 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.





cjgaddy
![]()
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Looks like a bunch of Robot Gibberish from 6-8 years ago, Hutschi. The Robot "posted" it on "3-30-17" - nothing to do with how old it is. I dislike junk like that just like the 20-30 Daily Robot, boiler-plate injected, "Financial Stock Articles" that show up each day on the Internet for Peregrine, and for every other stock under the sun.
Interesting Sloan Kettering Tweet today re: AACR’17
3-31-17 9:20amET “Getting ready for #AACR17? #Immunotherapy will be a hot topic. Learn more about how it works (video). @AACR”
https://twitter.com/sloan_kettering
Points to this 4-2016 Video (1:20):
“Immunotherapy – How It Works” https://www.youtube.com/watch?v=COQ1AeoGyco
Beg@:39:
“Immunotherapy drugs release this brake and empower immune cells to fight the cancer.
Sometimes the immune system needs a tune-up before it can fight cancer.
Immune cells can be removed from the body, armed with new proteins that can target cancer cells, and given back to a patient in large numbers.
Once inside the body, the modified immune cells recognize and attack the cancer.
This approach is called CAR T cell therapy. [an Adoptive Cell Transfer “ACT” strategy]
Despite the promise of immunotherapy, not everybody responds.
MSKCC scientists are exploring ways to improve immunotherapy.”
-------
All about CAR T Cell Therapy (an Adoptive Cell Transfer “ACT” strategy):
“Adoptive cell transfer is like ‘giving patients a living drug’,” states Renier J. Brentjens, MD/PhD, of Memorial Sloan Kettering Cancer Center (MSKCC).
https://www.cancer.gov/about-cancer/treatment/research/car-t-cells
“Adoptive T cell therapy (ACT) is one stone in this new pillar, a potentially powerful approach to cancer treatment that relies on the infusion of tumor-specific T cells.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4327320

=============AS WELL AS THIS 3-23-17 PARKER FOUNDATION RELEASE ON AACR’17:
3-23-17: “Parker Institute for Cancer Immunotherapy Scientists to Present Research on Checkpoint Inhibitors, Adoptive Cell Therapy, and Other Advances in Immuno-oncology at AACR 2017”
Investigators affiliated with the Parker Institute for Cancer Immunotherapy will present some of the most anticipated immuno-oncology research at the 2017 AACR Annual Meeting. The event takes place at the Walter E. Washington Convention Center in Washington, DC, April 1-5 2017. . .
Other adoptive cell therapy abstracts of interest:
• ”Targeting Phosphatidylserine in Combination with Adoptive T Cell Transfer Eliminates Advanced Tumors without Off-Target Toxicities in a Melanoma Preclinical Model” [see http://tinyurl.com/nx5q5os ]
The principal investigator is Taha Merghoub, PhD, Parker Institute member researcher at Memorial Sloan Kettering Cancer Center. Co-authors include Parker Institute Center Director Jedd Wolchok, MD, PhD, at Memorial Sloan Kettering Cancer Center.
http://www.parkerici.org/media/2017/parker-institute-for-cancer-immunotherapy-scientists-to-present-research-on
Now, we have Dr. Wolchok’s Lab and PPHM presenting the following poster at AACR’17:
Apr1-5 2017: “AACR 2017”, WashDC - See http://tinyurl.com/mxz23gz http://www.aacr.org/Meetings/Pages/MeetingDetail.aspx?EventItemID=105
2. 4-3-17/8am #1651 - Session: TUMOR MICROENVIRONMENT & CHECKPOINTS
“Targeting Phosphatidylserine in Combination with Adoptive T Cell Transfer Eliminates Advanced Tumors without Off-Target Toxicities in a Melanoma Preclinical Model” <=NEW(2nd) MSK STUDY
…...See: More on the Significance of the New MSK/Wolchok+PPHM “ACT” study: http://tinyurl.com/mkn6cvt
=> Daniel Hirschhorn-Cymerman 1, Sara Sara Schad 1, Sadna Budhu 1, Zhong Hong 1, Xia Yang 1, Hutchins T. Jeff 2, Bruce D. Freimark 2, Michael J. Gray 2, Jedd Wolchok 1, Taha Merghoub [Memorial Sloan Kettering]
1=Memorial Sloan Kettering CC, NYC [ http://www.mskcc.org/research-areas/labs/jedd-wolchok ]
2=Peregrine Pharmaceuticals
ABSTRACT:
A viable strategy to treat advanced cancers includes transferring of tumor-specific T cells. T cells that recognize tumor antigens can be expanded and reinvigorated ex-vivo. Furthermore, autologous T cells can be genetically modified to express anti-tumor T cell receptors or chimeric antigen receptors. Although the potency and specificity of tumor-specific T cells can be manipulated ex-vivo, once re-infused into patients, the T cells are subjected to immunosuppressive mechanisms established by the tumor. An important immune checkpoint regulator within tumors is phosphatidylserine (PS). Innate immune cells exposed to PS secrete suppressive cytokines and chemokines that can significantly impair the function and activation of anti-tumor T cells. Therefore, monoclonal antibodies that block PS activity can increase the anti-tumor potency of transferred T cells to treat aggressive cancers. Here we show that a PS targeting monoclonal antibody in combination with CD4+ T cells that recognize the melanoma antigen Trp1 can regress very advanced melanomas in all treated mice. Combination of anti-Trp1 CD4+ T cells with other immunomodulatory modalities such as anti-OX40 antibodies, can achieve equivalent treatment rates but these are typically accompanied by severe immune related adverse events. In contrast, in this setting, PS blockade did not show any off-target toxicities. Flow cytometry analysis revealed lower levels of CD206 expression concomitant with higher activation markers in macrophages and neutrophils in tumors from anti-PS treated mice. These results suggest that diminishing suppressive mechanisms locally in adoptive transfer protocols is a highly desirable strategy that can eliminate tumors while minimizing related adverse events.
AND MESH THAT WITH THIS ABOUT THE TOTALITY OF DR. WOLCHOK’s AACR’17 AGENDA:
INTERESTING: Mem. Sloan’s Dr. Jedd. Wolchok is co-author of 9 AACR’17 abstracts. 2 of the 9 are w/PPHM re: PS-Targeting. With biotechs, he has one each with Genocea Biosciences(ex-vivo screening), Infinity Pharm(Ph1), Leap Ther.(Ph1), and two with BMS(Ph1+Ph3). The 8th is MSKCC ONLY, and the 9th is jointly w/Cedars-Sinai/LA. http://www.abstractsonline.com/pp8/#!/4292 .
PEREGRINE (Joint Mem.Sloan Kettering Wolchok Lab & PPHM):
1. 4-2-17 #574 “Phosphatidylserine Targeting Antibody in Combination with Tumor Radiation & Immune Checkpoint Blockade Promotes Anti-Tumor Activity in Mouse B16 Melanoma” <=Same as SITC’16 11-14-16.
2. 4-3-17 #1651 “Targeting Phosphatidylserine in Combination With Adoptive T Cell Transfer Eliminates Advanced Tumors Without Off-Target Toxicities in a Melanoma Preclin. Model” <=NEW/2nd PPHM+MSK.
NON-PEREGRINE:
3. (MSK ONLY): 4-2-17 #874 “Lifting the iron curtain: Imaging cellular barriers to combination chelation-immune checkpoint therapy”
4. (MSK & Genocea Bio. http://www.genocea.com GNCA/$130mm MktCap) 4-2-17 #632 “Genome-scale neoantigen screening using ATLAS prioritizes candidate antigens for immunotherapy in a NSCLC patient”
5. (MSK & Cedars-Sinai/LA) 4-4-17 #4705 “CTLA4 blockade with HER2-directed therapy yields clinical benefit in women undergoing radiation therapy for HER2+ breast cancer brain metastases”
6. (MSK & Infinity Pharm.) 4-4-17 #CT089 “A Ph1, first-in-human study of IPI-549, a PI3K-y inhibitor, as monotherapy & in combo w/nivolumab in adv. solid tumors”
7. (MSK & Leap Ther.) 4-2-17 #CT018 “Intratumor & peripheral Treg modulation as a pharmacodynamic biomarker of the GITR agonist antibody TRX-518 in the 1st in-human trial”
8. (MSK & BMS) 4-3-17 #CT073 “(Ph1) Immunomodulatory effects of NIVO+IPI or NIVO/mono in adv. melanoma: CheckMate038”
9. (MSK & BMS) 4-3-17 #CT075 “OS results from a Ph3 of NIVO+IPI in treatment-naïve pts w/adv. Melanoma: CheckMate067”

----------ACT NOTES:
NOTE1:
From 3-2014 Immunotherapy article: “Cancer immunotherapy, particularly adoptive cell transfer (ACT), has shown great promise in the treatment of patients with late-stage disease, including those who are refractory to std. Therapies” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4372895
NOTE2:
The Parker Foundation: “The Immunotherapy Dream Team”
Through the support from SEAN PARKER, Stand Up To Cancer (SU2C) and the Cancer Research Institute (CRI) formed an Immunology Research Dream Team dedicated to cancer immunology: “Immunologic Checkpoint Blockade & Adoptive Cell Transfer in Cancer Therapy.” The Immunotherapy Dream Team is focused on 2 approaches for this translational cancer research project, which will unite laboratory & clinical efforts towards the immunological treatment, control, and prevention of cancer.
The 1st is investigating blockades (by inhibitory molecules called “checkpoints”) of T lymphocytes’ inhibitory receptors, which block immune responses; and the use of antibodies to remove the checkpoints, once again allowing white blood cells called T lymphocytes to kill the cancer cells.
Second, the Immunotherapy Dream Team is pursuing multiple Adoptive Cell Transfer (ACT) approaches, which increase immunity.”
DREAM TEAM LEADERSHIP: 10 scientists, incl. MSKCC’s Jedd D. Wolchok & Michel Sadelain.
http://parker.org/initiatives/immunotherapy
The Parker Foundation: “The Immunotherapy Dream Team”
Through the support from SEAN PARKER, Stand Up To Cancer (SU2C) and the Cancer Research Institute (CRI) formed an Immunology Research Dream Team dedicated to cancer immunology: “Immunologic Checkpoint Blockade & Adoptive Cell Transfer in Cancer Therapy.” The Immunotherapy Dream Team is focused on 2 approaches for this translational cancer research project, which will unite laboratory & clinical efforts towards the immunological treatment, control, and prevention of cancer.
The 1st is investigating blockades (by inhibitory molecules called “checkpoints”) of T lymphocytes’ inhibitory receptors, which block immune responses; and the use of antibodies to remove the checkpoints, once again allowing white blood cells called T lymphocytes to kill the cancer cells.
Second, the Immunotherapy Dream Team is pursuing multiple Adoptive Cell Transfer (ACT) approaches, which increase immunity.”
DREAM TEAM LEADERSHIP: 10 scientists, incl. MSKCC’s Jedd D. Wolchok & Michel Sadelain.
http://parker.org/initiatives/immunotherapy
= = = = = = =
3-23-17: “Parker Institute for Cancer Immunotherapy Scientists to Present Research on Checkpoint Inhibitors, Adoptive Cell Therapy, and Other Advances in Immuno-oncology at AACR 2017”
Investigators affiliated with the Parker Institute for Cancer Immunotherapy will present some of the most anticipated immuno-oncology research at the 2017 AACR Annual Meeting. The event takes place at the Walter E. Washington Convention Center in Washington, DC, April 1-5-2017. . .
Other adoptive cell therapy abstracts of interest:
• ”Targeting Phosphatidylserine in Combination with Adoptive T Cell Transfer Eliminates Advanced Tumors without Off-Target Toxicities in a Melanoma Preclinical Model” [see http://tinyurl.com/nx5q5os ]
The principal investigator is Taha Merghoub, PhD, Parker Institute member researcher at Memorial Sloan Kettering Cancer Center. Co-authors include Parker Institute Center Director Jedd Wolchok, MD, PhD, at Memorial Sloan Kettering Cancer Center.
http://www.parkerici.org/media/2017/parker-institute-for-cancer-immunotherapy-scientists-to-present-research-on
1st NCCN Trial(Moffitt/Liver) Recruiting a/o 3-27-17. Thx for the find, BB...
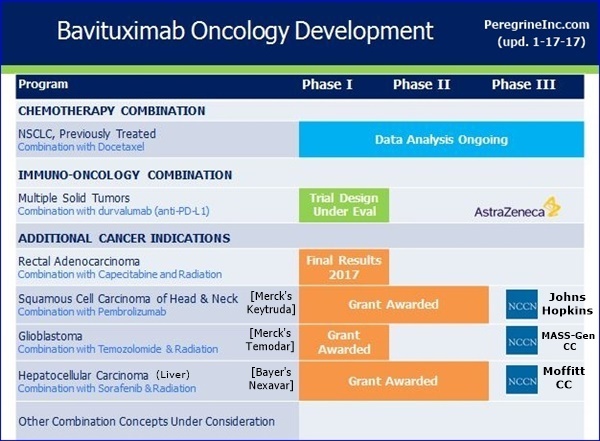
NCCN Bavituximab Trials Announced 9-6-16 - To Begin "Early 2017" http://tinyurl.com/gutgwb5
...#1: Ph1/HepC-Related Hepatocellular(Liver) (Bavi+RAD+Sorafenib), MOFFITT CANCER CENTER - PI: Jessica Frakes, MD
. . . . . . .https://clinicaltrials.gov/ct2/show/NCT02989870 <=Recruiting a/o 3-27-17
...#2: P1-2/Newly Diag. Glioblastoma (Bavi+RAD+Merck’s Temodar), MASS-GEN. CANCER CENTER - PI: Elizabeth Gerstner, MD
...#3: Ph2/Progressive Squamous Head+Neck (Bavi+Merck’s Keytruda), JOHNS-HOPKINS(Sidney Kimmel CC) - PI: Ranee Mehra, MD
3-13-17/CC JOE SHAN (VP/Clin.&Reg. Affairs) http://tinyurl.com/grhwjvy
“…Now turning to new trials, I’m happy to report that the 3 clinical trials to be funded through our collaboration with the NCCN are advancing as expected. The first study, expected to begin patient enrollment shortly, is being conducted by Dr. Jessica Frakes, at the Moffitt Cancer Center. This study, which builds upon a prior investigator sponsor trial [3-25-15/Dr. Adam. Yopp(UTSW) http://tinyurl.com/opkh5qy ], will evaluate the combination of Stereotactic Body Radiation Therapy, sorafenib, and bavituximab, for the treatment of Unresectable Hepatocellular [Liver] Carcinoma. We are interested in this trial design as radiation has been shown to increased PS expression on the surface of tumor cells, induce immunogenic tumor cell depth, and increase tumor specific T-cell activity. In addition, NCCN has recently communicated that both the study of bavituximab, temozolomide, and radiation in newly diagnosed Glioblastoma and the trial of bavituximab & temozolomide in recurrent Head & Neck cancer, which has progressed on checkpoint inhibitor treatment, are on track to be initiated by mid-year."
= = = = = = = = = = = = = = = = = =
9-6-16: NCCN to Initiate 3 Bavi-Trials Early’17 (Moffitt,MassGEN,JohnsHopkins) http://tinyurl.com/gutgwb5
=> Ph1/HepC-Related-Hepatocellular/MOFFITT, Ph1-2/Glioblastoma/MASS-GEN, Ph2/Head+Neck/JOHNS-HOPKINS
NCCN PR: https://www.nccn.org/about/news/newsinfo.aspx?NewsID=785
”NCCN is excited to initiate 3 studies by accomplished investigators at Member Institutions that will explore the effect of this novel immunotherapy in 3 different cancers with significant unmet need,” said Robert C. Young, MD, Interim VP, NCCN ORP.
I found the 9-26-16 Birge+PPHM Abstract here:
http://cancerimmunolres.aacrjournals.org/content/4/11_Supplement/B119
Sept25-28 2016: “2nd CRI-AACR-CIMT-EATI Intl. Cancer Immunotherapy Conf.”, NYC
9-26-16: #B119 “Characterization of a Phosphatidylserine, TAM Receptor (Tyro3, Axl, Mertk), PDL1 Axis in Breast Cancer”
Canan Kasikara 1, Sushil Kumar 1, Ke Geng 1, Viral Davre 1, Cyril Empig 2, Bruce Freimark 2, Michael Gray 2, Kyle Schlunegger 2, Jeff Hutchins 2, Sergei V. Kotenko 1, Raymond B. Birge 1
1=Rutgers, New Jersey Medical School, Newark, NJ
2=Peregrine Pharmaceuticals, Tustin
ABSTRACT:
Tyro3, Axl, and Mer (TAMs) are 3 homologous receptor tyrosine kinases that bind vitamin K-dependent endogenous ligands, Protein S (PROS1) and Gas6, and act as bridging molecules to promote PS-mediated clearance of apoptotic cells (efferocytosis). In recent years, evidence has accumulated that TAMs are overexpressed in a wide array of tumor types, whereby the level of expression correlates with the tumor grade and the emergence of chemo and radio resistance to targeted therapeutics. TAMs have also been implicated as inhibitory receptors on myeloid-derived cells that suppress anti-tumor immunity. In addition to TAM overexpression, externalized PS is also concomitantly up-regulated in the tumor microenvironment, suggesting that PS & PS receptors might act as immune checkpoint inhibitors. To better understand the biology of TAMs, and the specificity of interaction between TAMs & PS, we generated chimeric TAM reporter cell lines comprised of the extracellular domains of each TAM fused to the intracellular domains of the IFNR1, as well as cell lines stably expressing full-length native TAMs. Using these systems, we found that each TAM receptor has a unique pattern of activation by GAS6 and PROS1, as well as unique dependency for PS on apoptotic cells, PS liposomes, and exosomes. Interrogating epithelial cells that express WT TAMs, we also observed that each TAM showed differential capacity for efferocytosis, AKT-mediated chemo-resistance, and their ability to up-regulate the immune checkpoint inhibitory ligand PD-L1 on breast cancer cells. Functionally, TAM-mediated efferocytosis and PD-L1 up-regulation could be partially blocked by PS targeted antibodies 11.31 & bavituximab, suggesting the existence of a PS/PS-R (TAM-receptor)/PD-L1 axis that drives immune escape in solid cancers. These studies demonstrate that, despite their similarities, Tyro3, Axl, and Mertk are likely to perform distinct functions in both immune-regulation and the recognition and removal of apoptotic cells. Finally, these studies provide a rationale for combinatorial therapeutics targeting PS, TAM, and PD-L1 as immune checkpoint inhibitors in the treatment of cancer.
Rutgers’ Dr. Raymond Birge+Peregrine 9-26-16 AACR-CRI/NYC Poster, “Characterization of a PS, TAM Receptor (Tyro3, Axl, Mertk), PDL1 Axis in Breast Cancer”. That would be interesting to see the full article, Cheynew.
On 9-26-16, Rutgers’ Dr. Raymond Birge w/Peregrine co-authors, AACR-CRI/Sept26/NYC Poster. This involves Peregrine’s “preclinical I-O focused internal efforts”, which Jeff Hutchins (VP/PreClin.Res) described in the 9-8-16 CC as, “advancing well, and we have seen impressive signs of activity with new combinations of PS targeting and other treatment modalities such as checkpoint blockers, T-cell agonists and radiation.” - see Dr. Hutchin’s 9-8-16 comments below. Note that Dr. Birge is the Senior Author of B119.
= = = = = = = = = =
Sept25-28 2016: “2nd CRI-AACR-CIMT-EATI Intl. Cancer Immunotherapy Conf.”, NYC
“The pgm will focus on “Translating Science into Survival” and feature talks from more than 60 leaders in the field covering all areas of inquiry in cancer immunology and immunotherapy.”
http://www.aacr.org/Meetings/Pages/MeetingDetail.aspx?EventItemID=101
ABSTRACTS: http://www.cancerimmunotherapyconference.org/abstracts
9-26-16 5:15-7:45pm: Poster Session B
-----
Track: NEW AGENTS AND THEIR MODE OF ACTION IN ANIMALS AND HUMANS
I. #B019 “LAG3 is an Immunotherapeutic Target in Murine Triple- Breast Cancers, Whose Activity is Significantly Enhanced in Combination with Phosphatidylserine Targeting Antibodies”
Michael J. Gray, Jian Gong, Jeff Hutchins, Bruce Freimark (Peregrine Pharmaceuticals, Dir.Res/Preclin.Oncology)
-----
Track: MECHANISTIC MERGING OF TREATMENT MODALITIES
II. #B119 “Characterization of a Phosphatidylserine, TAM Receptor (Tyro3, Axl, Mertk), PDL1 Axis in Breast Cancer”
Canan Kasikara 1, Sushil Kumar 1, Ke Geng 1, Viral Davre 1, Cyril Empig 2, Bruce Freimark 2, Michael Gray 2, Kyle Schlunegger 2, Jeff Hutchins 2, Sergei V. Kotenko 1, Raymond B. Birge 1
1=Rutgers, New Jersey Medical School, Newark, NJ
2=Peregrine Pharmaceuticals, Tustin
#B119 ABSTRACT 9-26-16:
http://cancerimmunolres.aacrjournals.org/content/4/11_Supplement/B119
Tyro3, Axl, and Mer (TAMs) are 3 homologous receptor tyrosine kinases that bind vitamin K-dependent endogenous ligands, Protein S (PROS1) and Gas6, and act as bridging molecules to promote PS-mediated clearance of apoptotic cells (efferocytosis). In recent years, evidence has accumulated that TAMs are overexpressed in a wide array of tumor types, whereby the level of expression correlates with the tumor grade and the emergence of chemo and radio resistance to targeted therapeutics. TAMs have also been implicated as inhibitory receptors on myeloid-derived cells that suppress anti-tumor immunity. In addition to TAM overexpression, externalized PS is also concomitantly up-regulated in the tumor microenvironment, suggesting that PS & PS receptors might act as immune checkpoint inhibitors. To better understand the biology of TAMs, and the specificity of interaction between TAMs & PS, we generated chimeric TAM reporter cell lines comprised of the extracellular domains of each TAM fused to the intracellular domains of the IFNR1, as well as cell lines stably expressing full-length native TAMs. Using these systems, we found that each TAM receptor has a unique pattern of activation by GAS6 and PROS1, as well as unique dependency for PS on apoptotic cells, PS liposomes, and exosomes. Interrogating epithelial cells that express WT TAMs, we also observed that each TAM showed differential capacity for efferocytosis, AKT-mediated chemo-resistance, and their ability to up-regulate the immune checkpoint inhibitory ligand PD-L1 on breast cancer cells. Functionally, TAM-mediated efferocytosis and PD-L1 up-regulation could be partially blocked by PS targeted antibodies 11.31 & bavituximab, suggesting the existence of a PS/PS-R (TAM-receptor)/PD-L1 axis that drives immune escape in solid cancers. These studies demonstrate that, despite their similarities, Tyro3, Axl, and Mertk are likely to perform distinct functions in both immune-regulation and the recognition and removal of apoptotic cells. Finally, these studies provide a rationale for combinatorial therapeutics targeting PS, TAM, and PD-L1 as immune checkpoint inhibitors in the treatment of cancer.
- - - - -
9-8-16 CC/Jeff Hutchins: “I would now like to provide an update on Peregrine's preclinical I-O focused internal efforts and our collaboration with Memorial Sloan Kettering CC. The goal of this work is to evaluate combinations of PS targeting with other checkpoint inhibitors and immune stimulatory agents for the purpose of developing new and increasingly effective anticancer treatments. These programs are advancing well and to-date, we have seen impressive signs of activity with new combinations of PS targeting and other treatment modalities such as checkpoint blockers, T-cell agonists and radiation. These new combinations are improving overall survival accompanied with increases in cyto-reactive T cells into the tumor tissue. This exciting new internal work will be presented at the CRI/AACR Immunotherapy Meeting in NY later this month and at ESMO in early October. We expect the first results from our collaboration with the Wolchok Lab investigators to be presented at SITC in November and we will provide more detailed information as that presentation becomes available.” http://tinyurl.com/jydtkoy
= = = = = = =
2-2016: Rutgers' Dr. Raymond Birge's relationship with Peregrine & UTSW's Dr. Rolf Brekken and his 2-26-16 article, “Phosphatidylserine is a Global Immunosuppressive Signal in Efferocytosis, Infectious Disease, and Cancer” http://tinyurl.com/z5d9qt9 poster B019, “LAG3 is an Immunotherapeutic Target in Murine Triple- Breast Cancers, Whose Activity is Significantly Enhanced in Combo with PS-Targeting Antibodies”
11-9-15 SITC'15: New Bavi+Checkpoint Inhibitors preclin. data (UTSW/DUKE's Herbert K. Lyerly) http://tinyurl.com/pbof95w
...Also, collab. with Dr. Bernard Fox (Immunotherapist/Earle A. Chiles Res.Inst.) on new Immuno-Profiling Clinical Test (Opal 6-plex quantitative IF Assay), PPHM roundtable with Raymond Birge (Rutgers), Douglas Graham (Emory), Dmitry Gabrilovich (Wistar), Rolf Brekken (UTSW), Maria Karasarides (AstraZeneca) - ”Combining Bavi w/anti-PD-1 significantly enhanced O/S… significant incr. CD45+, CD8+ and CD3+ T-cells… led a prolonged anti-tumor immune response which protected the animals against a re-challenge w/same tumor.”
