay Carlson
Peregrine Pharmaceuticals, Inc., (800) 987-8256, info@peregrineinc.com
= = = = = = = = = = = = =
Latest 10K 4-30-12 iss. 7-16-12: http://tinyurl.com/79o57b2 PR: http://tinyurl.com/c8nytow (Cash 4-30-12 $18.0mm)
Latest 10Q 7-31-12 iss. 9-10-12: http://tinyurl.com/9sd8nua PR: tp://tinyurl.com/9f85fdo (Cash 7-31-12 $19.0mm)
ALL SEC filings for PPHM: http://tinyurl.com/6d4jw8