= = = = = = = =DR. BIRGE:
...Dr. Raymond Birge has authored ~85 scientific publications in molecular & cancer biology. http://www.ncbi.nlm.nih.gov/pubmed/?term=birge+rb
“The Birge laboratory conducts basic science focused on the eradication of cancer.”
http://birgelab.org => http://birgelab.org/biography.html
Ahhhhh, ImmunoVaccine & Jedd Wolchok – zero doubt IMO how & why PPHM & Immunovaccine have hooked up...
ImmunoVaccine & Jedd Wolchok go back to ASCO’13:
6-3-13: “Our poster (Ph1 data) is one of few selected for detailed discussion at ASCO by Dr. Jedd Wolchok, top cancer immunotherapy thought leader… Immunovaccine Inc. believes that these immune responses are consistent in profile to those necessary from a cancer vaccine to potentially impact disease progression. These study results were further discussed by Dr. Jedd Wolchok of Memorial Sloan-Kettering CC, a top thought leader in the area of cancer immunotherapy, at the poster discussion session that followed.”
https://www.imvaccine.com/communications.php?communications_id=11
SEE: The 4-4-17 AACR’17 PPHM+ImmunoVaccine DepoVax+Bavi poster #3657.
”PS Targeting Enhances Anti-Tumor Activity of a Tumor Vaccine(DepoVax), HPV-Induced Tumor”
http://investorshub.advfn.com/boards/read_msg.aspx?message_id=129835637
The 4-4-17 AACR’17 PPHM+ImmunoVaccine DepoVax+Bavi poster #3657. Also, Peregrine Exhibiting, booth #3312.
4. 4-4-17/8am #3657 - Session: BITES BISPECIFICS & CHECKPOINTS
”Phosphatidylserine-Targeting Antibodies Enhance Anti-Tumor Activity of a Tumor Vaccine in a HPV-Induced Tumor Model”
=> Genevieve Weir 1, Tara Quinton 1, Jeff T. Hutchins 2, Bruce D. Freimark 2, Marianne Stanford (VP/Res., Immunovaccine)
1=Immunovaccine, Inc., Halifax, NS, Canada [ https://www.imvaccine.com ]
2=Peregrine Pharmaceuticals
[Note: clearly, this study is combining PPHM’s Anti-PS with ImmunoVaccine’s DepoVax Vaccine Adjuvanting Platform https://www.imvaccine.com/depovax.php ]
ABSTRACT:
Antibodies targeting phosphatidylserine (PS) have been shown to induce anti-tumor responses by induction of tumor-specific T cells. Based on this observation, we evaluated the responses of PS and PD-1 targeting antibody therapy to enhance anti-tumor responses of a HPV16 peptide vaccine formulated in DepoVax (DPX) in mice bearing HPV-transformed C3 mouse tumors. The addition of PS-targeting antibody (mch1N11) [“Mouse version of Bavituximab”] to DPX/metronomic cyclophosphamide (mCPA) immunotherapy prolonged survival in comparison to mice receiving an isotype control in combination with DPX/mCPA. When anti-PD-1 was added to mch1N11 + mCPA, there was no increase in survival. The addition of mch1N11 to DPX/mCPA immunotherapy had no effect on tumor growth or survival in the aggressive B16-F10 model. TIL analysis revealed an increase in CD8+ T cells, antigen specific CD8+ T cells and PD-1+ T cells in the tumor with mch1N11 treatment. The expression of surface markers for macrophages (CD68high, F4/80) and dendritic cells (CD11c) were also increased in the tumors of mice treated with mch1N11. RT-qPCR analysis of the tumor confirmed higher mRNA expression of T cells markers (CD8, Granzyme B, PD-1) and antigen presenting cell markers (F4/80, CD74). In the spleen, expression of cell surface markers for monocytes (CD11b) and PD-1+ T cells (CD8) were elevated in groups treated with mch1N11 in combination with anti-PD-1. Combined, these findings indicate that in this model, PS-targeting antibodies can enhance the activity of phagocytic cells involved in antigen presentation. We have found that PD-1 expression increases as anti-tumor activity increases, therefore these results also provide an indication that antibodies targeting PS enhance the anti-tumor immune response induced by DPX/mCPA therapy. The observations suggest that PS-targeting antibodies may enhance therapeutic vaccines for the treatment of cancer.
-------
3-24-17 Immunovaccine PR: “Immunovaccine to Present New Preclin. Combo Therapy Data at AACR’17” …Immunovaccine conducted this research in collaboration with Peregrine Pharm. with the goal of analyzing the potential enhanced anti-cancer activity of combining DepoVax-based cancer immunotherapies with Peregrine's lead clinical product candidate bavituximab… Immunovaccine Dir./Res. Genevieve Weir will present data analyzing the potential for enhanced anti-tumor responses of PS & PD-1 targeting antibody therapies when combined with an HPV16 peptide vaccine formulated in Immunovaccine's proprietary DepoVax technology. "Our work with Peregrine, and the research it has produced, fits squarely into our corporate objective of exploring clinical stage immunotherapies that may have synergistic effects when combined with our lead candidate, DPX-Survivac," said Marianne Stanford (PhD) VP/Res. for Immunovaccine. "We look forward to discussing the results of this study, and its potential implications, with our colleagues in the scientific community at this year's AACR meeting." https://www.imvaccine.com/releases.php?releases_id=418
------------------------
POSSIBLE GENESIS OF IMMUNOVACCINE COLLAB???
11-9-15 SITC'15: New Bavi+Checkpoint Inhibitors preclin. data (UTSW/DUKE's Herbert K. Lyerly) http://tinyurl.com/pbof95w
...Also, collab. with Dr. Bernard Fox (Immunotherapist/Earle A. Chiles Res.Inst.) on new Immuno-Profiling Clinical Test (Opal 6-plex quantitative IF Assay), PPHM roundtable with Raymond Birge (Rutgers), Douglas Graham (Emory), Dmitry Gabrilovich (Wistar), Rolf Brekken (UTSW), Maria Karasarides (AstraZeneca) - ”Combining Bavi w/anti-PD-1 significantly enhanced O/S… significant incr. CD45+, CD8+ and CD3+ T-cells… led a prolonged anti-tumor immune response which protected the animals against a re-challenge w/same tumor.”
==========================
Apr1-5: AACR 2017, WashDC http://tinyurl.com/mxz23gz - SUMMARY of PPHM’s 5 AACR’17 ABSTRACTS: [See DETAILS below]
1. MSKCC+PPHM: 4-2-17/1pm #574, “PSTargeting+RAD+AntiPD1 Promotes Anti-Tumor Activity, Melanoma” (same as SITC'16/11-14-16 http://tinyurl.com/js3fca4 )
2. MSKCC+PPHM: 4-3-17/8am #1651, “PSTargeting+Adoptive TCell Transfer (ACT) Eliminates Adv. Tumors w/o Off-Target Toxicities, Melanoma” <=NEW(2nd) Joint MemSloan/PPHM study, see: http://tinyurl.com/h3ylrku
3. PPHM: 4-4-17/8am #3652, “PSTargeting+LAG3+AntiPD1 Significantly Enhances Anti-Tumor Activity, Triple- MBC”
4. IMMUNOVACCINE+PPHM: 4-4-17/8am #3657, ”PSTargeting Enhances Anti-Tumor Activity of a Tumor Vaccine(DepoVax), HPV-Induced Tumor” https://www.imvaccine.com See 3-24-17: https://www.imvaccine.com/releases.php?releases_id=418
5. PPHM+VANDERBILT+PRECISIONMEDICINE+PROVIDENCECC: 4-3-17/1pm #CT159/25 (Session: Ph2/3 Clinical Trials in Progress), “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” (abstract embargoed, Sunrise Biomarker #3) - See below.
ALSO: Peregrine Exhibiting – booth #3312.
Added more facts about AACR'17 = Jedd.Wolchok's "The_Peregrine_Show". 
Known Upcoming Events (incl. AACR’17 w/New MSK/Wolchok, NEW-BIOMARKER)
Apr1-5: AACR 2017, WashDC http://tinyurl.com/mxz23gz - SUMMARY of PPHM’s 5 AACR’17 ABSTRACTS: [See DETAILS below]
1. MSKCC+PPHM: 4-2-17/1pm #574, “PSTargeting+RAD+AntiPD1 Promotes Anti-Tumor Activity, Melanoma” (same as SITC'16/11-14-16 http://tinyurl.com/js3fca4 )
2. MSKCC+PPHM: 4-3-17/8am #1651, “PSTargeting+Adoptive TCell Transfer (ACT) Eliminates Adv. Tumors w/o Off-Target Toxicities, Melanoma” <=NEW(2nd) Joint MemSloan/PPHM study, see: http://tinyurl.com/h3ylrku
3. PPHM: 4-4-17/8am #3652, “PSTargeting+LAG3+AntiPD1 Significantly Enhances Anti-Tumor Activity, Triple- MBC”
4. IMMUNOVACCINE+PPHM: 4-4-17/8am #3657, ”PSTargeting Enhances Anti-Tumor Activity of a Tumor Vaccine(DepoVax), HPV-Induced Tumor” https://www.imvaccine.com
5. PPHM+VANDERBILT+PRECISIONMEDICINE+PROVIDENCECC: 4-3-17/1pm #CT159/25 (Session: Ph2/3 Clinical Trials in Progress), “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” (abstract embargoed, Sunrise Biomarker #3) - See below.
Jun2-6: ASCO 2017, Chicago https://am.asco.org (Abstracts: Titles/MidAPR, Full=May17)
...Peregrine will be presenting at ASCO’17, per CEO Steve King, 3-13-17 CC Q&A. http://tinyurl.com/grhwjvy
Jun19-22/Avid Booth #1411: BIO Intl. Convention, SanDiego http://www.convention.bio.org/2017
~Jul13: FY'17Q4 (fye 4-30-17) Financials & Conf. Call - http://ir.peregrineinc.com/events.cfm
.
.
.
= = = = = = = = = = = = = = = = = =AACR’17(Apr2-4) DETAILS...
AACR’17(Apr2-4), 5 PPHM ABSTRACTS: 2/MemSloan, 1/Immunovaccine, 1/PPHM-Only. There’s also a 5th one (PPHM, Vanderbilt, Precision-for-Medicine, Providence CC) in the “Ph2/3 Clinical Trials” session, whose Abstract is still embargoed: “CT159/25: IFN-y Analysis in Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” – this is our new (3rd) Sunrise Biomaker analysis - see below.
...Add ImmunoVaccine Inc. (Halifax https://www.imvaccine.com ) to the list of collaborators.
...#1651(Apr3) is the newly revealed 2nd joint PPHM+Mem.Sloan/Wolchok preclin. study: “PS Targeting + Adoptive T Cell Transfer Eliminates Advanced Tumors without Off-Target Toxicities in a Melanoma Model” - see more below.
...Memorial Sloan’s Dr. Jedd. Wolchok is co-author of 9 AACR’17 abstracts. 2 of the 9 are w/PPHM re: PS-Targeting. With biotechs, he has one each with Genocea Biosciences(ex-vivo screening), Infinity Pharm(Ph1), Leap Ther.(Ph1), and two with BMS(Ph1+Ph3). The 8th is MSKCC ONLY, and the 9th is jointly w/Cedars-Sinai/LA. http://www.abstractsonline.com/pp8/#!/4292 .
Apr1-5 2017: “AACR 2017”, WashDC http://www.aacr.org/Meetings/Pages/MeetingDetail.aspx?EventItemID=105
Abstracts: http://www.abstractsonline.com/pp8/#!/4292
AACR’17 DETAILS (5 PPHM ABSTRACTS)...
= = = = = = = = = = = = = = = = = = =
1. 4-2-17/1pm #574 - Session: CHECKPOINTS 1
“Phosphatidylserine Targeting Antibody in Combination with Tumor Radiation & Immune Checkpoint Blockade Promotes Anti-Tumor Activity in Mouse B16 Melanoma”
=> Sadna Budhu 1, Olivier De Henau 1, Roberta Zappasodi 1, Rachel Giese 1, Luis F. Campesato 1, Christopher Barker 1, Bruce Freimark 2, Jeff Hutchins 2, Jedd D. Wolchok 1, Taha Merghoub [Memorial Sloan Kettering]
1=Memorial Sloan Kettering CC, NYC [ http://www.mskcc.org/research-areas/labs/jedd-wolchok ]
2=Peregrine Pharmaceuticals
NOTE: SAME TITLE AS WAS PRESENTED BY Mem.Sloan 11-14-16 SITC’16: see http://tinyurl.com/js3fca4
ABSTRACT:
Phosphatidylserine (PS) is a phospholipid that is exposed on surface of apoptotic cells, tumor cells and tumor endothelium. PS has been shown to promote immunosuppressive signals in the tumor microenvironment. Antibodies that target PS have been shown to reactivate anti-tumor immunity by polarizing tumor associated macrophages into a pro-inflammatory M1 phenotype, reducing the number of MDSCs in tumors and promoting the maturation of dendritic cells into functional APCs. In a mouse B16 melanoma model, targeting PS in combination with immune checkpoint blockade promoted greater anti-tumor activity than either agent alone. This combination was shown to enhance CD4+ and CD8+ T cell infiltration and activation in the tumors of treated animals. Radiation therapy (RT) is an effective focal treatment of primary solid tumors, but is less effective in treating metastatic solid tumors as a monotherapy. There is evidence that RT induces immunogenic tumor cell death and enhances tumor-specific T cell infiltration in treated tumors. The abscopal effect, a phenomenon in which tumor regression occurs outside the site of RT, has been observed in both preclinical and clinical trials when RT is combined with immunotherapy. In this study, we show that irradiation treatment of B16 melanoma causes an increase in PS expression on the surface of viable tumor and immune infiltrates. We subsequently examined the effects of combining RT with an antibody that targets PS (mch1N11) [“Mouse version of Bavituximab”] and immune checkpoint blockade (anti-PD-1) in B16 melanoma. We found that treatment with mch1N11 synergizes with RT to improve anti-tumor activity and overall survival in tumor bearing mice. In addition, the triple combination of mch1N11, RT and anti-PD-1 treatment displayed even greater anti-tumor and survival benefit. Analysis of local immune responses in the tumors of treated animals revealed an increase in tumor-associated macrophages with a shift towards a pro-inflammatory M1 phenotype after treatment with RT & mch1N11. In addition, analysis of the systemic immune responses in the spleen and tumor draining lymph nodes revealed an increase in CD8 T cell activation, effector cytokine production and differentiation into effector memory cells in the triple combination. This finding highlights the potential of combining these 3 agents to improve outcome in patients with advanced-stage melanoma and other cancers and may inform the design of clinical studies combining PS-targeting antibodies with RT and/or checkpoint blockade.
= = = = = = = = = = = = = = = =
2. 4-3-17/8am #1651 - Session: TUMOR MICROENVIRONMENT & CHECKPOINTS
“Targeting Phosphatidylserine in Combination with Adoptive T Cell Transfer Eliminates Advanced Tumors without Off-Target Toxicities in a Melanoma Preclinical Model” <=NEW(2nd) MSK STUDY$$$
…...$$$See: More on the Significance of the New MSK/Wolchok+PPHM “ACT” study: http://tinyurl.com/h3ylrku
=> Daniel Hirschhorn-Cymerman 1, Sara Sara Schad 1, Sadna Budhu 1, Zhong Hong 1, Xia Yang 1, Hutchins T. Jeff 2, Bruce D. Freimark 2, Michael J. Gray 2, Jedd Wolchok 1, Taha Merghoub [Memorial Sloan Kettering]
1=Memorial Sloan Kettering CC, NYC [ http://www.mskcc.org/research-areas/labs/jedd-wolchok ]
2=Peregrine Pharmaceuticals
ABSTRACT:
A viable strategy to treat advanced cancers includes transferring of tumor-specific T cells. T cells that recognize tumor antigens can be expanded and reinvigorated ex-vivo. Furthermore, autologous T cells can be genetically modified to express anti-tumor T cell receptors or chimeric antigen receptors. Although the potency and specificity of tumor-specific T cells can be manipulated ex-vivo, once re-infused into patients, the T cells are subjected to immunosuppressive mechanisms established by the tumor. An important immune checkpoint regulator within tumors is phosphatidylserine (PS). Innate immune cells exposed to PS secrete suppressive cytokines and chemokines that can significantly impair the function and activation of anti-tumor T cells. Therefore, monoclonal antibodies that block PS activity can increase the anti-tumor potency of transferred T cells to treat aggressive cancers. Here we show that a PS targeting monoclonal antibody in combination with CD4+ T cells that recognize the melanoma antigen Trp1 can regress very advanced melanomas in all treated mice. Combination of anti-Trp1 CD4+ T cells with other immunomodulatory modalities such as anti-OX40 antibodies, can achieve equivalent treatment rates but these are typically accompanied by severe immune related adverse events. In contrast, in this setting, PS blockadedid not show any off-target toxicities. Flow cytometry analysis revealed lower levels of CD206 expression concomitant with higher activation markers in macrophages and neutrophils in tumors from anti-PS treated mice. These results suggest that diminishing suppressive mechanisms locally in adoptive transfer protocols is a highly desirable strategy that can eliminate tumors while minimizing related adverse events.
----------
NOTE1:
From 3-2014 Immunotherapy article: “Cancer immunotherapy, particularly adoptive cell transfer (ACT), has shown great promise in the treatment of patients with late-stage disease, including those who are refractory to std. Therapies” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4372895
NOTE2:
Through the support from SEAN PARKER, Stand Up To Cancer (SU2C) and the Cancer Research Institute (CRI) formed an Immunology Research Dream Team dedicated to cancer immunology: “Immunologic Checkpoint Blockade & Adoptive Cell Transfer in Cancer Therapy.” The Immunotherapy Dream Team is focused on 2 approaches for this translational cancer research project, which will unite laboratory & clinical efforts towards the immunological treatment, control, and prevention of cancer.
The 1st is investigating blockades (by inhibitory molecules called “checkpoints”) of T lymphocytes’ inhibitory receptors, which block immune responses; and the use of antibodies to remove the checkpoints, once again allowing white blood cells called T lymphocytes to kill the cancer cells.
Second, the Immunotherapy Dream Team is pursuing multiple Adoptive Cell Transfer (ACT) approaches, which increase immunity.”
DREAM TEAM LEADERSHIP: 10 scientists, incl. MSKCC’s Jedd D. Wolchok & Michel Sadelain.
http://parker.org/initiatives/immunotherapy
= = = = = = = = = = = = = = = =
3. 4-4-17/8am #3652 - Session: BITES BISPECIFICS & CHECKPOINTS
“Combinational Activity of LAG3 & PD-1 Targeted Therapies is Significantly Enhanced by the Addition of Phosphatidylserine Targeting Antibodies and Establishes an Anti-Tumor Memory Response in Murine Triple Negative Breast Cancer”
=> Michael J. Gray, Jian Gong, Jeff Hutchins, Bruce Freimark (Peregrine Pharmaceuticals)
ABSTRACT:
Previous studies utilizing NanoString immune profile analysis demonstrated that intratumoral levels of LAG3 (lymphocyte activation gene 3) mRNA increased in response to phosphatidylserine (PS) and PD-1 targeting antibodies in murine triple negative breast cancers (TNBC). This suggests LAG3 acts to attenuate immune system activation during I/O therapies - and that PD-1 and LAG3 function cooperatively in suppressing immune system activation. Here we show that adding PS targeting antibodies can further enhance the effectiveness of antibodies targeting LAG3 and/or LAG3+PD-1. We first examined expression of LAG3 and PD-1 in the murine TNBC model E0771 and found that tumor associated T-cells (CD4+ and CD8+) have expression of both markers. Mice implanted with TNBC tumors were next treated with antibodies targeting PS, PD-1, and LAG3 alone and in combination with each other. Interestingly, the addition of PS targeting antibodies not only increased the effectiveness anti-PD-1 effectiveness as previously observed, but also enhanced anti-LAG3 treatment, showing that PS targeting antibodies are capable of augmenting additional I/O therapeutic regimens. Comparison of anti-PD-1+LAG3 combination vs. single anti-PD-1 or anti-LAG3 treatments showed moderately more anti-tumor activity than single treatments, however the addition of PS targeting antibodies to either checkpoint inhibitor was as equally effective in inhibiting tumor growth as observed in the anti-LAG3+PD-1 treatment. Further comparison of antibody treatments targeting PD-1+LAG3 vs. PS+PD-1+LAG3 demonstrated that the addition of PS targeting antibodies resulted in a significant decrease in tumor growth with complete tumor regression in 80% of the animals (along with the ability to completely reject secondary TNBC challenge) compared to 0% in the anti-PD-1+LAG3 treatment group. Immunoprofiling showed that the addition of PS targeting antibodies to these checkpoint therapies, including the combination of anti-PD-1+LAG3, resulted in a phenotype associated with enhanced immune system activation and immune-surveillance including increased tumor infiltrating lymphocytes (TILs) with upregulation of T-cell associated activation pathways, increased Th1 to Th2 profile, and enhanced antigen presentation processing /presentation mechanisms along with cytokines associated with immune system activation. Overall our data demonstrate that adding PS targeting antibodies to clinically relevant therapies, including PD-1 and LAG3, may significantly enhance their ability to activate and redirect the host immune system into recognition and elimination of tumor cells compared to single and combinational treatments that lack PS targeting antibodies.
= = = = = = = = = = = = = = = =
4. 4-4-17/8am #3657 - Session: BITES BISPECIFICS & CHECKPOINTS
”Phosphatidylserine-Targeting Antibodies Enhance Anti-Tumor Activity of a Tumor Vaccine in a HPV-Induced Tumor Model”
=> Genevieve Weir 1, Tara Quinton 1, Jeff T. Hutchins 2, Bruce D. Freimark 2, Marianne Stanford (VP/Res., Immunovaccine)
1=Immunovaccine, Inc., Halifax, NS, Canada [ https://www.imvaccine.com ]
2=Peregrine Pharmaceuticals
[Note: clearly, this study is combining PPHM’s Anti-PS with ImmunoVaccine’s DepoVax Vaccine Adjuvanting Platform https://www.imvaccine.com/depovax.php ]
ABSTRACT:
Antibodies targeting phosphatidylserine (PS) have been shown to induce anti-tumor responses by induction of tumor-specific T cells. Based on this observation, we evaluated the responses of PS and PD-1 targeting antibody therapy to enhance anti-tumor responses of a HPV16 peptide vaccine formulated in DepoVax (DPX) in mice bearing HPV-transformed C3 mouse tumors. The addition of PS-targeting antibody (mch1N11) [“Mouse version of Bavituximab”] to DPX/metronomic cyclophosphamide (mCPA) immunotherapy prolonged survival in comparison to mice receiving an isotype control in combination with DPX/mCPA. When anti-PD-1 was added to mch1N11 + mCPA, there was no increase in survival. The addition of mch1N11 to DPX/mCPA immunotherapy had no effect on tumor growth or survival in the aggressive B16-F10 model. TIL analysis revealed an increase in CD8+ T cells, antigen specific CD8+ T cells and PD-1+ T cells in the tumor with mch1N11 treatment. The expression of surface markers for macrophages (CD68high, F4/80) and dendritic cells (CD11c) were also increased in the tumors of mice treated with mch1N11. RT-qPCR analysis of the tumor confirmed higher mRNA expression of T cells markers (CD8, Granzyme B, PD-1) and antigen presenting cell markers (F4/80, CD74). In the spleen, expression of cell surface markers for monocytes (CD11b) and PD-1+ T cells (CD8) were elevated in groups treated with mch1N11 in combination with anti-PD-1. Combined, these findings indicate that in this model, PS-targeting antibodies can enhance the activity of phagocytic cells involved in antigen presentation. We have found that PD-1 expression increases as anti-tumor activity increases, therefore these results also provide an indication that antibodies targeting PS enhance the anti-tumor immune response induced by DPX/mCPA therapy. The observations suggest that PS-targeting antibodies may enhance therapeutic vaccines for the treatment of cancer.
= = = = = = =THIS A NEW (3RD) KNOWN SUNRISE BIOMAKER ANALYSIS:
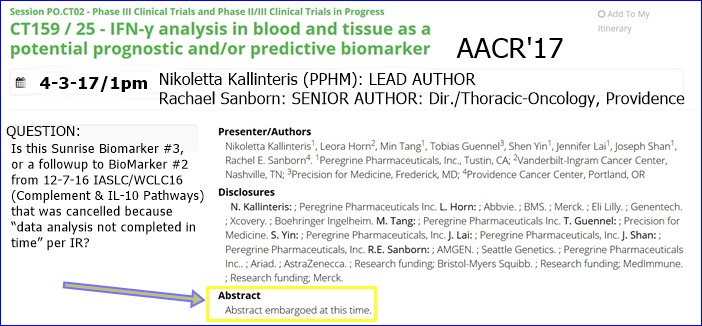
#5. 4-3-17/1pm #CT159/25 - Session: Phase III Clinical Trials & Phase II/III Clinical Trials in Progress
http://www.abstractsonline.com/pp8/#!/4292/presentation/12566
”IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker”
=> Nikoletta Kallinteris 1, Leora Horn 2, Min Tang 1, Tobias Guennel 3, Shen Yin 1, Jennifer Lai 1, Joseph Shan 1, Rachel E. Sanborn (Providence CC)*** 4
1=Peregrine Pharmaceuticals
2=Vanderbilt-Ingram Cancer Center, Nashville, TN
3=Precision for Medicine, Frederick, MD
4=Providence Cancer Center, Portland, OR
***Rachel Sanborn MD, Dir./Thoracic-Oncology, Providence CC http://cancergrace.org/faculty/rachel-sanborn-md - Dr. Sanborn's Conflicts of interest: DNA, AZN
ABSTRACT: Embargoed – assuming until 4/3/17.
-------
This AACR’17 #5 is certainly the 3rd Sunrise Biomarker.
Known Ph.3 Sunrise Biomarkers/UTSW’s Dr. David Gerber et al:
#1=B2GPI: 10-10-16 http://tinyurl.com/hp73njt
#2=Complement & IL-10 Pathways(12-7-17/IASLC delayed, “not done”, after prelim. abstract said, “Pts=193, within the 1st subgroup of N=104, a 2nd subgroup isolated: MOS 5.9=>12.5mos”
#3=IFN-y (this 4-3-17 AACR’17 one, #CT159/25)
The results of th the Biomarkers analysis may drive into the design of the 3 planned NCCN human trials and the AZN Bavi+Durva ‘Mult. Solid Tumors’ trial, the design of which is currently “under evaluation”. See http://tinyurl.com/jbv3ms5
- - - - - - -
***Maybe Dr. Ranee Mehra (Johns Hopkins, PPHM’s NCCN Bavi+Keytruda Head&Neck Ph2 P.I.) will stop by!
...Dr. Mehra’s work with Biomarker IFN-y seems to dovetail into PPHM’s newly revealed Sunrise Biomarker #3 to be presented 4-3-17 at AACR’17: #CT159/25, “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” ( http://tinyurl.com/zaz525l ).

Note: DR. RANEE MEHRA was co-author of ASCO’16, “Biomarkers & Response to Pembro(Keytruda) in Recurrent/Metastatic Head & Neck Cancer” - Conclusion: “The IFN-y signature score was significantly associated with ORR, PFS, and OS (all, P< .001)… PD-L2 & IFN-y signature may be associated with clinical response to Pembro[Keytruda] and may offer addl. strategies to improve prediction of response.” http://meetinglibrary.asco.org/content/165708-176
MORE: http://tinyurl.com/h8gzkww

- - - - - - - - - - - - - - - - - - -
INTERESTING: Mem. Sloan’s Dr. Jedd. Wolchok is co-author of 9 AACR’17 abstracts. 2 of the 9 are w/PPHM re: PS-Targeting. With biotechs, he has one each with Genocea Biosciences(ex-vivo screening), Infinity Pharm(Ph1), Leap Ther.(Ph1), and two with BMS(Ph1+Ph3). The 8th is MSKCC ONLY, and the 9th is jointly w/Cedars-Sinai/LA. http://www.abstractsonline.com/pp8/#!/4292 .
PEREGRINE (Joint Mem.Sloan Kettering Wolchok Lab & PPHM):
1. 4-2-17 #574 “Phosphatidylserine Targeting Antibody in Combination with Tumor Radiation & Immune Checkpoint Blockade Promotes Anti-Tumor Activity in Mouse B16 Melanoma” <=Same as SITC’16 11-14-16.
2. 4-3-17 #1651 “Targeting Phosphatidylserine in Combination With Adoptive T Cell Transfer Eliminates Advanced Tumors Without Off-Target Toxicities in a Melanoma Preclin. Model” <=NEW/2nd PPHM+MSK.
NON-PEREGRINE:
3. (MSK ONLY): 4-2-17 #874 “Lifting the iron curtain: Imaging cellular barriers to combination chelation-immune checkpoint therapy”
4. (MSK & Genocea Bio. http://www.genocea.com GNCA/$130mm MktCap) 4-2-17 #632 “Genome-scale neoantigen screening using ATLAS prioritizes candidate antigens for immunotherapy in a NSCLC patient”
5. (MSK & Cedars-Sinai/LA) 4-4-17 #4705 “CTLA4 blockade with HER2-directed therapy yields clinical benefit in women undergoing radiation therapy for HER2+ breast cancer brain metastases”
6. (MSK & Infinity Pharm.) 4-4-17 #CT089 “A Ph1, first-in-human study of IPI-549, a PI3K-y inhibitor, as monotherapy & in combo w/nivolumab in adv. solid tumors”
7. (MSK & Leap Ther.) 4-2-17 #CT018 “Intratumor & peripheral Treg modulation as a pharmacodynamic biomarker of the GITR agonist antibody TRX-518 in the 1st in-human trial”
8. (MSK & BMS) 4-3-17 #CT073 “(Ph1) Immunomodulatory effects of NIVO+IPI or NIVO/mono in adv. melanoma: CheckMate038”
9. (MSK & BMS) 4-3-17 #CT075 “OS results from a Ph3 of NIVO+IPI in treatment-naïve pts w/adv. Melanoma: CheckMate067”
= = = = = = = = = = = = =
2-28-17: Collabs with Mem.Sloan(Wolchok), Duke, MDA, Rutgers, ImmunoVaccine, UTSW… http://tinyurl.com/heg9t3v
BAVI MOA 11-14-16: SITC’16: Joint Memorial Sloan Kettering (Wolchok Lab) & PPHM poster on Triple Combo Rad+Bavi+aPD1 vs. Melanoma http://tinyurl.com/js3fca4
“PS Targeting Antibody in Combination with Checkpoint Blockade & Tumor Radiation Therapy Promotes Anti-Cancer Activity in Mouse Melanoma” (same as AACR’17 4-2-17 #574)
DR. JEDD WOLCHOK: "Based on these study results, we believe that the targeting of PS is having meaningful activity within the tumor microenvironment in the B16 melanoma model. It appears that this activity creates a more immune active environment in which other treatments, including radiation, are able to have a greater anti-tumor impact."
DR. TAHA MERGHOUB (Co-Dir., Ludwig Collaborative Lab at MSK): "We have noted that the combination of PS-targeting treatment and radiation, as well as triple combination of PS-targeting treatment, radiation and anti-PD-1, resulted in clear advantages in anti-tumor activity in the mouse B16 melanoma model. We believe that these findings suggest the potential benefit of combining these agents to improve the outcomes of patients with cancer. With this in mind, we think this research may play an important role in designing future clinical trials of PS-targeting agents in melanoma and other cancers."
5-29-15: Peregrine & Sloan Kettering Enter Collab. to “Investigate Novel PS-Targeting Immunotherapy Combos” http://tinyurl.com/o3k9ux8
...Dr. Wolchock states, ”The phosphatidylserine (PS) signaling pathway is a very interesting target for modulating the immune system's response to cancer. We look forward to exploring the potential of PS-targeting agents alone and with other immune modulators that may lead to novel advances in cancer therapy.”
...Dr. Taha Merghoub states, "A key focus of the Wolchok Lab's research is studying novel immunotherapy combinations that work together to enable the immune system to recognize & destroy cancer. This collaboration will allow us to focus on the role & contribution of PS blockade therapy in determining which combination of the current & next gen. of immune modulators is likely to increase the extent & amplitude of anti-tumor response. This important pre-clinical and translational work will potentially guide the design of the next gen. of clinical studies with bavituximab.”
POSSIBLE GENESIS OF IMMUNOVACCINE COLLAB???
11-9-15 SITC'15: New Bavi+Checkpoint Inhibitors preclin. data (UTSW/DUKE's Herbert K. Lyerly) http://tinyurl.com/pbof95w
...Also, collab. with Dr. Bernard Fox (Immunotherapist/Earle A. Chiles Res.Inst.) on new Immuno-Profiling Clinical Test (Opal 6-plex quantitative IF Assay), PPHM roundtable with Raymond Birge (Rutgers), Douglas Graham (Emory), Dmitry Gabrilovich (Wistar), Rolf Brekken (UTSW), Maria Karasarides (AstraZeneca) - ”Combining Bavi w/anti-PD-1 significantly enhanced O/S… significant incr. CD45+, CD8+ and CD3+ T-cells… led a prolonged anti-tumor immune response which protected the animals against a re-challenge w/same tumor.”
SITC’16 PPHM/Mem.Sloan Poster – same as AACR’17 4-2-17 #574…

3-13-17/CC Re-Read – A few things popped out...
3-13-17/CC: STEPHEN WORSLEY (VP/Bus.Dev.)
“In the near-term, we are aggressively working to expand Avid’s client base, and in Q3 we signed another new client for a late-stage clinical product. We are currently in discussions with a number of prospective new clients, and we expect to sign addl. clients in the coming months.”
--------
Avid Revs FY17(fye 4-30-17) Guidance upped by +$10mm to $60-65mm. I went back 4 prior years – they’ve never failed to TOP the upper-ends of prior March Guidances. With Revs for 1st 3qtrs = (5.6 + 23.4 + 10.7) = $39.7mm, if they follow suit, Q4 Revs will be at least (65mm – 39.7) = $25mm. ...How close would that get us to Cash-Flow positive for Q4, should it happen? OP. CASH BURN for Q3(1-31-17) was: $6,274,000, and that's with Revs=$10.7mm at GM=26%.
Period Halozyme Cust-A Other-Custs
FYE 4-30-14 91% 1% 8%
FYE 4-30-15 79% 12% 9%
FYE 4-30-16 69% 26% 5%
Q/E 7-31-16 65% 29% 6%
Q/E 10-31-16 77% 10% 13%
Q/E 1-31-17 29% 56% 15%
3-13-17 Qtly CC-Transcript, PR(Financials Q3FY17/qe1-31-17), updated Avid Revenues History Table By Quarter…
=> Total Revs May06-Jan17: $213.3mm/Avid + $24.1mm/Govt + $2.4mm/Lic. = $239.9mm.
Cash at 1-31-17: $41.5mm (Op. Cash Burn for q/e 1-31-17 was $6.3mm – see below).
As of Mar. 10, 2017, there were 297,709,478 shares outstanding.
This large post has 3 sections:
I. 3-13-17 Q3/FY17 Qtly. Earnings Conf. Call TRANSCRIPT (q/e 1-31-17)
II. 3-13-17 PPHM Press Release: Q3/FY17 Earnings & Developments
III. Updated Table of Avid Revenues By Quarter (May’06-Current)
…Recall: Peregrine’s FY runs May-Apr, so FY’17 = May’16-Apr’17.
((( Orig. transcript from SeekingAlpha.com [ http://tinyurl.com/zjnz76k ], with numerous corrections made. )))
Link to webcast replay: http://ir.peregrineinc.com/events.cfm => http://edge.media-server.com/m/p/2aw6274a
FULL TRANSCRIPT… 3-13-2017 FY’17/Q3 Earnings Conf. Call (q/e 1-31-17) (King/Shan/Worsley/Lytle)
WELCOME & FWD-LOOKING STATEMENTS: Tim Brons, Vida Strategic Partners (IR) http://www.peregrineinc.com
CEO STEVE KING – OPENING COMMENTS:
Thanks to all of you who have dialed in, and to all of you who are participating via webcast today. During the quarter, Avid’s revenue growth continued, representing a strong indicator of the increasing value of this contract development & mfg. organization, or CDMO, business. The steady growth of this business over the past 5 years has been remarkable, at almost 40% compounded annual growth rate, and we are pleased to see the trend continuing, even as we move through a number of process validations for clients, which we believe and expect to further support growth in the future, as potentially some or all of these products enter commercialization. Commercial production has been the cornerstone of our revenue growth, and being able to potentially expand the number of commercial products we manufacture, while supporting the expansion of the existing commercial products into new territories, is a priority. Making these process validation activities, along with the recent successful preapproval inspection for a major market, are very important milestones and are continuing to grow the Company. We already produce drug specimens for several commercial products that are marketed in over 15 countries. Taking together, we are building a solid foundation for future growth of the business through new introductions and by continuing to support the current customers through clinical development and into commercialization. An important component of our Avid growth strategy is capacity expansion within our Myford facility. We are currently on track to install two 2,000-liter bioreactors in the facility within the next few months, with a book of business for the reactors already in place. We believe the total capacity potential of the facility, when operating in campaign mode, can exceed more than $75mm annually, bringing us to well over $100mm in total potential revenue between our 2 mfg. facilities, providing us with adequate capacity to continue Avid revenue growth through FY’18. As we look beyond this FY and into the future, based on current operations & projected demand from our clients, we have also recently secured addl. space adjacent to our Myford facility, which we already have the use for as part of our growing operations. And additionally, would also allow us to further expand mfg. capacity based on committed business. While we will only begin converting space into mfg. capacity once client commitments and other necessary financing is in place, this puts us in an excellent position for continuing to grow the business beyond the coming FY. We already see Avid as a tremendously important asset with solid upside potential that it often overlooked as a value driver for the overall company. With projected revenue of over $60mm for the current FY, this is already a strong business in an industry that is expecting substantial growth over the next decade, and we are excited about future of the Company. We believe the recent improvement of stock price is a growing recognition of the value of Avid, and having the full value of the Avid business reflected in our stock price is a top priority.
During the quarter, we also achieved a number of goals on the other side of our business, drug development. While we are moving our dev. programs forward on a tight budget, we are working with some of the top research institutions in the world to explore the best ways to advance our lead bavituximab program. These efforts are highlighted by the 3 clinical trials under our collaboration with the National Comprehensive Cancer Network (NCCN), which are advancing as planned, and we expect at least 2 of the trials to be initiated by mid-year. Also during the quarter, working independently and in conjunction with our collaborators, we had multiple abstract accepted for presentations at AACR’17 in April [AACR’17:http://tinyurl.com/zzldh9n ]. These findings reinforce our belief that an immune activating mechanism, like bavituximab, can be an important component of combination cancer treatment approaches by significantly impacting the tumor microenvironment, creating a more favorable environment for checkpoint inhibitors. We look forward to further emphasizing the value of this research as the presentations are made and as the new trials get underway. Needless to say, we are excited to be working together with the world class researchers and clinicians at Memorial Sloan Kettering, UT Southwestern, and the NCCN.
Additionally during the quarter, our collaboration at the UTSW-MC published positive proof-of-content data for our recently licensed Exosome-based Cancer Detection Platform [2-9-17/UTSW’s Dr. Alan Schroit, PPHM SAB: http://tinyurl.com/jhv57ua ], which could have broad potential for patients with cancer. Results of the study showed that researchers were able to distinguish between healthy subjects and patients with ovarian tumors, based on the level of exosomes containing phosphatidylserine found in their blood. Further analysis of the PS positive exosome levels allowed researchers to further distinguish between malignant and benign tumors. While the work in this program is early, we are highly encouraged by the observed cancer detection capability of this platform, and we are actively seeking a partner to advance this diagnostic.
As a whole, even though we have reduced our R&D expenditures, we are pleased that collaborations, such as those with Memorial Sloan Kettering, NCCN and UTSW [Collabs: http://tinyurl.com/heg9t3v ], are allowing us to continue the advancement of our therapeutic & diagnostic programs as we continue to evaluate the best ways for advancing bavituximab and other PS targeting agents. The combined effort of the Avid bio-manufacturing business and these important collaborations are allowing us to make great strides in all fronts. I will now turn the call over to the other members of our team who will give you a detailed overview of our clinical and corporate activities, as well as our Avid Bioservices contract mfg. business. We will begin with Joe Shan...
JOE SHAN (VP/Clin.&Reg. Affairs) – CLINICAL TRIALS:
During the quarter, we continued to wrap-up patient treatment and follow-up with our SUNRISE trial. While the study was discontinued in Feb.2016, follow-up data collection continues, and patients assigned to bavituximab containing arm were allowed to continue receiving study drugs, if the investigators determined it was in the patients’ best interest. This has been a valuable effort and we are very pleased with the amount of data that has been collected over the past year. It is important to mention that we are now working diligently to transition the remaining patients still receiving bavituximab to compassionate-use programs. We have recently concluded data collection and are now working towards day-to-day slots and beginning our final analyses, and hope to present results later in the year. We’re in the meantime evaluating ways to advance bavituximab with immune stimulating therapies as resources permit, while supporting the stated corporate profitability goals. Concurrently, we’re completing patient sample testing from the comprehensive SUNRISE Biomarker Program [Biomarkers: http://tinyurl.com/jrenezs ]. Biomarkers play an increasingly important role in helping identify specific patient characteristics that correlate with or even potentially predict response to a treatment. For this reason, our SUNRISE study protocol pre-specified the collection of thousands of patient samples for exploratory analyses over a wide range of possible biomarkers. Through this effort, our team identified a correlation between pre-treatment levels of beta-2 glycoprotein-1 [B2GPI] and overall survival, which was presented at ESMO last October. In early April, at the upcoming AACR Annual Meeting, we will present data from an analysis of pre-treatment interferon gamma [IFN-y]. As the remaining SUNRISE patient samples are tested, we plan to correlate these data with the final clinical data, and plan to share these results as they become available later this year.
Now turning to new trials, I’m happy to report that the 3 clinical trials to be funded through our collaboration with the NCCN are advancing as expected. The first study, expected to begin patient enrolment shortly, is being conducted by Dr. Jessica Frakes, at the Moffitt Cancer Center. This study, which builds upon a prior investigator sponsor trial, will evaluate the combination of Stereotactic Body Radiation Therapy, sorafenib, and bavituximab, for the treatment of Unresectable Hepatocellular [Liver] Carcinoma. We are interested in this trial design as radiation has been shown to increased PS expression on the surface of tumor cells, induce immunogenic tumor cell depth, and increase tumor specific T-cell activity. In addition, NCCN has recently communicated that both the study of bavituximab, temozolomide, and radiation in newly diagnosed Glioblastoma and the trial of bavituximab & temozolomide in recurrent Head & Neck cancer, which has progressed on checkpoint inhibitor treatment, are on track to be initiated by mid-year. This concludes my comments today. I’ll now turn the call over to Steve Worsley…
----------NCCN:
[...#1: Ph1/HepC-Related Hepatocellular(Liver) (Bavi+RAD+Sorafenib), MOFFITT CANCER CENTER - PI: Jessica Frakes, MD - https://clinicaltrials.gov/ct2/show/NCT02989870
...#2: P1-2/Newly Diag. Glioblastoma (Bavi+RAD+Merck’s Temodar), MASS-GEN. CANCER CENTER - PI: Elizabeth Gerstner, MD
...#3: Ph2/Progressive Squamous Head+Neck (Bavi+Merck’s Keytruda), JOHNS-HOPKINS(Sidney Kimmel CC) - PI: Ranee Mehra, MD (See: http://tinyurl.com/h8gzkww ) ]
STEPHEN WORSLEY (VP/Bus.Dev.)
As previewed by Steve, our Avid business is strong and we are taking steps to establish sustained growth in the near-term and in the future. In the near-term, we are aggressively working to expand our client base, and in Q3 we signed another new client for a late-stage clinical product. We are currently in discussions with a number of prospective new clients, and we expect to sign addl. clients in the coming months. In the long-term, it is essential that we read the market appropriately and respond to the existing needs. At last year’s ISPE/FDA/PQRI Quality Meeting in WashDC, industry leaders gathered to address the most important trends and pressing needs of the CDMO industry with several key takeaways. First, the industry is set for a biologics boom. Today, amongst all pharmaceuticals segments, the oncology market is experiencing the fastest growth at 11% annually. Biosimilars are expected to grow to 25B by 2020, and biologic sales, which currently represent 45% of the top 100 drugs, are expected to increase to 52% by 2020. It is important to note that a majority of our clients are focused on the fast-growing biologics segment of the oncology market. One of the most serious points made by industry leaders was the need to address drug shortages, which, according to Janet Woodcock (Dir. of the FDA CDER) poses a huge risk to patients. According to the FDA, drug shortages peaked in 2011 with 251 shortages reported. Since then, 117 new drug shortages were reported in 2012, with another 44 reported in 2013. A large portion of drug shortages have been and continue to be sterile injectable and other acute drugs, including oncology drugs. Two of the major reasons for such shortages are quality mfg. problems and a lack of production capacity. In consideration of the CDMO industries’ greatest needs, including biologics production expertise, continuous manufacturing, quality and capacity, Avid is uniquely positioned to thrive in the future. Myford is a state-of-the-art model facility capable of providing our customers with the expertise, capacity, and quality required to support the drug supply demand of the pharmaceutical industry. Our quality standards are among the highest in the industry, and we just successfully completed another FDA preapproval inspection in Feb.2017, receiving zero 483 citations. With our current & planned facilities, we believe Avid is well positioned to respond to the needs of this industry and take advantage of this growing global market. This concludes my comments today. I’ll now turn the call over to CFO Paul Lytle…
PAUL LYTLE (CFO): [1-31-17 10Q iss. 3-13-17: http://tinyurl.com/zlozrv4 ]
Before I begin, I’d like to reiterate our financial goal of achieving profitability on an overall basis, starting 15 months from this current qtr-end. Our strategy for achieving this goal is to grow revenue from our contract mfg. business, while reducing our overall spending on R&D. During the first 9mos of FY17, we have made excellent progress toward both of these goals. I’ll first address our contract mfg. revenue. During Q3/FY17, we reported revenue of $10.7mm, and we’ve recognized $39.7mm over the past 9mos. This represents revenue growth of 61% for the qtr and 55% for the 9mos, compared to the same prior year period. Now looking ahead, we are increasing our full FY17 [fye 4-30-17] revenue guidance from $50-55mm to $60-65mm that is supported by our current revenue backlog of $70mm under committed contracts. This new revenue guidance translates into potential revenue growth of between 35% & 47% over FY16.
I’ll now address our efforts to reduce overall spending on R&D. As we announced last July, our R&D strategy has changed. Our goal was to reduce R&D spending by 50% this FY, and to focus our internal drug development efforts on small, cost effective, early stage clinical trials designed to attract potential partners to further advance our products. As we executed on this plan, our R&D expenses for Q3 and 9mo periods decreased 60% & 50% respectively compared to the same prior year period, confirming we are on track with this significant decrease in R&D spending. The result of the strategy has translated into a reduction in our net loss by 54% for Q3 and 48% for the 9mo period vs. the same prior year periods. And while we have achieved a significant decrease in our net loss this FY, our cash position has also decreased by approx. $20mm since the beginning of the FY. Therefore, we want continue to be diligent & thoughtful in our capital raising efforts. To maintain a stable and growing mfg. business, we must continue to raise sufficient capital to support this business. During the current 9mo. period, we carefully raised $11.6mm in net proceeds from the sale of common stock vs. $43.4mm we raised during the same period last year. Our mfg. business is not only valued based on the quality of the operations, but is also based on our ability to sustain our operations. As the business expands, our cash on hand should also increase to support this growing operation.
Switching gears now, I’d like to address our plans to preserve our NASDAQ listing. At a backdrop, last April, we were notified by the NASDAQ that our share price did not meet the $1 min. bid price for 30 consecutive days, which is a requirement for continued listing on the NASDAQ market. At that time, we were automatically afforded an initial compliance period of 180 days or until Oct. 10, 2016 to regain compliance. At the end of the initial compliance period, we requested and were granted a 180 day extension to regain compliance. This 2nd extension period will end on April 10, 2017. Let me discuss our strategy and future steps we plan to take over the next few months. First & foremost, we have determined that it is not in the best interest of our stockholders to affect a reverse stock split prior to April 10, 2017. If our share price does not trade above $1 for 10 consecutive trading days by April 10th, we expect to receive a notice of delisting. If we received this notice, we will appeal this decision within the required 7 days and this appeal will stay any delisting actions by NASDAQ. At that point, NASDAQ will schedule a hearing, which is typically held within 45 days, and we will present our plan to regain compliance. We are considering several paths to regain compliance, including having addl. time to continue to allow the market to adjust, to reflect the current value of Avid as evidence with the recent movement in our share price. The hearing panel could afford us up to 180 addl. days to regain compliance, although this addl. time is not guaranteed and this decision is at the discretion of the NASDAQ’s hearing panel. If we are not afforded addl. time from this panel, it is important to note that our stockholders approved the Board’s ability to implement a reverse stock split at a ratio of up to 1:7 as a means to regain compliance and to preserve our listing on NASDAQ. During this entire process, Peregrine will continue to be listed on that NASDAQ capital market as it does today. We will keep you informed on any material developments through our SEC filings on Form 8-K as we execute on this plan. With that, this concludes my financial overview. And I will now open the call up for questions...
Q&A: [beg. 20:30]
1. Kumara Raja - Noble Life Science Partners http://noblelsp.com/research
KR: ”On the Exosome-based cancer detection platform, you presented some positive data on the ovarian cancer. What other cancers, there is expression of possible serum and what kind of trials are you guys conducting there? And what is the next step for collaboration for this platform, like what needs to be done in terms of trials that need to be done and the state of offset? And also, in terms of the SUNRISE trials, what are you seeing in patients who are continuing on bavituximab? What kind of benefits are you seeing there? And you’ve talked about Compassionate Use Program, what needs to be done for that in different countries? And then, in terms of cost of contract mfg., it looks like that there has been an increase during Q3 compared to the similar time frame last year. What is the reason for that? And what should we expect in terms of cost of manufacturing going forward?”
Steve King: I’ll take a stab at the first piece of this, and then turn it over to Joe to answer the questions on the SUNRISE study, and then Paul on the cost of mfg. question. I think it's important on the PS-exosome diagnostics that this is a simple blood test. And so what we’ve been focusing our efforts on is really refining the assay into a format that would be easily implemented at a number of different sites vs. if you’re just doing it in a research-type setting. And that’s all being really done with internal expertise we already have in-house. As far as validating other tumors, we do believe this really could be a good marker across many different tumor types. So, while the initial effort has been focused on ovarian cancer, we do have an interest in implementing this into all of our future clinical studies as a simple blood collection; so including potentially the NCCN studies, for instance, and other collaborations. But also there are sample sources of serum that we can obtain, as well as working with our collaborators at UTSW and Memorial Sloan Kettering to look at other tumor types. So although our primary interests are breast cancer, lung cancer, and expanding into the other tumor types, liver cancer, which we looked at before, and really validating it across the board, because one of the bigger goals would be if this could potentially be a prognostic for the treatment of bavituximab - we’re a long way from that, but at least we have a tool and we can look at it in the conjunction of the tumors [???]. We think there’s very broad potential for this technology. As far as running any actual clinical studies, our goal is really to bringing the program forward to do the proof-of-concept based on our collaborations and then to find a partner to move forward to be further advancement and take on both the cost of the future development, as well as the commercialization with us receiving some downstream royalties & milestones to most of these types of agreements. For the question regarding patients that are still on bavi and how are they doing, and the Compassionate Use, I’ll turn it over to Joe.
Joe Shan: For SUNRISE overall, while there was no significant difference between the bavituximab+docetaxel arm and the docetaxel alone arm, there are of course patients still as we mentioned still receiving bavituximab, so that gives you an indication that there are patients that are not only, what we call long-term survivors but there are diseases that stabilized. That’s why it's was important that the trial is formally concluded that we allow the patients the opportunity to continue receiving bavituximab under compassionate use. The biomarker analysis is still ongoing, and we’re also hoping to wrap that up in the next few months. Those data will be presented as they’re become available, but the first observation that we’ve reported on already, we mentioned the correlation between beta-2glycoprotein-1 [B2GPI] levels, which is an important protein for bavituximab to bind, so that’s important confirmation of a biomarker for drug activity. And, like I mentioned, there will be a presentation on other cytokine biomarker, interferon gamma [IFN-y], in about 2 weeks time [4-3-17 AACR’17 http://tinyurl.com/zzldh9n ]. Regarding the compassionate use, the procedure varies from country-to-country, but basically, investigators that have patients still receiving bavituximab need to file an IND or expanded access to application in the U.S. It’s a single patient IND, and in Europe it's under the expanded access. It’s a bit of paper work, but we’re assisting where we can, but basically the investigator takes responsibility from that point on, and the approvals are pretty quick.
Steve King: That’s one of the things that we see with bavituximab is, while we’re all disappointed that the overall trial results weren’t what we expected, certainly, you see these anecdotal signs where we obviously see a number of patients that are still on therapy who are then coming in for quite now very long extended period of time, we feel like they’re getting benefit. You see these anecdotal signs activity in those patients that have been on therapy, and for us that’s one of the reasons we’re still very happy and actually excited about the collaborations at Sloan Kettering and UTSW, in particular, where there’s not just an interest in studying bavituximab in preclinical models, but actually taking some of that data and eventually turning that into clinical indications where the drug excels. We look forward to keeping everyone updated on those activities at AACR, ASCO, and beyond. Then the other question on the cost of mfg, I’ll turn it over to Paul.
Paul Lytle: Let me just say the backdrop we’re really excited about Avid, and what we’ve done so far. We have great projections this year hitting $60-65mm in potential revenue. And it's just a phenomenal year that could be anywhere from 35% to 47% increase over the previous FY. Last FY, we did about $44mm in revenue, and that represented about 66% growth over the previous FY. So, as Steve Worsley mentioned, I think this industry is set for a boom, and we're feeling the impact of that and it's great part of the business. On the costing side, as we mentioned on previous calls, our Franklin facility, generally have a higher gross margin, because of the lower cost structure. That particular facility is smaller, it has lower overhead costs, and is running at a higher capacity. Whereas our Myford facility currently is a much larger facility, has a higher cost structure. It absorbs depreciation and also it's not utilized fully right now as we're in the process of doing process validation runs. And these particular runs are done in a series, so they're not done in campaign mode where you can maximize the usage of the facility, and that just causes a higher burden for those runs and higher costs for those runs, causing the gross margins on an overall basis to decline. But as Myford becomes more fully utilized, we expect the margins to get back in place where we’ve seen them before, between the 40% and 48% range. And we think, as Steve Worsley mentioned, there’s the opportunity to get there based on where the industry is going and what the demand is.
----
Apr1-5: AACR 2017, WashDC http://tinyurl.com/zdsbds8 - SUMMARY of PPHM’s 5 AACR’17 ABSTRACTS:
1. MSKCC(Wolchok Lab)+PPHM: 4-2-17/1pm #574, “PSTargeting+RAD+AntiPD1 Promotes Anti-Tumor Activity, Melanoma” (same as SITC'16/11-14-16 http://tinyurl.com/js3fca4 )
2. MSKCC(Wolchok Lab)+PPHM: 4-3-17/8am #1651, “PSTargeting+Adoptive TCell Transfer (ACT) Eliminates Adv. Tumors w/o Off-Target Toxicities, Melanoma” <=NEW(2nd) Joint MemSloan(Wolchok Lab)/PPHM study, see: http://tinyurl.com/h3ylrku
3. PPHM: 4-4-17/8am #3652, “PSTargeting+LAG3+AntiPD1 Significantly Enhances Anti-Tumor Activity, Triple- MBC”
4. IMMUNOVACCINE+PPHM: 4-4-17/8am #3657, ”PSTargeting Enhances Anti-Tumor Activity of a Tumor Vaccine(DepoVax), HPV-Induced Tumor” https://www.imvaccine.com
5. PPHM+VANDERBILT+PRECISIONMEDICINE+PROVIDENCECC: 4-3-17/1pm #CT159/25 (Session: Ph2/3 Clinical Trials in Progress), “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” (abstract embargoed, Sunrise Biomarker #3) – MORE on Biomarkers: http://tinyurl.com/jrenezs
Jun2-6: ASCO 2017, Chicago https://am.asco.org (Abstracts: Titles/MidAPR, Full=May17)
1. Thomas Yip (FBR & Co.): http://www.fbr.com
TY: ”Good to see Avid continuing to grow, with higher revenue guidance. Glad to hear some new progress on exosome program as well. Looking at your new revenue guidance, it looks like the coming Q4 [q/e 4-30-17] will be the big quarter. So, should we expect to see similar seasonality fluctuations from qtr-to-qtr for the next FY’18?”
Paul Lytle: There iare number of variables that go into the revenue recognition. Some of it is driven by the timing of doing runs, and remember that these runs typically from beginning to end, are around 4-5mos time periods. So, you’re going to have the natural variability there as to how many actually started in a given time period that could end in a qtr. The 2nd is, in the past we’ve had some issues, which recently seem to have been resolved with some of the testing labs and the ability to get test results, which impacted lot release and the timing of shipping, and when the clients were ready to accept the material. So given that, there’s going to be some natural variability. Hopefully, as we get the Myford facility really up and running and it converts over into a more consistent flow of business going through there, which we expect over time as some of those process validations turn into commercial production, then hopefully, we’ll have a pretty good level of stabilization. But, by the nature of the business, you’re going to have a little bit of lumpiness. It may be a bit exaggerated between Q3 and Q4, but overall we think as Myford comes into constant production then naturally the number is going to grow, and therefore, the amount of variability we’ll see should decrease. But the key thing is that we’re bringing in new customers and aligning ourselves up for that future business, because that’s where the real value is going to come from.
TY: ”Re: Avid backlog of $70mm, are they selling type contracts or do they have a period of time that you need to fulfill these orders?”
Steve King: We typically get a rolling forecast from our clients, which covers generally 9-15 mo. periods, with a committed period, and then we get a viewpoint of their future business after that. We talk about our backlog, it is all committed business from a number of clients for production that they need. The production schedule then flows off of those projections of when they need the material delivered. We start it months in advance so we’re in a position to deliver it during those quarters in which they projected they need the material.
TY: ”You said the Myford plant expansion will happen in a couple of months, which will put us towards the 1H of FY’18. How should we account for the expansion costs, will they be reflected primarily between now to 1H of FY’18 in COGS or will that be an underlying item?”
Paul Lytle: When we talk about expansion, Thomas, we’re talking about the installation of two 2,000 liter bioreactors which will be installed in our existing Myford facility, and will allow us addl. capacity at a higher scale to meet some of our customers’ demands that are currently adhere the book of business work. And the cost of those bioreactors is nominal compared to the overall cost of facility, and it will be negligible compared to the opportunity that we can generate from those bioreactors.
TY: ”So we shouldn’t project higher costs for the next couple of quarters?”
Paul Lytle: Yes. Correct.
TY: ”Re: Bavi, I don’t see any new NCCN trials for lung cancer. Should we expect future Phase1/2 trials to focus primarily on exploring other solid tumor indications, or do you plan to re-address NSCLC in the future?”
Steve King: The NCCN process is relatively independent from us. It's a competitive process in which the investigators from any of the NCCN institutions can submit their proposals for clinical studies. None of the studies are happening in lung cancer, but that was just part of their overall competitive process. As we’re evaluating and looking at the rest of the data from SUNRISE, which gives us more insight into the lung cancer potential of bavituximab, then we will consider, addl. lung cancer studies in the future. Right now, we’re just evaluating where we’re at and what those studies could potentially look like. But, as has been the overall goal of the Company, which is continue to take control our R&D expenses and to move toward profitability for the next 15mos now. But yes, we still have an interest in lung cancer. It’s obviously a complicated space, maybe getting more complicated with expected approvals and PDUFA dates and what have you coming up that could further change the landscape. The bottom line is there are still patients who are not getting cured. The research community and clinical community is focused on the tumor microenvironment as the potential root cause, and as we have these collaborations that have results coming up at AACR and beyond, they’re indicating that that could be Bavi’s sweet spot. So, as we put together our data set with what the market needs, our lung cancer is still attractive. It’s a huge indication and still lots of need there. While we’re happy to see the great progress in treating those patients, there’s still lot of patients who still need lot more options.
MR. KING’S CLOSING COMMENTS:
I’d like to thank you all again for participating in today’s phone call. As always, I want to thank our stockholders for their continued support, and I would like to especially thank our patients, their families and the investigators that are participating in our bavituximab clinical trials. With that, we will now conclude the call.
= = = = = = = = = = = = = = = = = = = = = = = = = = = = = == = = =
3-13-17/PR: Peregrine Pharmaceuticals Reports Financial Results for 3rd Quarter of FY 2017 and Recent Developments
**Avid Revenue Guidance Increased to $60-65 Million for Full FY 2017 and Contracted Backlog of Future Business Currently at $70 Million
**Multiple Preclinical Studies Demonstrating Bavituximab's Ability to Enhance Activity of Immune Stimulating Therapies Accepted for Presentation at AACR
http://ir.peregrineinc.com/releasedetail.cfm?ReleaseID=1017192
TUSTIN, March 13, 2017: Peregrine Pharmaceuticals, Inc. (NASDAQ:PPHM, PPHMP), a biopharmaceutical company committed to improving patient lives by manufacturing high quality products for biotechnology and pharmaceutical companies, and advancing its proprietary R&D pipeline, today announced financial results for the third quarter of fiscal year (FY) 2017 ended January 31, 2017, and provided an update on its contract manufacturing business, preclinical and clinical pipeline, and other corporate developments.
Highlights Since October 31, 2016
"During the third quarter, Avid's revenue growth continued, which is a strong indicator of the increasing value of this contract development and manufacturing organization (CDMO) business. The steady growth of this business over the past 5 years has been remarkable and we are pleased to see the trend continuing as we move through a number of process validations for clients, which we expect to spur further growth in the future as some or all of those products move to commercialization. We see Avid as a tremendously important asset with solid upside potential that is often overlooked as a value driver for the overall organization. With projected revenue of over $60 million for the current fiscal year, this is already a strong business in an industry that is expecting substantial growth over the next decade and we are excited about the future of the company," stated Steven W. King, President and CEO officer of Peregrine, and President of Avid Bioservices. "An important component of our Avid growth strategy is capacity expansion within our Myford facility. We are currently on track to install two 2,000-liter bioreactors in the facility within the next few months with a book of business for the reactors already in place. We believe the total capacity potential of the facility, when operating in campaign mode, can exceed more than $75 million annually bringing us to well over $100 million in total potential revenue between our two manufacturing facilities, and giving us adequate capacity to continue Avid revenue growth through FY 2018. As we look to the future, based on current operations and projected demand from our existing clients, we have also recently secured additional space within the same building as our Myford facility for which we already have use as part of our existing operations but would also allow us to further expand capacity based on committed business. While we will only begin converting the space into manufacturing capacity once client commitments and other necessary financing is in place, this puts us in an excellent position for continuing to grow the business beyond the coming fiscal year."
Mr. King continued, "During the quarter, we also achieved a number of goals on the development front. These efforts are highlighted by the three clinical trials under our collaboration with the National Comprehensive Cancer Network (NCCN) which are advancing as planned, and we expect at least two of the trials to be initiated by mid-year. Additionally, we and our collaborators will be presenting a number of studies at the upcoming AACR annual meeting [AACR’17: http://tinyurl.com/zaz525l ], including data from researchers at Memorial Sloan Kettering that support the ability of PS-targeting agents, including bavituximab, to significantly impact the tumor microenvironment, creating a more favorable environment for checkpoint inhibitors. Additionally, our collaborators at the University of Texas Southwestern Medical Center published positive proof-of-concept data for our recently-licensed exosome-based cancer detection platform, which could have broad potential for patients with cancer. Even though we have reduced our R&D expenditures, we are pleased that collaborations such as these are allowing us to continue the advancement of our therapeutic and diagnostic programs as we continue to evaluate the best ways for moving our bavituximab and other PS-targeting programs forward. The combined efforts of growing the Avid biomanufacturing business and these important collaborations are allowing us to make great strides on all fronts."
Avid Bioservices Highlights:
"The Avid business continues to build momentum. During the third quarter of FY 2017, contract manufacturing revenue increased 61% to $10.7 million compared to the third quarter of FY 2016. Given this performance, and our expected fourth quarter results, we are increasing our full FY 2017 revenue guidance from $50 to $55 million, to $60 to $65 million," stated Paul Lytle, CFO of Peregrine. "We are also pleased to report that we recently leased 42,000 square feet within the same building as our Myford facility, allowing us to leverage existing oversized utilities and infrastructure that should allow us greater operational efficiency and overall cost savings. While we design the new facility within this new space, it's important to note that our two existing commercial facilities have sufficient capacity to continue to grow our contract manufacturing revenue in FY 2018."
The company is increasing its manufacturing revenue guidance for the full FY 2017 from $50-55 million, to $60-65 million.
Avid's current manufacturing revenue backlog is $70 million, representing estimated future manufacturing revenue to be recognized under committed contracts. This backlog primarily covers revenue to be recognized during the remainder of fiscal year 2017 and fiscal year 2018.
Clinical Development Highlights:
-- The three clinical trials under the collaboration with the NCCN are advancing as planned.
* Moffitt Cancer Center - “A Phase I Trial of Sorafenib and Bavituximab Plus Stereotactic Body Radiation Therapy for Unresectable Hepatitis C Associated Hepatocellular Carcinoma”. This protocol is approved and patient screening is expected soon.
* Massachusetts General Hospital Cancer Center - “Phase I/II Clinical Trial of Bavituximab with Radiation and Temozolomide for Patients with Newly Diagnosed Glioblastoma”. This trial is on track to be initiated by mid-calendar 2017.
* The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins - “Phase II Study of Pembrolizumab and Bavituximab for Progressive Recurrent/Metastatic Squamous Cell Carcinoma of the Head and Neck”. This trial is on track to be initiated by mid-calendar 2017.
-- The company is continuing its comprehensive biomarker analysis of data collected in the Phase III SUNRISE trial [See Biomarkers summary: http://tinyurl.com/jrenezs ].
* Through this analysis, and as reported previously, Peregrine scientists have identified a correlation between overall survival and pre-treatment levels of the biomarker, beta-2 glycoprotein-1 (B2GP1).
* The results of an analysis of pre-treatment interferon gamma (IFN-y) will be the subject of a presentation at AACR entitled: “IFN-y Analysis in Blood and Tissue as a Potential Prognostic and/or Predictive Biomarker”
Research Highlights:
-- Peregrine scientists and collaborators from Memorial Sloan Kettering Cancer Center will present preclinical results from multiple studies at the upcoming AACR meeting in April [AACR’17: http://tinyurl.com/zaz525l ]. Each study evaluates the use of a bavituximab equivalent in combination with immune stimulating therapies. The following abstracts will be presented:
* Memorial Sloan Kettering: Targeting Phosphatidylserine in Combination with Adoptive T Cell Transfer Eliminates Advanced Tumors without Off-Target Toxicities in a Melanoma Preclinical Model
* Memorial Sloan Kettering (initial findings presented at SITC): Phosphatidylserine Targeting Antibody in Combination with Tumor Radiation and Immune Checkpoint Blockade Promotes Anti-Tumor Activity in Mouse B16 Melanoma
* Peregrine (initial findings presented at the 2016 Society for Immunotherapy of Cancer Meeting): Combinational Activity of LAG3 and PD-1 Targeted Therapies is Significantly Enhanced by the Addition of Phosphatidylserine Targeting Antibodies and Establishes an Anti-Tumor Memory Response in Murine Triple Negative Breast Cancer
-- Collaborators from the University of Texas Southwestern Medical Center at Dallas, recently published positive proof-of-concept findings for Peregrine's recently licensed exosome-based cancer detection platform in the peer-reviewed journal, Oncotarget [2-9-17: http://tinyurl.com/jhv57ua Senior Author: Dr. Alan Schroit, PPHM SAB]. Results demonstrated that those patients with malignant ovarian cancer displayed significantly higher blood PS exosome levels than those with benign tumors, and the malignant and benign groups displayed significantly higher blood PS exosome levels than the healthy subjects.
Financial Highlights and Results:
-- Peregrine continues to execute its previously-announced strategy to reach sustained profitability by increasing contract manufacturing revenue while decreasing research and development expenses, with the goal of reaching profitability 15 months from now. During the first nine months of FY 2017, the company made significant progress toward this goal with contract manufacturing revenues increasing 55% compared to the first nine months of FY 2016 and research and development expenses decreasing by 50% compared to the first nine months of FY 2016.
Contract manufacturing revenue from Avid's biomanufacturing services provided to its third-party customers increased to $10,747,000 for the third quarter of FY 2017 compared to $6,672,000 for the third quarter of FY 2016.
Total costs and expenses for the third quarter of FY 2017 were $18,544,000, compared to $23,576,000 for the third quarter of FY 2016. For the third quarter of FY 2017, research and development expenses decreased 60% to $5,989,000, compared to $15,156,000 for the third quarter of FY 2016. Cost of contract manufacturing increased to $7,974,000 in the third quarter of FY 2017 compared to $3,896,000 for the third quarter of FY 2016, primarily due to an increase in the cost of contract manufacturing associated with higher reported revenue. Also contributing to this increase and impacting gross margins for the period is the higher cost of operating the new Myford facility as well as the higher cost associated with performing process validation runs during the quarter. For the third quarter of FY 2017, selling, general and administrative expenses increased slightly to $4,581,000 compared to $4,524,000 for the third quarter of FY 2016 primarily due to the company's growing manufacturing business.
Peregrine's consolidated net loss attributable to common stockholders was $9,216,000 or $0.04 per share, for the third quarter of FY 2017, compared to a net loss attributable to common stockholders of $18,227,000, or $0.08 per share, for the same prior year quarter.
Peregrine reported $41,528,000 in cash and cash equivalents as of January 31, 2017, compared to $61,412,000 at fiscal year ended April 30, 2016.
More detailed financial information and analysis may be found in Peregrine's Quarterly Report on Form 10-Q, which will be filed with the Securities and Exchange Commission today. [ http://tinyurl.com/zlozrv4 ]
CONFERENCE CALL: Peregrine will host a conference call and webcast this afternoon, March 13, 2017, at 4:30 PM EDT (1:30 PM PDT).
To listen to the conference call, please dial (877) 312-5443 or (253) 237-1126 and request the Peregrine Pharmaceuticals conference call. To listen to the live webcast, or access the archived webcast, please visit: http://ir.peregrineinc.com/events.cfm .
ABOUT PEREGRINE PHARMACEUTICALS, INC.
Peregrine Pharmaceuticals, Inc. is a biopharmaceutical company committed to improving the lives of patients by delivering high quality pharmaceutical products through its contract development and manufacturing organization (CDMO) services and through advancing and licensing its investigational immunotherapy and related products. Peregrine's in-house CDMO services, including cGMP manufacturing and development capabilities, are provided through its wholly-owned subsidiary Avid Bioservices, Inc. ( http://www.avidbio.com) , which provides development and biomanufacturing services for both Peregrine and third-party customers. The company is also working to evaluate its lead immunotherapy candidate, bavituximab, in combination with immune stimulating therapies for the treatment of various cancers, and developing its proprietary exosome technology for the detection and monitoring of cancer. For more information, please visit http://www.peregrineinc.com .
ABOUT AVID BIOSERVICES
Avid Bioservices provides a comprehensive range of process development, high quality cGMP clinical and commercial manufacturing services for the biotechnology and biopharmaceutical industries. With over 15 years of experience producing monoclonal antibodies and recombinant proteins in batch, fed-batch and perfusion modes, Avid's services include cGMP clinical and commercial product manufacturing, purification, bulk packaging, stability testing and regulatory strategy, submission and support. The company also provides a variety of process development activities, including cell line development and optimization, cell culture and feed optimization, analytical methods development and product characterization. For more information about Avid, please visit http://www.avidbio.com .
PEREGRINE PHARMACEUTICALS, INC.
CONDENSED CONSOLIDATED STATEMENTS OF OPERATIONS AND COMPREHENSIVE LOSS (UNAUDITED)
THREE MONTHS ENDED
JANUARY 31, NINE MONTHS ENDED
JANUARY 31,
2017 2016 2017 2016
REVENUES:
Contract manufacturing revenue $ 10,747,000 $ 6,672,000 $ 39,726,000 $ 25,574,000
License revenue — 37,000 — 329,000
Total revenues 10,747,000 6,709,000 39,726,000 25,903,000
COSTS AND EXPENSES:
Cost of contract manufacturing 7,974,000 3,896,000 26,477,000 13,245,000
Research and development 5,989,000 15,156,000 21,580,000 43,264,000
Selling, general and administrative 4,581,000 4,524,000 14,625,000 13,839,000
Total costs and expenses 18,544,000 23,576,000 62,682,000 70,348,000
LOSS FROM OPERATIONS (7,797,000 ) (16,867,000 ) (22,956,000 ) (44,445,000 )
OTHER INCOME (EXPENSE):
Interest and other income 25,000 34,000 71,000 691,000
Interest and other expense (2,000 ) (14,000 ) (2,000 ) (14,000 )
Total other income, net 23,000 20,000 69,000 677,000
NET LOSS $ (7,774,000 ) $ (16,847,000 ) $ (22,887,000 ) $ (43,768,000 )
COMPREHENSIVE LOSS $ (7,774,000 ) $ (16,847,000 ) $ (22,887,000 ) $ (43,768,000 )
Series E preferred stock accumulated dividends (1,442,000 ) (1,380,000 ) (3,558,000 ) (3,448,000 )
NET LOSS ATTRIBUTABLE TO COMMON STOCKHOLDERS $ (9,216,000 ) $ (18,227,000 ) $ (26,445,000 ) $ (47,216,000 )
WEIGHTED AVERAGE COMMON SHARES OUTSTANDING:
Basic and Diluted 260,811,553 227,389,225 248,407,470 209,549,670
BASIC AND DILUTED LOSS PER COMMON SHARE $ (0.04 ) $ (0.08 ) $ (0.11 ) $ (0.23 )
PEREGRINE PHARMACEUTICALS, INC.
CONDENSED CONSOLIDATED BALANCE SHEETS
JANUARY 31,
2017 APRIL 30,
2016
Unaudited
ASSETS
CURRENT ASSETS:
Cash and cash equivalents $ 41,528,000 $ 61,412,000
Trade and other receivables 5,883,000 2,859,000
Inventories 33,829,000 16,186,000
Prepaid expenses and other current assets 1,747,000 1,351,000
Total current assets 82,987,000 81,808,000
Property and equipment, net 24,143,000 24,302,000
Restricted cash 600,000 600,000
Other assets 3,587,000 2,333,000
TOTAL ASSETS $ 111,317,000 $ 109,043,000
LIABILITIES AND STOCKHOLDERS' EQUITY
CURRENT LIABILITIES:
Accounts payable $ 7,696,000 $ 8,429,000
Accrued clinical trial and related fees 3,127,000 7,594,000
Accrued payroll and related costs 5,637,000 5,821,000
Deferred revenue 26,367,000 10,030,000
Customer deposits 26,210,000 24,212,000
Other current liabilities 941,000 1,488,000
Total current liabilities 69,978,000 57,574,000
Deferred rent, less current portion 1,325,000 1,395,000
Commitments and contingencies
STOCKHOLDERS' EQUITY:
Preferred stock—$0.001 par value; authorized 5,000,000 shares; 1,647,760 and 1,577,440 issued and outstanding at January 31, 2017 and April 30, 2016, respectively 2,000 2,000
Common stock—$0.001 par value; authorized 500,000,000 shares; 271,068,464 and 236,930,485 issued and outstanding at January 31, 2017 and April 30, 2016, respectively 271,000 237,000
Additional paid-in capital 571,904,000 559,111,000
Accumulated deficit (532,163,000 ) (509,276,000 )
Total stockholders' equity 40,014,000 50,074,000
TOTAL LIABILITIES AND STOCKHOLDERS' EQUITY $ 111,317,000 $ 109,043,000
Safe Harbor *snip*
CONTACTS:
• Stephanie Diaz (Investors) Vida Strategic Partners 415-675-7401 sdiaz@vidasp.com
• Tim Brons (Media) Vida Strategic Partners 415-675-7402 tbrons@vidasp.com
- - - - - - - - -
[From 10-Q header: “As of Mar. 10 2017, there were 297,709,478 shares outstanding.”
- - - - - - - - - - - - - - - - -
Latest 10K 4-30-16 iss. 7-14-16 PR: http://tinyurl.com/h8eqtg5 (Cash 4-30-16=$61.4mm)
Latest 10Q 1-31-17 iss. 3-13-17 http://tinyurl.com/zlozrv4 PR: http://tinyurl.com/grhwjvy (Cash 1-31-17=$41.5mm)
ALL SEC filings for PPHM: http://tinyurl.com/6d4jw8
= = = = = = = = = = = = = = = = = = = = = = = = = = = =
Updated PPHM REVS-BY-QTR TABLE, now thru FY17'Q3(qe 1-31-17), per the 10-Q ( http://tinyurl.com/zlozrv4 ) issued 3-13-17.
• Total Revs since May’06: ($213.3mm/Avid + $24.1mm/Govt + $2.5mm/Lic.) = $239.9mm
• 3-13-17: FY'17 (May'16-Apr'17) Avid revs guidance $60-65mm (Committed B/L=$70mm).
• Deferred-Revs at 1-31-17 total $26.4mm, UP from $18.0mm at 10-31-16.
• Cust.Deposits at 1-31-17 total $26.2mm, DOWN from $26.9mm at 10-31-16.
• Inventories at 1-31-17 total $33.8mm, UP from $25.9mm at 10-31-16.
• Avid’s Gross-Profit over last 4 qtrs: $22.3mm on revs of $58.5mm (GP%=38%)
• Recall, Avid Rev$ from Gov’t DTRA Contract work (6/30/08 – 4/15/11, totaling $24.15mm), went into GOVT-REVS, not AVID-REVS, in the Financials.
Avid’s website: http://www.avidbio.com
AVID PROFITABILITY (GROSS*) BY QTR:
QTR Avid-Rev$ CostofMfg$ Gross-Profit$ GP%
FY13Q1 7-31-12 4,135,000 2,024,000 2,111,000 51%
FY13Q2 10-31-12 6,061,000 3,703,000 2,358,000 39%
FY13Q3 1-31-13 6,961,000 3,651,000 3,310,000 47%
FY13Q4 4-30-13 4,176,000 3,217,000 959,000 23%
FY14Q1 7-31-13 4,581,000 2,670,000 1,911,000 42%
FY14Q2 10-31-13 7,354,000 4,195,000 3,159,000 43%
FY14Q3 1-31-14 3,885,000 2,416,000 1,469,000 38%
FY14Q4 4-30-14 6,474,000 3,829,000 2,645,000 41%
FY15Q1 7-31-14 5,496,000 3,583,000 1,913,000 35%
FY15Q2 10-31-14 6,263,000 4,139,000 2,124,000 34%
FY15Q3 1-31-15 5,677,000 3,113,000 2,564,000 45%
FY15Q4 4-30-15 9,308,000 4,758,000 4,550,000 49%
FY16Q1 7-31-15 9,379,000 4,608,000 4,771,000 51%
FY16Q2 10-31-15 9,523,000 4,741,000 4,782,000 50%
FY16Q3 1-31-16 6,672,000 3,896,000 2,776,000 42%
FY16Q4 4-30-16 18,783,000 9,721,000 9,062,000 48%
FY17Q1 7-31-16 5,609,000 3,062,000 2,547,000 45%
FY17Q2 10-31-16 23,370,000 15,441,000 7,929,000 34%
FY17Q3 1-31-17 10,747,000 7,974,000 2,773,000 26%
FY13 TOTAL: 21,333,000 12,595,000 8,738,000 41%*
FY14 TOTAL: 22,294,000 13,110,000 9,184,000 41%*
FY15 TOTAL: 26,744,000 15,393,000 11,151,000 42%*
FY16 TOTAL: 44,357,000 22,966,000 21,391,000 48%*
*Avid Net-Profit (ie, incl. Selling, G&A) not split out from PPHM-Corp. in the financials.
.
PPHM REVENUES (in thousands) DEFERRED
-------REVENUES------- REVENUES INVEN-
Quarter Avid Govt Lic. TOTAL Avid Govt TORIES
FY07Q1 7-31-06 398 0 23 421 317 0 971
FY07Q2 10-31-06 636 0 48 684 1388 0 1899
FY07Q3 1-31-07 347 0 16 363 2202 0 1325
FY07Q4 4-30-07 2111 0 129 2240 1060 0 1916
FY08Q1 7-31-07 1621 0 4 1625 1820 0 2363
FY08Q2 10-31-07 1863 0 29 1892 1338 0 3500
FY08Q3 1-31-08 1662 0 13 1675 1434 0 2394
FY08Q4 4-30-08 751 0 150 901 2196 0 2900
FY09Q1 7-31-08 1193 324 0 1517 4021 980 4628
FY09Q2 10-31-08 983 958 0 1941 6472 1701 6700
FY09Q3 1-31-09 5778 1048 0 6826 4805 3262 5547
FY09Q4 4-30-09 5009 2683 175 7867 3776 3871 4707
FY10Q1 7-31-09 2070 4671 9 6750 5755 2332 6177
FY10Q2 10-31-09 5308 1510 78 6896 4260 3989 5850
FY10Q3 1-31-10 2945 6854 78 9877 3052 76 3861
FY10Q4 4-30-10 2881 1461 78 4420 2406 78 3123
FY11Q1 7-31-10 983 2111 115 3209 3719 47 4692
FY11Q2 10-31-10 3627 966 78 4671 2447 35 3555
FY11Q3 1-31-11 1922 882 79 2883 4300 40 3915
FY11Q4 4-30-11 1970 681 78 2729 5617 0 5284
FY12Q1 7-31-11 5439 0 216 5655 4145 0 4481
FY12Q2 10-31-11 4154 0 78 4232 2012 0 3178
FY12Q3 1-31-12 3203 0 78 3281 2552 0 2722
FY12Q4 4-30-12 1987 0 78 2065 3651 0 3611
FY13Q1 7-31-12 4135 0 116 4251 6056 0 5744
FY13Q2 10-31-12 6061 0 78 6139 6221 0 5426
FY13Q3 1-31-13 6961 0 78 7039 5061 0 4635
FY13Q4 4-30-13 4176 0 78 4254 4171 0 4339
FY14Q1 7-31-13 4581 0 107 4688 4164 0 5679
FY14Q2 10-31-13 7354 0 0 7354 3468 0 4033
FY14Q3 1-31-14 3885 0 0 3885 4329 0 5224
FY14Q4 4-30-14 6474 0 0 6474 5241 0 5530
FY15Q1 7-31-14 5496 0 0 5496 4670 0 5998
FY15Q2 10-31-14 6263 0 37 6300 3612 0 5379
FY15Q3 1-31-15 5677 0 0 5677 5752 0 6148
FY15Q4 4-30-15 9308 0 0 9308 6630 0 6148
FY16Q1 7-31-15 9379 0 292 9671 8291 0 10457
FY16Q2 10-31-15 9523 0 0 9523 9688 0 12554
FY16Q3 1-31-16 6672 0 37 6709 15418 0 15189
FY16Q4 4-30-16 18783 0 0 18783 15418 0 15189
FY17Q1 7-31-16 5609 0 0 5609 21531 0 25274
FY17Q2 10-31-16 23370 0 0 23370 21531 0 25274
FY17Q3 1-31-17 10747 0 0 10747 26367 0 33829
Totals: 213295 24149 2453 239897 <=since5/1/2006
.
TOTAL REV’s BY YEAR (Avid+Gov’t+Lic):
FY04 4-30-04 3,314 …Avid(CMO)= 3,039 (Avid-Revs don’t incl. Govt-SVCS)
FY05 4-30-05 4,959 …Avid(CMO)= 4,684
FY06 4-30-06 3,193 …Avid(CMO)= 3,005
FY07 4-30-07 3,708 …Avid(CMO)= 3,492
FY08 4-30-08 6,093 …Avid(CMO)= 5,897
FY09 4-30-09 18,151 …Avid(CMO)= 12,963
FY10 4-30-10 27,943 …Avid(CMO)= 13,204
FY11 4-30-11 13,492 …Avid(CMO)= 8,502
FY12 4-30-12 15,233 …Avid(CMO)= 14,783
FY13 4-30-13 21,683 …Avid(CMO)= 21,333
FY14 4-30-14 22,401 …Avid(CMO)= 22,294
FY15 4-30-15 26,781 …Avid(CMO)= 26,744
FY16 4-30-16 44,686 …Avid(CMO)= 44,357
...Total Gov’t Revs from 7-2008 inception thru FY11Q1(Apr’11): $24.15mm
.
PPHM’S QTLY. NET LOSS BY QTR:
FY08Q1 7-31-07 4,656,000
FY08Q2 10-31-07 6,207,000
FY08Q3 1-31-08 6,154,000
FY08Q4 4-30-08 6,159,000
FY09Q1 7-31-08 5,086,000
FY09Q2 10-31-08 4,497,000
FY09Q3 1-31-09 3,332,000
FY09Q4 4-30-09 3,609,000
FY10Q1 7-31-09 2,428,000
FY10Q2 10-31-09 2,787,000
FY10Q3 1-31-10 1,538,000
FY10Q4 4-30-10 7,741,000
FY11Q1 7-31-10 7,695,000
FY11Q2 10-31-10 7,513,000
FY11Q3 1-31-11 8,929,000
FY11Q4 4-30-11 10,014,000
FY12Q1 7-31-11 8,092,000
FY12Q2 10-31-11 12,055,000
FY12Q3 1-31-12 11,090,000
FY12Q4 4-30-12 10,882,000
FY13Q1 7-31-12 7,664,000
FY13Q2 10-31-12 8,753,000
FY13Q3 1-31-13 4,914,000
FY13Q4 4-30-13 8,449,000
FY14Q1 7-31-13 7,600,000
FY14Q2 10-31-13 7,790,000
FY14Q3 1-31-14 9,724,000
FY14Q4 4-30-14 10,248,000
FY15Q1 7-31-14 13,129,000
FY15Q2 10-31-14 12,100,000
FY15Q3 1-31-15 12,994,000
FY15Q4 4-30-15 12,135,000
FY16Q1 7-31-15 13,723,000
FY16Q2 10-31-15 13,198,000
FY16Q3 1-31-16 16,847,000
FY16Q4 4-30-16 11,884,000
FY17Q1 7-31-16 11,057,000
FY17Q2 10-31-16 4,056,000
FY17Q3 1-31-17 7,774,000
= = = = = = = =
OPER. CASH BURNS* BY QTR(FROM THE 10-Q/K’S):
FY10Q1 7-31-09 2,024,000 (from 10Q pg.25)
FY10Q2 10-31-09 2,351,000 (Q1+Q2: 4,375,000 pg.28)
FY10Q3 1-31-10 1,158,000 (Q1+Q2+Q3: 5,533,000 pg.30)
FY10Q4 4-30-10 6,375,000 (FY’10: 11,908,000 10K pg.58)
FY11Q1 7-31-10 6,567,000 (from 10Q pg.24)
FY11Q2 10-31-10 6,167,000 (Q1+Q2: $12,734,000 pg.25)
FY11Q3 1-31-11 7,736,000 (Q1+Q2+Q3: $20,470,000 pg.26)
FY11Q4 4-30-11 8,961,000 (FY’11: 29,431,000 10K pg.54)
FY12Q1 7-31-11 6,984,000 (from 10Q pg.25)
FY12Q2 10-31-11 11,668,000 (Q1+Q2: 18,652,000 pg.25)
FY12Q3 1-31-12 8,490,000 (Q1+Q2+Q3: 27,142,000 pg.25)
FY12Q4 4-30-12 11,265,000 (FY’12: 38,407,000 10K pg.55)
FY13Q1 7-31-12 6,742,000 (from 10Q pg.21)
FY13Q2 10-31-12 6,162,000 (Q1+Q2: 12,904,000 pg.23)
FY13Q3 1-31-13 3,597,000 (Q1+Q2+Q3: 16,501,000 pg.23)
FY13Q4 4-30-13 7,053,000 (FY’13: 23,554,000 10K pg.60)
FY14Q1 7-31-13 5,750,000 (from 10Q pg.23)
FY14Q2 10-31-13 5,834,000 (Q1+Q2: 11,584,000 10Q pg.24)
FY14Q3 1-31-14 7,875,000 (Q1+Q2+Q3: 19,459,000 10Q pg.26)
FY14Q4 4-30-14 8,706,000 (FY’14: 28,165,000 10K pg.55)
FY15Q1 7-31-14 11,076,000 (from 10Q pg.23)
FY15Q2 10-31-14 9,947,000 (Q1+Q2: 21,023,000 10Q pg.25)
FY15Q3 1-31-15 11,116,000 (Q1+Q2+Q3: 32,139,000 10Q pg.26)
FY15Q4 4-30-15 10,474,000 (FY’15: 42,613,000 10K pg.54)
FY16Q1 7-31-15 12,306,000 (from 10Q pg.25)
FY16Q2 10-31-15 11,701,000 (Q1+Q2: 24,007,000 10Q pg.26)
FY16Q3 1-31-16 15,086,000 (Q1+Q2+Q3: 39,093,000 10Q pg.27)
FY16Q4 4-30-16 10,112,000 (FY'16: 49,205,000 10K pg.39)
FY17Q1 7-31-16 9,607,000 (from 10Q pg.22)
FY17Q2 10-31-16 2,565,000 (Q1+Q2: 12,172,000 10Q pg.24)
FY17Q3 1-31-17 6,274,000 (Q1+Q2+Q3: 18,446,000 10Q pg.24)
FY’09 total Op-Burn: $14,715,000
FY’10 total Op-Burn: $11,908,000
FY’11 total Op-Burn: $29,431,000
FY’12 total Op-Burn: $38,407,000
FY’13 total Op-Burn: $23,554,000
FY’14 total Op-Burn: $28,165,000
FY’15 total Op-Burn: $42,613,000
FY’16 total Op-Burn: $49,205,000
Period Halozyme Cust-A Other-Custs
FYE 4-30-14 91% 1% 8%
FYE 4-30-15 79% 12% 9%
FYE 4-30-16 69% 26% 5%
Q/E 7-31-16 65% 29% 6%
Q/E 10-31-16 77% 10% 13%
Q/E 1-31-17 29% 56% 15%
O/S Shares & ATM Sales History (’06–curr.)
PPHM - O/S Shares History (’06–curr.)
4-30-06 35,876,438
1-31-07 39,222,440
4-30-07 39,222,440
7-6-07 45,233,123
7-31-07 45,242,123
10-31-07 45,242,123
1-31-08 45,242,123
4-30-08 45,242,123
7-31-08 45,242,123
10-31-08 45,242,123
1-31-09 45,242,123
4-30-09 45,537,711
7-10-09 47,392,883
7-31-09 47,393,783
10-31-09 48,869,563 +1,475,780
1-31-10 50,903,404 +2,033,841
4-30-10 53,094,894 +2,191,490
6-21-10 54,388,917 +1,294,023 (6-22-10 ATM/mlv Form424)
7-9-10 55,069,449 +475,987 (4-30-10 10K iss. 7-14-10)
7-31-10 55,784,955 +715,506
10-31-10 59,220,742 +3,435,787
11-30-10 63,932,353 +4,711,611 (10-31-10 10Q iss. 12-9-10)
12-15-10 64,404,097 +471,744 (12-17-10 S-3: $75M Shelf Reg.)
1-31-11 66,813,419 +2,409,322
2-28-11 67,885,811 +1,072,392 (1-31-11 10Q iss. 3-11-11)
4-30-11 69,837,142 +1,951,331
7-8-11 71,069,858 +1,232,716 (4-30-11 10K iss. 7-14-11)
8-22-11 72,704,647 +1,634,789 (Proxy iss. 8-26-11)
8-31-11 73,284,016 +579,369 (424B5 iss. 9-2-11)
9-8-11 79,536,268 +6,252,252 (Roth Sale to 3 Inst’s @ $1.11/sh.)
10-31-11 82,638,201 +3,101,933
12-9-11 86,788,817 +4,150,616 (10-31-11 10Q iss. 12-12-11)
1-31-12 93,146,226 +6,357,409
2-29-12 98,873,172 +5,726,946 (1-31-12 10Q iss. 3-9-12)
4-30-12 101,421,365 +2,548,193
7-13-12 104,174,056 +2,752,691 (4-30-12 10K iss. 7-16-12)
7-31-12 104,178,431 +4,375 (7-31-12 10Q iss. 9-10-12)
8-16-12 104,191,176 +12,745 (prelim. proxy 14A http://tinyurl.com/c48bvof )
9-7-12 104,191,176 nochg (7-31-12 10Q iss. 9-10-12)
10-31-12 123,310,188 +19,119,012
12-7-12 132,539,783 +9,229,595 (10-31-12 10Q iss. 12-10-12)
1-31-13 133,770,614 +1,230,831
3-12-13 137,110,758 +3,340,144 (1-31-13 10Q iss. 3-12-13)
4-30-13 143,768,946 +6,658,188 (4-30-13 10K iss. 7-11-13)
7-5-13 151,602,765 +7,833,819 (4-30-13 10K iss. 7-11-13)
7-31-13 153,506,811 +1,904,046
9-5-13 156,461,114 +2,954,303 (7-31-13 10K iss. 9-9-13)
10-31-13 160,248,742 +3,781,628
12-6-13 160,325,891 +77,149 (10-31-13 10K iss. 12-10-13)
1-31-14 176,453,261 +16,127,370
3-3-14 176,481,054 +27,793 (1-31-14 10Q iss. 3-7-14)
4-30-14: 178,871,164 +2,390,110
7-7-14: 179,209,458 +338,294 (4-30-14 10-K cover page, iss. 7-14-14)
7-31-14: 179,216,032 +6,574 (7-31-14 10Q iss. 9-9-14)
8-22-14: 179,226,424 +10,392 (8-28-14 Proxy/Def14A)
9-5-14: 179,505,424 +279,000 (7-31-14 10Q iss. 9-9-14)
10-31-14: 182,000,583 +2,495,159 (10-31-14 10Q iss. 12-10-14)
12-5-14: 182,081,234 +80,651 (10-31-14 10Q cover pg., iss. 12-10-14)
12-19-14: 182,081,234 -0- (12-23-14 S-3)
1-31-15: 184,244,698 +2,163,464 (1-31-15 10Q iss. 3-12-15)
3-12-15: 188,332,872 +4,088,174 (“ “ “)
4-30-15: 193,346,627 +5,013,755 (4-30-15 10-K iss. 7-14-15)
7-10-15: 199,934,918 +6,588,291 (4-30-15 10-K/cover-pg, iss. 7-14-15)
7-31-15: 200,983,948 +1,049,030 (7-31-15 10Q iss. 9-9-15)
9-4-15: 202,124,031 +1,140,083 (“ “ “)
10-31-15: 225,824,551 +23,700,520 (10-31-15 10Q iss. 12-10-15)<=Incl. 18.5mm sh. Dart/EastCAP @1.08
12-9-15: 229,701,808 +3,877,257 (10-31-15 10Q iss. 12-10-15)
1-31-16: 232,231,242 +2,529,434 (1-31-16 10Q iss. 3-9-16)
3-8-16: 233,738,426 +1,507,184 (“ “ “)
4-30-16: 236,930,485 +3,192,059 (4-30-16 10K iss. 7-14-16)
7-11-16: 241,456,721 +4,526,236 (“ “ “)
7-31-16: 241,456,721 -0- (7-31-16 10Q iss. 9-8-16)
9-2-16: 242,381,850 +925,129 (“ “ “)
10-31-16: 251,765,279 +9,383,429 (10-31-16 10Q iss. 12-12-16)
12-8-16: 257,141,534 +5,376,255 (“ “ “)
1-31-17: 271,068,464 +13,926,930 (1-31-17 10Q iss. 3-13-17)
3-10-17: 297,709,478 +26,641,014 (“ “ “)
= = = = = = = = = = = = = = = = = =
ATM Sales Summary (3/2009–3/13/2017). Also, PPHM O/S Shares History Table (’06–curr.) at the bottom of this post. At 3-10-17, common shares O/S = 297,709,478sh.
ATM = “At-The-Market Sales Issuance”
I. WM-SMITH 3-2009:
• $7.5mm ATM/Wm.SMITH 3-26-09: $7,500,000gr. / 2,150,759sh. = $3.49/sh. (commiss: 3%)
• $25mm ATM/Wm.SMITH 7-14-09: $25,000,000gr. / 7,569,314sh. = $3.30/sh. (commiss: 3%/1st$15mm, then 2%)
*Total Raised via WmSmith ATM Sales thru 7-31-10:
. . . . $32,500,000gr. / 9,720,073sh. = $3.34/sh.
II. MLV 6-2010: http://www.mlvco.com
$15mm ATM/MLV 6-22-10 (commiss: 2%) Form424: http://tinyurl.com/24txkxb
• Sold 6/22/10–10/31/10: $6,840,000gr. / 4,031,018sh. = $1.70/sh.
• Sold 11/1/10–11/30/10: $7,407,000gr. / 4,711,611sh. = $1.57/sh.
• Sold 12/1/10–1/31/11: $753,000gr. / 471,744sh. = $1.60/sh.
*Total Raised via MLV June’10 ATM Sales thru 1-31-11:
. . . . $15,000,000gr. / 9,214,373 = $1.63/sh.
III. MLV 12-2010: “Dec’10 AMI Agreement” http://www.mlvco.com
$75mm ATM/MLV 12-29-10 (commiss: max=5%) Form8K: http://tinyurl.com/2a6w76g
(pursuant to $75mm S-3 Shelf Reg. filed 12-17-10: http://tinyurl.com/2469b2d )
• Sold 12/29/10-1/31/11: $6,460,000gr. / 2,385,862sh. = $2.71/sh.
• Sold 2/1/11-2/28/11: $2,358,000gr. / 998,142sh. = $2.36/sh.
• Sold 3/1/11-4/30/11: $4,470,000gr. / 1,840,487sh. = $2.43/sh.
• Sold 5/1/11-7/31/11: $3,713,000gr. / 1,912,576sh. = $1.94/sh.
• Sold 8/1/11-10/31/11: $5,582,000gr. / 4,727,840sh. = $1.18/sh.
• Sold 9-2-12 Roth Direct: $6,940,000gr./ 6,252,252sh. = $1.11/sh.
• Sold 11/1/11-1/31/12: $10,961,000gr. / 10,308,025sh. = $1.06/sh.
• Sold 2/1/12-2/29/12: $5,871,000gr. / 5,726,946sh. = $1.03/sh.
• Sold 3/1/12-4/30/12: $1,263,000gr. / 2,198,543sh. = $.57/sh.
• Sold 5/1/12-6/30/12: $1,496,000gr. / 2,752,691sh. = $.54/sh.
• Sold 7/1/12-9/26/12: none**
• Sold 9/27/12-10/31/12: $16,719,000gr./ 18,557,928 = $.90/sh.
• Sold 11/1/12-11/30/12: $7,296,000gr./ 9,220,313 = $.79
• Sold 12/1/12-1/31/13: $1,540,000gr./ 1,131,282 = $1.36
• Sold 2/1/13-3/12/13: $330,000gr./ 201,154 = $1.64
*Total Raised via MLV Dec’10 ATM Sales thru 3-12-2013:
. . . . $75,000,000gr. / 68,214,041 = $1.10sh.
IV. MLV 12-2012: “Dec’12 AMI Agreement” http://www.mlvco.com
$75mm ATM/MLV 12-29-12 (commiss: max=5%) Form8K: http://tinyurl.com/2a6w76g
(pursuant to $75mm S-3 Shelf Reg. filed 3-9-12: http://tinyurl.com/7dl7pjm )
• Sold 2/1/13-3/12/13: $4,475,000gr. / 3,132,402sh. = $1.43/sh.
• Sold 3/13/13-4/30/13: $8,897,000gr. / 6,188,273sh. = $1.44/sh.
• Sold 5/1/13-7/11/13: $12,729,000gr. / 7,927,016sh. = $1.61/sh.
• Sold 7/12/13-7/31/13: $2,468,000gr. / 1,690,864sh. = $1.46/sh.
• Sold 8/1/13-9/9/13: $4,372,000gr. / 3,057,431sh. = $1.43/sh.
• Sold 9/10/13-10/31/13: $4,708,000gr. / 3,262,958sh. = $1.44/sh.
• Sold 11/1/13-12/6/13: NONE – see 10Q note below.
• Sold 12/7/13-1/31/14: $28,130,000gr. / 16,045,717sh. = $1.75/sh.
• Sold 2/1/14-4/30/14: $3,017,000gr. / 1,543,383sh. = $1.95/sh.
• Sold 5/1/14-7/31/14: $425,000gr. / 226,700sh. = $1.92/sh.
• Sold 8/1/14-10/31/14: $3,891,000gr. / 2,494,835sh. = $1.56/sh.
• Sold 11/1/14-1/31/15: $1,878,000gr. / 1,261,825sh. = $1.49/sh.
*Total Raised via MLV Dec’12 ATM Sales thru 10-31-2014:
. . . . $75,000,000gr. / 46,831,404 = $1.60sh.
V. MLV 6-2014: “Jun’14 AMI Agreement – up to $25mm” http://www.mlvco.com
• Sold 11/1/14-1/31/15: $1,193,000gr. / 869,504sh. = $1.43/sh.
• Sold 2/1/15-3/12/15: $6,204,000gr. / 4,354,954sh. = $1.44/sh.
• Sold 3/13/15-4/30/15: $6,147,000gr. / 4,457,299sh. = $1.38/sh.
• Sold 5/1/15-7/14/15: $8,896,000gr. / 6,534,400sh. = $1.36/sh.
• Sold 7/15/15-7/31/15: $1,270,000gr. / 1,003,830sh. = $1.27/sh.
• Sold 8/1/15-9/9/15: $1,290,000gr. / 1,091,508sh. = $1.18/sh.
*Total Raised via MLV Jun’14 ATM Sales thru 9-9-2015:
. . . . $25,000,000gr. / 18,311,495 = $1.37/sh.
VI. MLV 8-2015: “Aug’15 AMI Agreement – up to $30mm” http://www.mlvco.com
• Sold 8/7/15-9/9/15: $892,000gr. / 1,091,000sh. = $1.18/sh.
• Sold 9/10/15-10/31/15: $4,294,000gr. / 4,059,478sh. = $1.06/sh.
• Sold 11/1/15-12/10/15: $2,261,000gr. / 1,939,413sh. = $1.17/sh.
• Sold 12/11/15-1/31/16: *NO ATM SALES*, per 1-31-16 10Q iss. 3-9-16
• Sold 2/2/16-4/30/16: *NO ATM SALES*, per 4-30-16 10Q iss. 7-14-16
• Sold 5/1/16-7/14/16: $937,000gr. / 1,876,918sh. = $.50/sh.
• Sold 7/15/16-9/8/16: *NO ATM SALES*, per 7-31-16 10Q iss. 9-8-16
• Sold 9/9/16-10/31/16: $2,513,000gr. / 6,432,439sh. = $.39/sh.
• Sold 11/1/16-12/12/16: $1,174,000gr. / 3,788,346sh. = $.31/sh.
• Sold 12/13/16-1/31/17: $3,404,000gr. / 11,069,646sh. = $.31/sh.
• Sold 2/1/17-3/13/17: $7,335,000gr. / 15,308,300sh. = $.48/sh.
. . . . $22,810,000gr. / 45,227,300 = $.50/sh.
VII. NOBLE 8-2015: “Aug’15 Eq.Dist. Agreement – up to $20mm” http://www.noblelsp.com
• Sold 11/1/15-12/10/16: $2,371,000gr. / 1,925,844sh. = $1.23/sh.
• Sold 12/11/15-1/31/16: $2,857,000gr. / 2,529,434sh. = $1.13/sh.
• Sold 2/1/16-4/30/16: $1,741,000gr. / 4,017,010sh. = $.43/sh.
• Sold 5/1/16-7/14/16: $1,233,000gr. / 2,649,318sh. = $.47/sh.
• Sold 7/15/16-9/8/16: *NO ATM SALES*, per 7-31-16 10Q iss. 9-8-16
• Sold 9/9/16-10/31/16: $1,283,000gr. / 2,988,086sh. = $.43/sh.
• Sold 11/1/16-12/12/16: $496,000gr. / 1,587,909sh. = $.31/sh.
• Sold 12/13/16-1/31/17: $904,000gr. / 2,857,284sh. = $.32/sh.
• Sold 2/1/17-3/13/17: $6,006,000gr. / 11,273,296sh. = $.53/sh.
. . . . $16,891,000gr. / 29,828,181 = $.57/sh. '
TOTAL ALL A-T-M SALES – INCEPTION (3-2009) THRU 12-12-2016:
==> $262,201,000gr. / 227,346,867sh. = $1.15/sh.
= = = = = = = = = = = = = = = = = =
O/S WARRANTS & STOCK-OPTIONS A/O 1-31-2017 (10Q pg.13-14):
• WARRANTS: As of 10-31-2016, warrants to purchase 273,280 shares at an exercise price of $2.47 were outstanding and are exercisable through Aug30 2018. These warrants were issued in FY’13 in connection with the Aug.2012 [Oxford] loan agreement, which was paid in full Sept.2012.
• STOCK OPTIONS OUTSTANDING A/O 1-31-2017: 29,467,870 shares at a wgt.avg. exercise price of $1.26.
***3-9-17: Ronin Cap+SWIM Partners (John Stafford+Stephen White*) acquire 9.4% stake (24,308,415sh.) in PPHM (via 13D’s)
...3-1-17: Ronin/17,565,843 + SWIM/3,494,166 = 21,060,009sh. 8.2% http://tinyurl.com/jr42u23 (13D)
...3-9-17: Ronin/20,814,248 + SWIM/3,494,166 = 24,308,415sh. 9.4% http://tinyurl.com/huundwu (13D)
…...NOTES: As a Group, ie, “people that share the furtherance of a common objective/concerted action”. 13D’s are reserved for ACTIVE INVESTORS who may be “interested in agitating for some kind of a change at the company”. See John Stafford/XENCOR BOD(18yrs service): http://tinyurl.com/hcmsv8p
- - - - - - - - - - - - - - - - -
Latest 10K 4-30-16 iss. 7-14-16 http://tinyurl.com/zgognwz PR: http://tinyurl.com/h8eqtg5 (Cash 4-30-16=$61.4mm)
Latest 10Q 1-31-17 iss. 3-13-17 http://tinyurl.com/zlozrv4 PR: http://ir.peregrineinc.com/releasedetail.cfm?ReleaseID=1017192 (Cash 1-31-17=$41.5mm)
ALL SEC filings for PPHM: http://tinyurl.com/6d4jw8
- - - - - - - - - -
10-31-11 10Q: “During the 6mos. 10-31-11, we sold 6,440,416 shares of our common stock at mkt-prices for gross proceeds of $9,295,000 under the Dec’10 AMI Agreement before deducting commissions and other issuance costs of $260,000”
1-31-12 10Q: “During the 9mos. ended 1-31-12, we sold 16,948,441 shares of our common stock at mkt-prices for gross proceeds of $20,256,000 under the Dec’10 AMI Agreement before deducting commissions and other issuance costs of $482,000. …During Feb.2012, we sold an addl. 5,726,946 shares of common stock at market prices under the Dec’10 AMI Agreement in exchange for aggregate gross proceeds of $5,871,000. As of 2-29-12, gross proceeds of $38,644,000 remained available under our 2 effective shelf registration statements.”
4-30-12 10K: “Under the Dec. 2010 AMI Agreement with MLV …for aggregate gross proceeds of up to $75,000,000… During FY’s 2011 (5’10-4’11) and 2012 (5’11-4’12), we sold 30,098,421 shares of common stock at market prices under the Dec.2010 AMI for aggregate gross proceeds of $40,678,000 before deducting commissions & other issuance costs of $917,000. As of April 30, 2012, aggregate gross proceeds of up to $27,382,000 remained available under the Dec.2010 AMI… Subsequent to April 30, 2012 and through June 30, 2012, we sold 2,752,691 shares of common stock at mkt prices under the Dec.2010 AMI for aggregate gross proceeds of $1,496,000… Under the registered direct public offering dated Sept. 2, 2011, we entered into separate subscription agreements with 3 institutional investors, pursuant to which we sold an aggregate of 6,252,252 shares of our common stock at a purchase price of $1.11/sh. for gross proceeds of $6,940,000 before deducting placement agent fees and other offering expenses of $525,000.”
10-31-12 10Q: “During the 6mos. 10-31-12, we sold 21,310,619 shares… at varying mkt-prices under the Dec’10 AMI Agreement for gross proceeds of $18,215,000 before deducting commissions and other issuance costs of $620,000. From 11-1-12 thru 11-30-12, we sold 9,220,313 shares gross of $7,296,000. As of 11-30-12, aggregate gross proceeds of up to $1,871,000 remained available under the Dec’10 AMI Agreement. As of 11-30-12, gross proceeds of $151,871,000 remained available under 2 effective shelf registration statements.”
1-31-13 10Q/pg.11: “DEC’10-AMI(max=$75mm): During the 9 mos. ended 1-31-13, we sold 31,662,214 shares at varying mkt-prices for gross proceeds of $27,051,000 before deducting commissions/other-costs of $885,000. As of 1-31-13, gross proceeds of up to $330,000 remained available. From 2-1-13 – 3-12-13, we sold 201,154 shares at mkt prices for gross $330,000. As of 3-12-13, we had raised the full amt of gross proceeds available… DEC’12-AMI(max=$75mm): As of 1-31-13, we had not sold any shares. From 2-1-13 - 3-12-13, we sold 3,132,402 shares at mkt prices for gross proceeds of $4,475,000. As of 3-12-13, gross proceeds of up to $70,525,000 remained available.”
4-30-13 10K/pg.F26: Dec’12-AMI(max=$75mm)Agreement – During FY’13, we sold 9,320,675 shares gross proceeds of $13,372,000 before deducting commissions and other issuance costs of $337,000. As of April 30, 2013, gross proceeds of up to $61,628,000 remained available under the Dec’12-AMI. From 5/1/13 – 7/11/13, we sold 7,927,016 shares for gross proceeds of $12,729,000. As of 7-11-13, gross proceeds of $48,899,000 remained available under the Dec’12-AMI. http://tinyurl.com/p58jcbw
7-31-13 10Q/pg.10: During the 3mos ended 7-31-13, we sold 9,617,880 shares at mkt prices under the Dec’12 AMI Agreement for gross proceeds of $15,197,000 before deducting commissions and other issuance costs of $491,000. As of July 31, 2013, gross proceeds of up to $46,431,000 remained available under the Dec’12-AMI. From 8-1-13 – 9-9-13, we sold 3,057,431 shares for gross proceeds of $4,372,000. As of 9-9-13, gross proceeds of $42,059,000 remained available under the Dec’12-AMI.
10-31-13 10Q/pg.10: During the 6mos ended 10-31-13, we sold 15,938,269 at mkt prices under the Dec’12 AMI for gross proceeds of $24,277,000 before deducting costs of $722,000. As of 10-31-13, aggregate gross proceeds of up to $37,351,000 remained available under the Dec’12 AMI.
***NOTE: There is no stmt in the 10-Q regarding AMI Sales subsequent to 10-31-13 (thru 12-6-13) as has been the case in the 10Q’s for years – the assumption being: NO AMI Sales made 11/1/13-12/6/13, a period where O/S shares only went up by 77,149.
1-31-14 10Q/pg.11: During the 9 mos. ended 1-31-14, we sold 31,983,986 shares under the Dec’12/AMI for gross $52,407,000 before deducting commissions & other iss. costs of $1,427,000. As of 1-31-14, gross proceeds of up to $9,221,000 remained available under the Dec’12/AMI. http://tinyurl.com/pxcjocw
4-30-14 10K pg.F25: “During FY14, we sold 33,527,369 shares under the Dec’12/AMI for gross proceeds of $55,424,000 before deducting commissions & other iss. costs of $1,504,000. As of April 30, 2014, aggregate gross proceeds of up to $6,204,000 remained available under the December 2012 AMI Agreement.” http://tinyurl.com/mhva3k3
7-31-14 10Q/Pg5: During the 3mos. ended 7-31-14, we raised $10,000,000 in aggregate gross proceeds from the sale of our 10.50% SeriesE Convertible Preferred Stock under an At Market Issuance Sales Agreement. Pg.11: During the 3mos. ended 7-31-14, we sold 226,700sh. under the Dec’12-2012 AMI Agreement for gross of $435,000 before deducting commissions & other costs of $14,000. As of 7-31-14, gross of up to $5,769,000 remained available under the Dec’12-2012/AMI. On 6-13-14, we entered into an At Market Issuance Sales Agreement (“June2014/AMI”), with MLV, pursuant to which we may sell shares of our common stock through MLV, for aggregate gross proceeds of up to $25,000,000, in registered transactions from our shelf registration statement on Form S-3. As of 7-31-14, we had not sold any shares of common stock under the June 2014 AMI Agreement. http://tinyurl.com/phw6dkp
10-31-14 10Q/Pg12: COMMON: During 6mos. ended 10-31-14, we sold 2,721,535 sh. at mkt prices under the Dec’12-AMI for gross proceeds of $4,326,000 before deducting commissions and other issuance costs of $113,000. As of 12-31-14, gross proceeds of up to $1,878,000 remained available under the Dec’12-AMI. PREFERRED: During 6mos. ended 10-31-14, we sold 402,858 sh. at mkt prices gross proceeds of $10,070,000 before deducting commission and other issuance costs of $552,000. As of 10-31-14, gross proceeds of up to $19,930,000 remained available under the Series E AMI Agreement. http://tinyurl.com/m6ldhg7
1-31-15 10Q/Pg12: COMMON: During the 9mos. ended 1-31-15, we sold 3,983,360 sh. at mkt prices under the Dec’12-AMI for gross proceeds of $6,204,000 before deducting commissions and other issuance costs of $162,000. As of 1-31-15, we had raised the full-amt of gross proceeds available to us under the Dec’12-AMI. PREFERRED:
Jun’14-AMI: On 6-13-14, we entered into an AMI with MLV…up to $25mm… ,000,000, in registered transactions from our shelf registration statement on Form S-3 (File No. 333-180028). During the 9mos. ended 1-31-15, we sold 869,504 sh. at mkt prices under the Jun’14-AMI for gross of $1,193,000 before deducting commissions and other issuance costs of $31,000. As of 1-31-15, gross proceeds of up to $23,807,000 remained available. Subsequent to 1-15-15 and thru 3-12-15, we sold 4,354,954 sh. of common at mkt prices under the Jun’14-AMI for gross of $6,204,000. As of 3-12-15, 2015, gross proceeds of $17,603,000 remained available under the Jun’14-AMI.
PREFERRED: During the 9mos. ended 1-31-15, we sold 405,004 sh. of our Series E Preferred Stock at mkt prices under the Series E AMI Agreement for gross proceeds of $10,121,000 before deducting commission and other issuance costs of $553,000. As of 1-31-15, 2015, gross proceeds of up to $19,879,000 remained available under the Series E AMI. http://tinyurl.com/mwedt8w
4-30-15 10K pg.F25: During FY’15 we sold 9,681,757sh. under the June’14/AMI for $13,544,000, before deducting costs of $352,000. As of 4-30-15, $11,456,000 remained available. Pg.F35: Subsequent to 4-30-15 & thru 7-14-15, we sold 6,534,400sh. for $8,896,000. A/o 7-14-15, $2,560,000 remain. http://tinyurl.com/ocrtkuj
7-31-15 10Q/Pg12+18: During the 3mos ended 7-31-15, we sold 7,538,230sh. Under the JUNE2014 AMI for gross of $10,166,000 before deducting commiss/iss-costs of $275,000. As of 7-31-15, gross of $1,290,000 remained available under the JUNE2014 AMI, as amended. JUNE2014 AMI: subsequent to 7-31-15 and thru 9-9-15, we sold 1,091,508sh. gross of $1,290,000. As of 9-9-15, 2015, we had raised the full amount available under the June2014 AMI. AUG2015 AMI: on 8-7-15, we entered into an At Market Issuance Sales Agreement with MLV, for gross proceeds of up to $30,000,000, 2.5% commission; as of 9-9-15, we sold 752,760sh. under the AUG2015 AMI for gross of $892,000. http://tinyurl.com/pemub47
10-31-15 10Q/Pg13+19: During 6mos ended 10-31-15, we sold 4,812,238sh at mkt prices under MLV AUG2015 AMI for gross=$5,186,000 before deducting commiss/costs of $132,000. As of 10-31-15, gross proceeds of up to $24,814,000 remained available. Subsequent to 10-31-15, thru 12-10-15, we sold 1,939,413sh for gross=$2,261,000. As of 12-10-15, $22,553,000 remained.
On 8-7-15, we entered into an “Equity Dist. Agreement” with Noble Life Science Partners, pursuant to which we may sell shares for gross proceeds of up to $20,000,000 (commission=2.5% of gross). As of 10-31-15, we had not sold any shares… Subsequent to 10-31-15 & thru 12-10-15, we sold 1,925,844 shs. at mkt prices for gross=$2,371,000. As of 12-10-15, gross of up to $17,629,000 remained available.
On 10-30-15, we entered into a Common Stock Pur. Agreement with EASTERN CAPITAL Ltd: sold 18,518,518shs @1.08/sh for gross=$20,000,000 before deducting issuance costs of $1,000.
10Q: http://tinyurl.com/zdbo9rv [10-30-15: Kenneth Dart (Eastern Capital) acquires 13.1% stake (30,106,945sh.) in PPHM http://tinyurl.com/24qctos ]
1-31-16 10Q/Pg13: During 9mos ended 1-31-16, we sold 6,751,651sh at mkt prices under MLV AUG2015 AMI for gross=$7,447,000 before commiss/costs =$190,000. As of 1-31-16, gross of $22,553,000 remained available. Subsequent to 10-31-15 thru 12-10-15, we sold 1,939,413sh for gross=$2,261,000. As of 12-10-15, $22,553,000 remained.
NOBLE Eq-Dist-AMI: during 9mos. ended 1-31-16, we sold 4,455,278shs. for gross of $5,228,000, commissions=$131,000. As of 1-31-16, $14,772,000 remained… http://tinyurl.com/hdgto9y
4-30-16 10K pg.F24+25: NOBLE Eq-Dist-AMI - FY’16 sales: 8,472,288sh. For gross=$6,969,000. As of 4-30-16, gross remaining=$13,031,000. Pg.F35/SUBSEQUENT EVENTS: NOBLE/EQ 5/1/16-7/14/16, sold 2,649,318sh. for gross=$1,232,000, a/o 7-14-16, $11,799,000 remain available. MLV AUG2015 AMI: 5/1/16-7/14/16, sold 1,876,918sh. for gross=$937,000, a/o 7-14-16, $21,616,000 remain available. 10K: http://tinyurl.com/zgognwz
7-31-16 10Q p.12: NOBLE Eq-Dist-AMI: 5/1/16-7/31/16, sold 2,649,318sh. for gross=$1,233,000, a/o 7-31-16, $ 11,798,000 remain available. MLV AUG2015 AMI: 5/1/16-7/31/16, sold 1,876,918sh. for gross=$937,000, a/o 7-31-16, $21,616,000 remain available. Pg16/SUBSEQUENT: PREFERRED/SeriesE: 8/1/16-9/8/16, we sold 68,910sh. for gross=$1,601,000; a/o 9-8-16, $9,134,000 remained available. 10Q: http://tinyurl.com/jmy77g3
10-31-16 10Q p.13: MLV AUG2015 AMI $30mm max, 2.5% commiss): 6mos ended 10-31-16, sold 8,309,357sh. for gross=$3,450,000. Pg17/SUBSEQUENT: 11/1/16 - 12-12-16, sold 3,788,346sh. for gross=$1,174,000. A/o 12-12-16, $17,929,000 remain available. NOBLE AUG2015 Eq-Dist-AMI($20mm max, 2.5% commiss): 6mos ended 10-31-16, sold 5,637,404sh. for gross=$2,516,000. Pg17/SUBSEQUENT: 11/1/16 - 12-12-16, sold 1,587,909sh. for gross=$496,000. A/o 12-12-16, $10,019,000 remain available.
1-31-17 10Q p12: MLV AUG2015 AMI $30mm max, 2.5% commiss): 9mos ended 1-31-17, sold 23,167,349 for gross=$8,028,000. At 1-31-17, $14,525,000 remain avail. Pg17/SUBSEQUENT: 2/1/17-3/13/17, sold 15,308,300 for gross=$7,335,000. A/o 12-12-16, $7,190,000 remain available.
NOBLE AUG2015 Eq-Dist-AMI($20mm max, 2.5% commiss): 9mos ended 1-31-17, sold 10,082,597 for gross=$3,916,000. At 3-13-17, $9,115,000 remain avail. Pg17/SUBSEQUENT: 2/1/17-3/13/17, sold 11,273,296 for gross=$6,006,000. A/o 3-13-17, $3,109,000 remain available.
= = = = = = = = = = =PREFERRED STOCK:
...2-5-14: PPHM Announces Public Offering of 10.5% Series E Convertible Preferred Stock http://tinyurl.com/lkxsna6
...2-11-14: PPHM Raises net $16.2mm selling 700k Preferred Shares with 10.5% div. at $25/sh, convertible to common at $3/sh http://tinyurl.com/jwmsnsk (8-K)
...6/14/14-7/14/13: PPHM Raises net $9.5mm selling 400k Preferred Shares with 10.5% div. at $25/sh, convertible to common at $3/sh http://tinyurl.com/mhva3k3 (4-30-14 10-K pg. F-34; $20mm gross remaining)
PREFERRED SHARES:
4-30-15 10K/p.F26: On 6-13-14, we entered into an At Market Issuance Sales Agreement with MLV, pursuant to which we may issue & sell shares of our Series E Preferred Stock through MLV, as agent, for gross proceeds of up to $30,000,000, in registered transactions from our Jan2014 Shelf. During FY’2015, we sold 799,764 shares of our Series E Preferred Stock at mkt prices for gross $19,205,000 before deducting commissions/costs of $1,002,000. As of 4-30-15, gross proceeds of up to $10,795,000 remained available under the Series E AMI Agreement.
NOTE: One of the holders of Preferred is KENNETH DART (EASTERN CAPITAL), who in a 2-13-15 SG14G ( http://tinyurl.com/k4nsfuu ) reported their 240,000sh. Preferred holdings as 2,000,000 common shares (SHARED VOTING POWER: 9,921,760,% OF CLASS REPRESENTED: 5.4%).
“which has a liquidation preference of $25.00/sh. and a conversion price of $3.00/sh.” 2,000,000 / 240,000 = 8.333
10Q: http://tinyurl.com/j2u2bjk
**7-31-16 10Q(iss. 9-8-16): 8/1/16-9/8/16, we sold 68,910sh. for gross=$1,601,000; a/o 9-8-16, $9,134,000 remained available.
4OUR, Customer A (56%/Q3) isn’t Halozyme…
Period Halozyme Cust-A Other-Custs
FYE 4-30-14 91% 1% 8%
FYE 4-30-15 79% 12% 9%
FYE 4-30-16 69% 26% 5%
Q/E 7-31-16 65% 29% 6%
Q/E 10-31-16 77% 10% 13%
Q/E 1-31-17 29% 56% 15%
Avid Revs FY17(fye 4-30-17) Guidance $60-65mm. I went back 4 prior years – they’re not in the habit of not beating the upper-ends of March Guidances. With Revs for 1st 3qtrs = (5.6 + 23.4 + 10.7) = $39.7mm, if they follow suit, Q4 Revs will be at least (65mm – 39.7) = $25mm.
...How close would that get us to Cash-Flow positive for Q4, should it happen? OP. CASH BURN for Q3(1-31-17) was: $6,274,000.
3-13-17/PR: “Avid Revenue Guidance Increased to $60-65mm for FY’17; Contracted B/L=$70mm”
ACTUAL FY17= $??.?mm (reported ~7-13-17)
= = = = = = = =
3-9-16/CC/PL: “$35-40mm and today, we believe we can exceed this guidance and top $40mm in contract mfg. revenues for the full FY'16.”
ACTUAL FY16= $44.4mm (reported 7-14-16)
3-12-15/CC/PL: “raising our contract mfg. revenue guidance to $23-25mm for the full FY’15.”
ACTUAL FY15= $26.7mm (reported 7-14-15)
3-7-14/CC/PL: “maintaining our initial contract mfg. revenue guidance of $18-22mm for the entire FY'14, and we are on track to hit the higher end of that range.”
ACTUAL FY14= $22.3mm (reported 7-14-14)
3-12-13/CC/PL: “we’re raising revenue guidance from for the entire FY’13 to at least $20mm.”
ACTUAL FY14= $21.3mm (reported 7-11-13)
AVID REVS TABLE THRU 1-30-17 (FY17/Q3):
http://investorshub.advfn.com/boards/read_msg.aspx?message_id=129479667
Updated PPHM REVS-BY-QTR TABLE, now thru FY17'Q3(qe 1-31-17), per the 10-Q ( http://tinyurl.com/zlozrv4 ) issued 3-13-17.
• Total Revs since May’06: ($213.3mm/Avid + $24.1mm/Govt + $2.5mm/Lic.) = $239.9mm
• 3-13-17: FY'17 (May'16-Apr'17) Avid revs guidance $60-65mm (Committed B/L=$70mm).
• Deferred-Revs at 1-31-17 total $26.4mm, UP from $18.0mm at 10-31-16.
• Cust.Deposits at 1-31-17 total $26.2mm, DOWN from $26.9mm at 10-31-16.
• Inventories at 1-31-17 total $33.8mm, UP from $25.9mm at 10-31-16.
• Avid’s Gross-Profit over last 4 qtrs: $22.3mm on revs of $58.5mm (GP%=38%)
• Recall, Avid Rev$ from Gov’t DTRA Contract work (6/30/08 – 4/15/11, totaling $24.15mm), went into GOVT-REVS, not AVID-REVS, in the Financials.
Avid’s website: http://www.avidbio.com
AVID PROFITABILITY (GROSS*) BY QTR:
QTR Avid-Rev$ CostofMfg$ Gross-Profit$ GP%
FY13Q1 7-31-12 4,135,000 2,024,000 2,111,000 51%
FY13Q2 10-31-12 6,061,000 3,703,000 2,358,000 39%
FY13Q3 1-31-13 6,961,000 3,651,000 3,310,000 47%
FY13Q4 4-30-13 4,176,000 3,217,000 959,000 23%
FY14Q1 7-31-13 4,581,000 2,670,000 1,911,000 42%
FY14Q2 10-31-13 7,354,000 4,195,000 3,159,000 43%
FY14Q3 1-31-14 3,885,000 2,416,000 1,469,000 38%
FY14Q4 4-30-14 6,474,000 3,829,000 2,645,000 41%
FY15Q1 7-31-14 5,496,000 3,583,000 1,913,000 35%
FY15Q2 10-31-14 6,263,000 4,139,000 2,124,000 34%
FY15Q3 1-31-15 5,677,000 3,113,000 2,564,000 45%
FY15Q4 4-30-15 9,308,000 4,758,000 4,550,000 49%
FY16Q1 7-31-15 9,379,000 4,608,000 4,771,000 51%
FY16Q2 10-31-15 9,523,000 4,741,000 4,782,000 50%
FY16Q3 1-31-16 6,672,000 3,896,000 2,776,000 42%
FY16Q4 4-30-16 18,783,000 9,721,000 9,062,000 48%
FY17Q1 7-31-16 5,609,000 3,062,000 2,547,000 45%
FY17Q2 10-31-16 23,370,000 15,441,000 7,929,000 34%
FY17Q3 1-31-17 10,747,000 7,974,000 2,773,000 26%
FY13 TOTAL: 21,333,000 12,595,000 8,738,000 41%*
FY14 TOTAL: 22,294,000 13,110,000 9,184,000 41%*
FY15 TOTAL: 26,744,000 15,393,000 11,151,000 42%*
FY16 TOTAL: 44,357,000 22,966,000 21,391,000 48%*
*Avid Net-Profit (ie, incl. Selling, G&A) not split out from PPHM-Corp. in the financials.
.
PPHM REVENUES (in thousands) DEFERRED
-------REVENUES------- REVENUES INVEN-
Quarter Avid Govt Lic. TOTAL Avid Govt TORIES
FY15Q1 7-31-14 5496 0 0 5496 4670 0 5998
FY15Q2 10-31-14 6263 0 37 6300 3612 0 5379
FY15Q3 1-31-15 5677 0 0 5677 5752 0 6148
FY15Q4 4-30-15 9308 0 0 9308 6630 0 6148
FY16Q1 7-31-15 9379 0 292 9671 8291 0 10457
FY16Q2 10-31-15 9523 0 0 9523 9688 0 12554
FY16Q3 1-31-16 6672 0 37 6709 15418 0 15189
FY16Q4 4-30-16 18783 0 0 18783 15418 0 15189
FY17Q1 7-31-16 5609 0 0 5609 21531 0 25274
FY17Q2 10-31-16 23370 0 0 23370 21531 0 25274
FY17Q3 1-31-17 10747 0 0 10747 26367 0 33829
Totals: 213295 24149 2453 239897 <=since5/1/2006
.
TOTAL REV’s BY YEAR (Avid+Gov’t+Lic):
FY04 4-30-04 3,314 …Avid(CMO)= 3,039 (Avid-Revs don’t incl. Govt-SVCS)
FY05 4-30-05 4,959 …Avid(CMO)= 4,684
FY06 4-30-06 3,193 …Avid(CMO)= 3,005
FY07 4-30-07 3,708 …Avid(CMO)= 3,492
FY08 4-30-08 6,093 …Avid(CMO)= 5,897
FY09 4-30-09 18,151 …Avid(CMO)= 12,963
FY10 4-30-10 27,943 …Avid(CMO)= 13,204
FY11 4-30-11 13,492 …Avid(CMO)= 8,502
FY12 4-30-12 15,233 …Avid(CMO)= 14,783
FY13 4-30-13 21,683 …Avid(CMO)= 21,333
FY14 4-30-14 22,401 …Avid(CMO)= 22,294
FY15 4-30-15 26,781 …Avid(CMO)= 26,744
FY16 4-30-16 44,686 …Avid(CMO)= 44,357
...Total Gov’t Revs from 7-2008 inception thru FY11Q1(Apr’11): $24.15mm
.
PPHM’S QTLY. NET LOSS BY QTR:
FY15Q1 7-31-14 13,129,000
FY15Q2 10-31-14 12,100,000
FY15Q3 1-31-15 12,994,000
FY15Q4 4-30-15 12,135,000
FY16Q1 7-31-15 13,723,000
FY16Q2 10-31-15 13,198,000
FY16Q3 1-31-16 16,847,000
FY16Q4 4-30-16 11,884,000
FY17Q1 7-31-16 11,057,000
FY17Q2 10-31-16 4,056,000
FY17Q3 1-31-17 7,774,000
= = = = = = = =
OPER. CASH BURNS* BY QTR(FROM THE 10-Q/K’S):
FY15Q3 1-31-15 11,116,000 (Q1+Q2+Q3: 32,139,000 10Q pg.26)
FY15Q4 4-30-15 10,474,000 (FY’15: 42,613,000 10K pg.54)
FY16Q1 7-31-15 12,306,000 (from 10Q pg.25)
FY16Q2 10-31-15 11,701,000 (Q1+Q2: 24,007,000 10Q pg.26)
FY16Q3 1-31-16 15,086,000 (Q1+Q2+Q3: 39,093,000 10Q pg.27)
FY16Q4 4-30-16 10,112,000 (FY'16: 49,205,000 10K pg.39)
FY17Q1 7-31-16 9,607,000 (from 10Q pg.22)
FY17Q2 10-31-16 2,565,000 (Q1+Q2: 12,172,000 10Q pg.24)
FY17Q3 1-31-16 6,274,000 (Q1+Q2+Q3: 18,446,000 10Q pg.24)
FY’09 total Op-Burn: $14,715,000
FY’10 total Op-Burn: $11,908,000
FY’11 total Op-Burn: $29,431,000
FY’12 total Op-Burn: $38,407,000
FY’13 total Op-Burn: $23,554,000
FY’14 total Op-Burn: $28,165,000
FY’15 total Op-Burn: $42,613,000
FY’16 total Op-Burn: $49,205,000
Period Halozyme Cust-A Other-Custs
FYE 4-30-14 91% 1% 8%
FYE 4-30-15 79% 12% 9%
FYE 4-30-16 69% 26% 5%
Q/E 7-31-16 65% 29% 6%
Q/E 10-31-16 77% 10% 13%
Q/E 1-31-17 29% 56% 15%
Seems Peregrine is Jedd Wolchok’s thrust at AACR’17. I wonder if maybe this might be in the cards down the road for Peregrine?
https://globenewswire.com/news-release/2015/09/11/767726/10149045/en/BeiGene-Announces-the-Addition-of-Dr-Jedd-D-Wolchok-to-Scientific-Advisory-Board.html
Apr1-5: AACR 2017, WashDC (5 PPHM Abstracts - see http://tinyurl.com/zdsbds8 )
1. MSKCC/WolchokLab+PPHM: 4-2-17/1pm #574, “PSTargeting+RAD+AntiPD1 Promotes Anti-Tumor Activity, Melanoma” (same as SITC'16/11-14-16 http://tinyurl.com/js3fca4 )
2. MSKCC/WolchokLab+PPHM: 4-3-17/8am #1651, “PSTargeting+Adoptive TCell Transfer (ACT) Eliminates Adv. Tumors w/o Off-Target Toxicities, Melanoma” <=NEW(2nd) Joint MemSloan/PPHM study, see: http://tinyurl.com/h3ylrku
. . .3 4 5...
=================
Mem. Sloan’s DR. JEDD WOLCHOK is co-author of 9 AACR’17 abstracts. 2 of the 9 are w/PPHM re: PS-Targeting. With biotechs, he has one each with Genocea Biosciences(ex-vivo screening), Infinity Pharm(Ph1), Leap Ther.(Ph1), and two with BMS(P1+3). The 8th is MSKCC ONLY, and the 9th is jointly w/Cedars-Sinai/LA. http://www.abstractsonline.com/pp8/#!/4292 .
PEREGRINE (Joint Mem.Sloan Kettering Wolchok Lab & PPHM):
1. 4-2-17 #574 “Phosphatidylserine Targeting Antibody in Combination with Tumor Radiation & Immune Checkpoint Blockade Promotes Anti-Tumor Activity in Mouse B16 Melanoma” <=Same as SITC’16 11-14-16.
2. 4-3-17 #1651 “Targeting Phosphatidylserine in Combination With Adoptive T Cell Transfer Eliminates Advanced Tumors Without Off-Target Toxicities in a Melanoma Preclin. Model” <=NEW/2nd PPHM+MSK.
NON-PEREGRINE:
3. (MSK ONLY): 4-2-17 #874 “Lifting the iron curtain: Imaging cellular barriers to combination chelation-immune checkpoint therapy”
4. (MSK & Genocea Bio. http://www.genocea.com GNCA/$130mm MktCap) 4-2-17 #632 “Genome-scale neoantigen screening using ATLAS prioritizes candidate antigens for immunotherapy in a NSCLC patient”
5. (MSK & Cedars-Sinai/LA) 4-4-17 #4705 “CTLA4 blockade with HER2-directed therapy yields clinical benefit in women undergoing radiation therapy for HER2+ breast cancer brain metastases”
6. (MSK & Infinity Pharm.) 4-4-17 #CT089 “A Ph1, first-in-human study of IPI-549, a PI3K-y inhibitor, as monotherapy & in combo w/nivolumab in adv. solid tumors”
7. (MSK & Leap Ther.) 4-2-17 #CT018 “Intratumor & peripheral Treg modulation as a pharmacodynamic biomarker of the GITR agonist antibody TRX-518 in the 1st in-human trial”
8. (MSK & BMS) 4-3-17 #CT073 “(Ph1) Immunomodulatory effects of NIVO+IPI or NIVO/mono in adv. melanoma: CheckMate038”
9. (MSK & BMS) 4-3-17 #CT075 “OS results from a Ph3 of NIVO+IPI in treatment-naïve pts w/adv. Melanoma: CheckMate067”
JDM, Item5 seems to Summarize everything down to 24.3mm 9.4%. They do seem to try to make these 13D's complicated to figure out!
ITEM3 vs. ITEM5 ??
See ITEM5: http://ir.peregrineinc.com/secfiling.cfm?filingid=1104659-17-15858&CIK=704562
3-9-17/13D: Ronin(J.Stafford) adds 3,248,405; group now 24,308,415sh. 9.4%.
As of 3-9-17:
20,814,248 sh. Ronin Cap/John Stafford - 350 N. Orleans St. Chicago, IL
+ 3,494,166 SWIM Partners/Stephen White - 737 N Michigan Ave., Chicago IL
= 24,308,415sh. 9.4% stake (of 257mm O/S per 12-8-16 10Q)
3-9-17 13D: http://tinyurl.com/huundwu
= = = = = = = = = = = = =
3-1-17 13D: Filed under ONE CUSIP(713661304/Ronin): 21,060,009sh.(8.2% stake), but then shows as 2 “reporting persons” in the detail:
17,565,843sh. Ronin Cap/John Stafford - 350 N. Orleans St. Chicago, IL
+ 3,494,166 SWIM Partners/Stephen White - 737 N Michigan Ave., Chicago IL
= 21,060,009sh. 8.2% stake (of 257mm O/S per 12-8-16 10Q)
3-1-17 13D: http://tinyurl.com/jr42u23
------
The two of them are acquiring as a “Group”…
***Group: “The fundamental factor for determining whether an aggregation of persons constitutes a group is whether the persons are ‘combined in furtherance of a common objective.’ Such a ‘concerted action’ by the group’s members does not need to be formally memorialized in writing.” https://media2.mofo.com/documents/faqs-schedule-13d-g.pdf
“13D filings are reserved for people or companies who may be interested in agitating for some kind of a change at the company, whereas "passive investors" (13G) are just that – passive.” http://www.davemanuel.com/investor-dictionary/schedule-13g
PPHM’s Sunrise Biomarkers (#1/Oct16, #2/Dec16, #3/AACR17)
A 3rd Sunrise Biomarker (IFN-y) was revealed on 3-1-17 when the AACR’17 Abstracts were released. It will be presented on 4-3-17: #CT159/25 (Session: Phase II/III Clinical Trials in Progress). IMO(stress IMO), this 3rd Biomarker is the superior and go-forward one for Peregrine (ie, “associated with improved outcomes for future bavituximab-containing trials”), since the latest one released and the only one to be presented at AACR’17. Summary of the 3 known Ph3/Sunrise Biomarker Data Presentations:
#1 10-10-16/ESMO’16: “B2GPI Biomarker(30%pts) StatSig OS 7.7=>13.2mos.”
David R. Spigel: LEAD AUTHOR: CSO/Dir. Lung Cancer Pgm/Sarah Cannon Res.
David E. Gerber: SENIOR AUTHOR: UTSW/Dallas (Sunrise PI)
CO-AUTHORS: R.Natale/CEDARS-SINAI, R.Sanborn/PROVCC, PPHM’s N.Kallinteris, J.Lai, M.Tang, J.Shan, and 7 Intl. Sunrise PI’s: Ger/2, Ukraine, Greece, Spain, Korea, Hungry.
RESULTS:
~200 of 600 pts (~30%) tested positive for B2GPI(200-240). Those 200 received Stat.Sig. Improvement in O/S 7.7=>13.2mos; ie, lived +70% longer.
MORE DETAILS: http://tinyurl.com/hp73njt
#2 12-7-16/WCLC’16(IASLC): “Complement & IL-10 Pathways Id Pts Benefiting from Bavi+Doce”
PRESENTATION CANCELLED – IR said,”Data analysis not completed in time.”
David E. Gerber: LEAD AUTHOR: UTSW/Dallas (Sunrise PI)
Rachael Sanborn: SENIOR AUTHOR: Dir./Thoracic-Oncology, Providence CC/Portland
CO-AUTHORS: L.Horn/VANDY, G.Losonczy/BUDAPEST, R.Natale/CEDARS-SINAI, H.Roder, J.Roder/BIODESIX, PPHM’s N.Kallinteris, M.Tang, J.Shan.
RESULTS:
104 of 193 pts tested high for complement activation, and from that, a 2nd subgrp isolated that tested low IL-10: O/S 5.9=>12.5mos. Remaining 397pts will be presented at WCLC’16.
* ”The Complement System is an enzyme cascade that is a collection of blood & cell surface proteins to help the abilities of antibodies to clear pathogens from an organism.”
* ”IL-10 is an anti-inflammatory TH2 cytokine that has a critical role in limiting the immune response to pathogens to prevent host damage.”
MORE DETAILS: http://tinyurl.com/z8cq8vx
. . . .
12-12-16 CEO/S.King: “We are actively evaluating addl. potential biomarkers and we hope to identify a profile for patients who will receive therapeutic benefit from treatment with bavituximab.” VP/JOE SHAN: ”Numerous addl. biomarkers are currently being evaluated.” http://tinyurl.com/hhn4gga
#3 - REVEALED BY AACR’17 ABSTRACT REL. 3-1-17 – SUNRISE BIOMARKER #3:
4-3-17/1pm #CT159/25 (Session: Phase II/III Clinical Trials in Progress)
“IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” <=this abstract is embargoed by AACR’17.
Nikoletta Kallinteris (PPHM): LEAD AUTHOR: Peregrine
Rachael Sanborn: SENIOR AUTHOR: Dir./Thoracic-Oncology, Providence
CO-AUTHORS: L.Horn/VANDY, T.Guennel/PRECISION-FOR-MEDICINE, PPHM’s N.Kallinteris, M.Tang, S.Yin, J.Lai, J.Shan.
* “IFNy, or type II interferon gamma, is a cytokine that is critical for innate & adaptive immunity against viral, some bacterial & protozoal infections.”
MORE DETAILS: http://tinyurl.com/zdsbds8
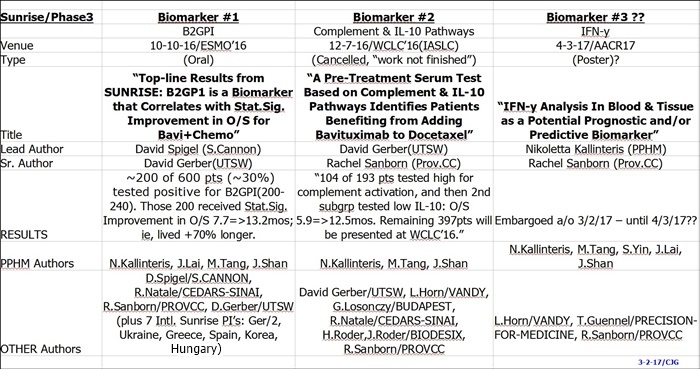
= = = = = = = =BIOMARKER #3 AND PPHM/NCCN JOHNS-HOPKINS TRIAL TIE-IN (IMO):
Dr. Ranee Mehra’s (Johns-Hopkins/SidneyKimmelCC) work with Biomarker IFN-y seems to dovetail into PPHM’s newly revealed Sunrise Biomarker #3 to be presented 4-3-17 at AACR’17: #CT159/25, “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” ( http://tinyurl.com/zaz525l ).
-------
1-6-17 Dr. Ranee Mehra (Johns-Hopkins/SidneyKimmelCC), P.I. for the upcoming NCCN Ph2 Bavi+Keytruda Head&Neck trial. Excerpts from her 1-6-17 talk at GBMC/Greater Balt. MC “H+N Grand Rounds”… I do believe she views this trial is an important part of Johns-Hopkins future anti-cancer direction. Also, look at her Slide #36: “Interferon-y Signature”. Is that an exact tie-in to the newly-revealed AACR’17(4-3-17) Sunrise Biomarker #3 Abstract, “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” (embargoed)? I still totally believe that PPHM has been working with the 3 NCCN Bavi Awardees (Moffitt, MassGEN, JohnsHopkins) to weave in the “chosen” Sunrise Biomarker that is associated with generating “improved outcomes for bavituximab-containing treatments” in future trials.
PDF Link(1-6-17): http://www.gbmc.org/workfiles/HeadNeck/Grand%20Rounds/IO_Therapy_SCCHN02017.pdf
-------
Note: DR. RANEE MEHRA was co-author of ASCO’16, “Biomarkers & Response to Pembro(Keytruda) in Recurrent/Metastatic Head & Neck Cancer” - Conclusion: “The IFN-y signature score was significantly associated with ORR, PFS, and OS (all, P< .001)… PD-L2 & IFN-y signature may be associated with clinical response to Pembro[Keytruda] and may offer addl. strategies to improve prediction of response.” http://meetinglibrary.asco.org/content/165708-176
PPHM’s NCCN#3: Ph2/Progressive Squamous Head+Neck (Bavi+Merck’s Keytruda), JOHNS-HOPKINS(Sidney Kimmel CC) - PI: Ranee Mehra, MD
”Phase II Study of Pembrolizumab[Keytruda] & Bavituximab for Progressive Recurrent/Metastatic Squamous Cell Carcinoma of the Head & Neck" http://tinyurl.com/gutgwb5
Ranee Mehra, MD: Dir., Head & Neck Oncology Therapeutics, Johns Hopkins Medicine https://www.linkedin.com/in/ranee-mehra-34a0467
RANEE MEHRA Disclosures(ASCO’16): GSK, Bayer, BMS, Genentech, Novartis, Mirati Ther.

NCCN Bavituximab Trials Announced 9-6-16 - To Begin "Early 2017" http://tinyurl.com/gutgwb5
...#1: Ph1/HepC-Related Hepatocellular(Liver) (Bavi+RAD+Sorafenib), MOFFITT CANCER CENTER - PI: Jessica Frakes, MD - https://clinicaltrials.gov/ct2/show/NCT02989870
...#2: P1-2/Newly Diag. Glioblastoma (Bavi+RAD+Merck’s Temodar), MASS-GEN. CANCER CENTER - PI: Elizabeth Gerstner, MD
...#3: Ph2/Progressive Squamous Head+Neck (Bavi+Merck’s Keytruda), JOHNS-HOPKINS(Sidney Kimmel CC) - PI: Ranee Mehra, MD
9-9-16/CC/JoeShan: “The 3rd award is for a Phase II study of pembrolizumab [Merck’s Keytruda, anti-PD-1] & bavituximab in Head & Neck Cancer. We are particularly excited about this project, as it will be the 1st clinical trial of bavituximab with a checkpoint inhibitor. In multiple previous preclin. studies, we have observed bavituximab's potential to work synergistically with PD1 inhibitors such as pembrolizumab (Merck’s Keytruda).” http://tinyurl.com/ktrfswj
- - - - - - - - - -
Steve King 9-9-16/CC: “Our collaboration with the NCCN has been an important part of our strategy for advancing the bavituximab clinical program in a cost effective way. We earlier provided NCCN with a $2mm grant to support bavituximab related clinical research with no further financial obligations, and these grant awards represent the outcome of a competitive selection process for the best proposals. These studies will evaluate novel bavituximab combinations in Glioblastoma, Head & Neck Cancer, and Hepatocellular Carcinoma, including an immunotherapy combination [Bavi + Merck’s Keytruda], which is a major focus for advancing the program.” http://tinyurl.com/ktrfswj
- - - - - - - - - -
Steve King 9-9-16/CC/Q&A: “I’m very excited about the combinations that were chosen because the Radiation combination is one that in preclinical studies, as was mentioned during the prepared remarks, has always shown a lot of promise. It’s great to be able to now see that put into a clinical setting in a couple of different clinical trials. And the I-O combinations, as Jeff mentioned during his prepared remarks, is a major focus of ours. So to see a Pembro [Merck’s Keytruda] combination picked as well, we are just really excited that these were the 3 winners out of the NCCN selection process.” http://tinyurl.com/ktrfswj
= = = = = = = = = = = = = =
Apr1-5: AACR 2017, WashDC http://tinyurl.com/zdsbds8 - SUMMARY of PPHM’s 5 AACR’17 ABSTRACTS: [See DETAILS below]
1. MSKCC+PPHM: 4-2-17/1pm #574, “PSTargeting+RAD+AntiPD1 Promotes Anti-Tumor Activity, Melanoma” (same as SITC'16/11-14-16 http://tinyurl.com/js3fca4 )
2. MSKCC+PPHM: 4-3-17/8am #1651, “PSTargeting+Adoptive TCell Transfer (ACT) Eliminates Adv. Tumors w/o Off-Target Toxicities, Melanoma” <=NEW(2nd) Joint MemSloan/PPHM study, see: http://tinyurl.com/h3ylrku
3. PPHM: 4-4-17/8am #3652, “PSTargeting+LAG3+AntiPD1 Significantly Enhances Anti-Tumor Activity, Triple- MBC”
4. IMMUNOVACCINE+PPHM: 4-4-17/8am #3657, ”PSTargeting Enhances Anti-Tumor Activity of a Tumor Vaccine(DepoVax), HPV-Induced Tumor” https://www.imvaccine.com
5. PPHM+VANDERBILT+PRECISIONMEDICINE+PROVIDENCECC: 4-3-17/1pm #CT159/25 (Session: Ph2/3 Clinical Trials in Progress), “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” (abstract embargoed, Sunrise Biomarker #3)
.
.
= = = = = = = = = =DETAILS ON SUNRISE BIOMARKERS #1(B2GPI) & #2(COMPLEMENT/IL-10):
#1 10-10-16/ESMO’16: “B2GPI Biomarker(30%pts) StatSig OS 7.7=>13.2mos.” http://tinyurl.com/hp73njt
10-10-16/PR:
“Peregrine Reports Top-Line and Initial Biomarker Data from Phase III SUNRISE Trial of Bavituximab in Oral Presentation at Eur. Society for Medical Oncology (ESMO) 2016 Congress”
-- Company Has Identified Beta-2 Glycoprotein-1 (B2GP1) as a Biomarker that Correlates with Statistically Significant Improvement in Overall Survival for Patients Receiving the Bavituximab Combination Compared to Chemotherapy Alone
-- Ongoing SUNRISE Trial Biomarker Analysis Expected to Identify Addl. Biomarkers Associated with Patients Benefiting from Bavituximab Treatment that Will Help Guide Program's Future Clinical Development. . .
** "With every clinical trial we conduct, we are constantly reminded of the difficulty involved in treating patients with NSCLC. This continues to prove to be a very challenging cancer to combat and the need for effective treatments remains high," David R. Spigel, MD, CSO and PgmDir. of Lung Cancer Res. at the Sarah Cannon Res. Inst. and one of the lead investigators in the SUNRISE trial. "The findings with regard to B2GP1 that have been collected as part of the ongoing SUNRISE trial data analysis are interesting and support further investigation."
** Peregrine intends to further evaluate the role of B2GP1 levels in response to bavituximab therapy in future clinical trials. The company has filed a new patent application directed to the use of this initial biomarker discovery. Addl. patient sample testing & analysis is ongoing and may result in other biomarkers of importance.
--------------
** Data presented at ESMO’16 demonstrated that patients with pre-treatment B2GP1 levels between 200 and 240 (representing approx. 30% of randomized patients) achieved a statistically significant, 5.5-mo. improvement (13.2 mos. vs. 7.7 mos.) in MOS as compared to patients in the ctl. group with the same range of B2GP1 levels [p = 0.049; HR=.67].
-------------
** "We would once again like to thank all of the patients, clinical investigators and scientists who participated in the SUNRISE trial and have made it possible for us to continue to collect and analyze a range of key data from the study. While we were disappointed with the trial being discontinued earlier in the year, we are excited by the fact that we are beginning to learn important information from the trial through the ongoing biomarker analysis program that will be critical in helping guide the future clinical development of bavituximab," said Joseph Shan, VP/Clin&Reg.Affairs at Peregrine. "It is encouraging that the initial biomarker analysis has identified an important biomarker early in the process and we are optimistic that additional biomarkers associated with improved outcomes for bavituximab-containing treatments will be identified as the analysis continues. We expect to be able to share the emerging data over the coming months at scientific & medical conferences as the more results become available.”
http://investorshub.advfn.com/boards/read_msg.aspx?message_id=125687447
= = = = = = = = = = = = = = = =
#2 12-7-16/WCLC’16(IASLC): “Complement & IL-10 Pathways Id Pts Benefitting from Bavi+Doce” <=CANCELLED/”Anal.Not.Done(IR)”
...Lead author (presenter) is UTSW’s Dr. David Gerber (previously presented Ph2/NSCLC data and Prelim. SUNRISE data at AACR’14). The Senior author is Dr. Rachel E. Sanborn, Co-Dir., Thoracic Oncology Pgm, Robert W. Franz Cancer Res. Center, Earle A. Chiles Res. Inst., Providence CC, Portland, OR. Interestingly, one co-author is Heinrich Roder, CTO of Biodesix, Boulder CO...
ABSTRACT CONCLUSION:
“...Proteomic & correlative approaches identified complement activation and low IL-10 levels as important pathways for predicting improved outcomes of patient treatment with Doce+Bavi, in line with preclinical work on Bavi’s MOA...” [Pts=193, within the 1st subgroup of N=104, a 2nd subgroup isolated: MOS 5.9mos => 12.5mos.]
Dec4-7 2016: “WCLC’16 - IASLC’s 17th World Conf. on Lung Cancer”, Vienna, Austria
http://wclc2016.iaslc.org Pgm: http://wclc2016.iaslc.org/wp-content/uploads/2016/10/WCLC-2016-Poster-Program.pdf
Poster Session with Presenters Present (ID 472) - Track: Advanced NSCLC
12/7/16 2:30-3:45pm David E. Gerber [UTSW], J. Roder, N.L. Kallinteris, L. Horn, G. Losonczy, R. Natale, M. Tang, Heinrich Roder [CTO, Biodesix http://www.biodesix.com/project/heinrichroder ], Joe S. Shan [VP/Clin+Reg], Rachel E. Sanborn [Providence Portland Medical Ctr]
”A Pre-Treatment Serum Test Based on Complement & IL-10 Pathways Identifies Patients Benefiting from the Addition of Bavituximab to Docetaxel”
ABSTRACT Book PDF: http://wclc2016.iaslc.org/wp-content/uploads/2016/12/WCLC2016-Abstract-Book_vF-WEB_revDec12.pdf
ABSTRACT: http://library.iaslc.org/virtual-library-search?product_id=6
BACKGROUND:
SUNRISE, a global, double-bind, Phase III trial of docetaxel (D) plus bavituximab (B) or D plus placebo (P) in previously treated non-squamous non-small cell lung cancer, demonstrated similar overall survival (OS) in both treatment arms. Mass spectrometry and correlative analysis were used to create a test able to identify a subgroup of patients benefitting from the addition of B to D.
METHODS:
Pre-treatment serum samples were available for 197 of the first 200 subjects enrolled in the trial. Mass spectra could be generated for 193 samples using the Deep MALDI method (Duncan et al, ASMS 2013), processed and features (peaks) identified. Mass spectral (MS) features associated with various biological functions were identified using a gene set enrichment analysis approach. Analysis of scores based on these MS feature, subsets indicated that in patients with High Complement Activation outcome depended on IL-10 activation in D+B but not in D+P. A test using the MS features associated with these functions was created to reliably identify a patient subgroup associated with clinical benefit using modern machine learning methods.
RESULTS:
Complement activation, as assessed by a classifier trained using related MS features, was a prognostic factor in both treatment arms, with high activation associated with poorer clinical outcome (OS HR = 0.54, log-rank p = 0.013 for D+B; OS HR = 0.60, log-rank p = 0.040 for D+P). Within the subgroup with high complement activation [N=50 (D+B); N=54 (D+P)], a second classifier using features related to IL-10 activation was able to isolate a subgroup of patients showing numerical benefit from the addition of B [Bavituximab] [median OS 5.9mos.(D+Placebo), 12.5mos.(D+Bavituximab)]. The remaining subgroup showed no benefit from addition of B [MOS 10.4mos.(D+P), 5.6mos.(D+B)]. Blinded validation of the test in the remainder 397 patients randomized in SUNRISE is will be presented.
CONCLUSION:
Proteomic and correlative approaches identified complement activation and low IL-10 levels as important pathways for predicting improved outcomes of patient treatment with D+B, in line with preclinical work on B’s mechanism of action. The test resulting from this work will undergo blinded indep. validation.
- - - - - - - - -
12-20-16/S.Diaz(per Cheynew post #282068): “There was no poster in Vienna. The team was working on a very tight timeframe and, despite their best efforts, couldn’t complete the data analysis in time. Given the crunch, we knew there was a possibility that we wouldn’t meet the timing, so we never issued a PR announcing that we would present. Hence no PR announcing that we did not present.” S.DIAZ/FOLLOWUP: ”Unfortunately, I don’t have a timeline for completion of the analysis or where/when it might be presented. We’ll certainly announce this as soon as we know for sure. Only Joe Shan attended the conference for Peregrine.”
= = = = = = = = = =NOTE:
Ann Oncol (11-8-16/suppl8): ESMO Symposium on Immuno-Oncology, Nov4-6 2016, Lausanne, Switzerland
#30P: “Proteomic Signature Analysis & Application in Clinical Development of the Novel Phosphatidylserine-Targeting Immunotherapy, Bavituximab”
http://annonc.oxfordjournals.org/content/27/suppl_8/mdw525.30
David E. Gerber [UTSW] 1, N.L. Kallinteris 2, L. Horn 3, G. Losonczy 4, R. Natale 5, Heinrich Roder 6 [CTO, Biodesix], M. Tang 7, J. Lai 2, J. Shan 8, Rachel E. Sanborn [9=Providence Portland Medical Ctr]
1 Oncology, UTSW-MC/Dallas
2 Clinical, Peregrine Pharmaceuticals Inc.
3 Oncology, Vanderbilt Ingram CC, Nashville, TN
4 Oncology, Semmelweis Univ., Budapest, Hungary
5 Oncology, Cedars-Sinai M/C, Los Angeles
6 Biodesix, Boulder, CO [CTO, Dr. Heinrich Roder: http://www.biodesix.com/project/heinrichroder ] “Founded in 2005, Biodesix discovers & commercializes cancer tests (diagnostics) that help patients & their doctors make more informed decisions about treatment based on a patient’s unique molecular profile.”
7 Biostatistics, Peregrine Pharmaceuticals Inc.
8 Clinical & Regulatory Affairs, Peregrine Pharmaceuticals, Inc.
9 Thoracic Oncology, Providence Cancer Care, Providence, OR
Aim/Background:
Understanding the multi-dimensional characteristics of cancer is essential to patient selection and treatment planning. Topline results from SUNRISE, a global double-blind Phase III trial of docetaxel + bavituximab (D+B) vs. docetaxel + placebo (D) in previously treated non-squamous NSCLC demonstrated mOS of 10.7mos. in the D+B group and 10.8mos. for the D group, which was unexpectedly different from the assumed 9.1mos. for D+B vs. 7.0mos. used for study powering. VeriStrat, a….[must subscribe]
- - - - - - - - - -
5-31-14 ASCO’14: David Gerber/Joe Shan Poster on Ph3/SUNRISE Trial (#TPS8129) http://tinyurl.com/nv4jloo
STOXX, thx for finding that about a 13D/"GROUP"... I just wove that into my post. Very interesting!
***Group(13D): “The fundamental factor for determining whether an aggregation of persons constitutes a group is whether the persons are ‘combined in furtherance of a common objective.’ Such a ‘concerted action’ by the group’s members does not need to be formally memorialized in writing.” https://media2.mofo.com/documents/faqs-schedule-13d-g.pdf
3-1-17: Ronin Cap+SWIM Partners (John Stafford+Stephen White) acquire 8.2% stake (21,060,009sh.) in PPHM
http://tinyurl.com/jr42u23 (13D)
“13D filings are reserved for people or companies who may be interested in agitating for some kind of a change at the company, whereas "passive investors" (13G) are just that – passive.” http://www.davemanuel.com/investor-dictionary/schedule-13g
3-1-17 13D: Filed under ONE CUSIP(713661304/Ronin): 21,060,009sh.(8.2% stake), but then shows as 2 “reporting persons” in the detail:
17,565,843sh. Ronin Cap/John Stafford - 350 N. Orleans St. Chicago, IL
+ 3,494,166 SWIM Partners/Stephen White - 737 N Michigan Ave., Chicago IL
= 21,060,009sh.
The two of them are a Team/Group*** of some sort? Can’t figure this out. I don’t see any relationship by Googling. OK, thanks to Stoxx...
------
***Group (13D): “The fundamental factor for determining whether an aggregation of persons constitutes a group is whether the persons are ‘combined in furtherance of a common objective.’ Such a ‘concerted action’ by the group’s members does not need to be formally memorialized in writing.” https://media2.mofo.com/documents/faqs-schedule-13d-g.pdf
3-1-17: Ronin Cap+SWIM Partners (John Stafford+Stephen White) acquire 8.2% stake (21,060,009sh.) in PPHM http://tinyurl.com/jr42u23 (13D)
“13D filings are reserved for people or companies who may be interested in agitating for some kind of a change at the company, whereas "passive investors" (13G) are just that – passive.” http://www.davemanuel.com/investor-dictionary/schedule-13g
Thanks, JDM - most interesting 13D-v-13G...
Schedule 13D is considered the long-form beneficial ownership report. ACTIVE INVESTORS in a company and investors who own more than 20% of a company must file Form SC 13D with EDGAR.
Schedule 13G is a beneficial ownership disclosure statement intended for PASSIVE INVESTORS who own less than 20% of a public company’s outstanding shares. A passive investor does not intend to exert control over or seek any changes in the company.
https://www.novaworkssoftware.com/blog/archives/38-Quick-Guide-Schedule-13D-vs.-Schedule-13G.html
-----------
3-1-17: Ronin Cap+SWIM Partners (John Stafford+Stephen White) acquire 8.2% stake (21,060,009sh.) in PPHM http://tinyurl.com/jr42u23 (13D)
-----------
“13D filings are reserved for people or companies who may be interested in agitating for some kind of a change at the company, whereas "passive investors" (13G) are just that – passive.”
http://www.davemanuel.com/investor-dictionary/schedule-13g
Sounds great, N40K – await your AACR attendee report! I wish and the missus could go early on April 3rd and catch the Wolchok Lab people presenting the new PPHM+MSKCC study, “PSTargeting+Adoptive TCell Transfer (ACT) Eliminates Adv. Tumors w/o Off-Target Toxicities, Melanoma” - that one has really got me excited.
Apr1-5: AACR 2017, WashDC http://tinyurl.com/zdsbds8 - SUMMARY of PPHM’s 5 AACR’17 ABSTRACTS: [See DETAILS below]
1. MSKCC+PPHM: 4-2-17/1pm #574, “PSTargeting+RAD+AntiPD1 Promotes Anti-Tumor Activity, Melanoma” (same as SITC'16/11-14-16 http://tinyurl.com/js3fca4 )
2. MSKCC+PPHM: 4-3-17/8am #1651, “PSTargeting+Adoptive TCell Transfer (ACT) Eliminates Adv. Tumors w/o Off-Target Toxicities, Melanoma” <=NEW(2nd) Joint MemSloan/PPHM study, see: http://tinyurl.com/h3ylrku
3. PPHM: 4-4-17/8am #3652, “PSTargeting+LAG3+AntiPD1 Significantly Enhances Anti-Tumor Activity, Triple- MBC”
4. IMMUNOVACCINE+PPHM: 4-4-17/8am #3657, ”PSTargeting Enhances Anti-Tumor Activity of a Tumor Vaccine(DepoVax), HPV-Induced Tumor” https://www.imvaccine.com
5. PPHM+VANDERBILT+PRECISIONMEDICINE+PROVIDENCECC: 4-3-17/1pm #CT159/25 (Session: Ph2/3 Clinical Trials in Progress), “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” (abstract embargoed, Sunrise Biomarker #3)
***Maybe Dr. Ranee Mehra (Johns Hopkins, PPHM’s NCCN Bavi+Keytruda Head&Neck Ph2 P.I.) will stop by!
...Dr. Mehra’s work with Biomarker IFN-y seems to dovetail into PPHM’s newly revealed Sunrise Biomarker #3 to be presented 4-3-17 at AACR’17: #CT159/25, “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” ( http://tinyurl.com/zaz525l ).
Note: DR. RANEE MEHRA was co-author of ASCO’16, “Biomarkers & Response to Pembro(Keytruda) in Recurrent/Metastatic Head & Neck Cancer” - Conclusion: “The IFN-y signature score was significantly associated with ORR, PFS, and OS (all, P< .001)… PD-L2 & IFN-y signature may be associated with clinical response to Pembro[Keytruda] and may offer addl. strategies to improve prediction of response.” http://meetinglibrary.asco.org/content/165708-176
MORE: http://tinyurl.com/h8gzkww
1-6-17 Dr.Ranee Mehra(Johns-Hopkins/SidneyKimmelCC), P.I. for the upcoming NCCN Ph2 Bavi+Keytruda Head&Neck trial. Excerpts from her 1-6-17 talk at GBMC/Greater Balt. MC “H+N Grand Rounds”… I do believe she views this trial is an important part of Johns-Hopkins future anti-cancer direction. Also, look at her Slide #36: “Interferon-y Signature”. Is that an exact tie-in to the newly-revealed AACR’17(4-3-17) Sunrise Biomarker #3 Abstract, “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” (embargoed)? I still totally believe that PPHM has been working with the 3 NCCN Bavi Awardees (Moffitt, MassGEN, JohnsHopkins) to weave in the “chosen” Sunrise Biomarker that is associated with generating “improved outcomes for bavituximab-containing treatments” in future trials.
PDF Link(1-6-17): http://www.gbmc.org/workfiles/HeadNeck/Grand%20Rounds/IO_Therapy_SCCHN02017.pdf
PPHM's NCCN#3: Ph2/Progressive Squamous Head+Neck (Bavi+Merck’s Keytruda), JOHNS-HOPKINS(Sidney Kimmel CC) - PI: Ranee Mehra, MD
”Phase II Study of Pembrolizumab & Bavituximab for Progressive Recurrent/Metastatic Squamous Cell Carcinoma of the Head & Neck" http://tinyurl.com/gutgwb5
Ranee Mehra, MD: Dir., Head & Neck Oncology Therapeutics, Johns Hopkins Medicine https://www.linkedin.com/in/ranee-mehra-34a0467
RANEE MEHRA Disclosures(ASCO’16): GSK, Bayer, BMS, Genentech, Novartis, Mirati Ther.
Note: DR. RANEE MEHRA was co-author of ASCO’16, “Biomarkers & Response to Pembro(Keytruda) in Recurrent/Metastatic Head & Neck Cancer” - Conclusion: “The IFN-y signature score was significantly associated with ORR, PFS, and OS (all, P< .001)… PD-L2 & IFN-y signature may be associated with clinical response to Pembro[Keytruda] and may offer addl. strategies to improve prediction of response.” http://meetinglibrary.asco.org/content/165708-176
...Dr. Mehra’s work with Biomarker IFN-y seems to dovetail into PPHM’s newly revealed Sunrise Biomarker #3 to be presented 4-3-17 at AACR’17: #CT159/25, “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” ( http://tinyurl.com/zaz525l ).
NCCN Bavituximab Trials Announced 9-6-16 - To Begin "Early 2017" http://tinyurl.com/gutgwb5
...#1: Ph1/HepC-Related Hepatocellular(Liver) (Bavi+RAD+Sorafenib), MOFFITT CANCER CENTER - PI: Jessica Frakes, MD - https://clinicaltrials.gov/ct2/show/NCT02989870
...#2: P1-2/Newly Diag. Glioblastoma (Bavi+RAD+Merck’s Temodar), MASS-GEN. CANCER CENTER - PI: Elizabeth Gerstner, MD
...#3: Ph2/Progressive Squamous Head+Neck (Bavi+Merck’s Keytruda), JOHNS-HOPKINS(Sidney Kimmel CC) - PI: Ranee Mehra, MD
9-9-16/CC/JoeShan: “The 3rd award is for a Phase II study of pembrolizumab [Merck’s Keytruda, anti-PD-1] & bavituximab in Head & Neck Cancer. We are particularly excited about this project, as it will be the 1st clinical trial of bavituximab with a checkpoint inhibitor. In multiple previous preclin. studies, we have observed bavituximab's potential to work synergistically with PD1 inhibitors such as pembrolizumab (Merck’s Keytruda).” http://tinyurl.com/ktrfswj
- - - - - - - - - -
Steve King 9-9-16/CC: “Our collaboration with the NCCN has been an important part of our strategy for advancing the bavituximab clinical program in a cost effective way. We earlier provided NCCN with a $2mm grant to support bavituximab related clinical research with no further financial obligations, and these grant awards represent the outcome of a competitive selection process for the best proposals. These studies will evaluate novel bavituximab combinations in Glioblastoma, Head & Neck Cancer, and Hepatocellular Carcinoma, including an immunotherapy combination [Bavi + Merck’s Keytruda], which is a major focus for advancing the program.” http://tinyurl.com/ktrfswj
- - - - - - - - - -
Steve King 9-9-16/CC/Q&A: “I’m very excited about the combinations that were chosen because the Radiation combination is one that in preclinical studies, as was mentioned during the prepared remarks, has always shown a lot of promise. It’s great to be able to now see that put into a clinical setting in a couple of different clinical trials. And the I-O combinations, as Jeff mentioned during his prepared remarks, is a major focus of ours. So to see a Pembro [Merck’s Keytruda] combination picked as well, we are just really excited that these were the 3 winners out of the NCCN selection process.” http://tinyurl.com/ktrfswj
= = = = = = = = = = = = = =
Apr1-5: AACR 2017, WashDC http://tinyurl.com/zdsbds8 - SUMMARY of PPHM’s 5 AACR’17 ABSTRACTS: [See DETAILS below]
1. MSKCC+PPHM: 4-2-17/1pm #574, “PSTargeting+RAD+AntiPD1 Promotes Anti-Tumor Activity, Melanoma” (same as SITC'16/11-14-16 http://tinyurl.com/js3fca4 )
2. MSKCC+PPHM: 4-3-17/8am #1651, “PSTargeting+Adoptive TCell Transfer (ACT) Eliminates Adv. Tumors w/o Off-Target Toxicities, Melanoma” <=NEW(2nd) Joint MemSloan/PPHM study, see: http://tinyurl.com/h3ylrku
3. PPHM: 4-4-17/8am #3652, “PSTargeting+LAG3+AntiPD1 Significantly Enhances Anti-Tumor Activity, Triple- MBC”
4. IMMUNOVACCINE+PPHM: 4-4-17/8am #3657, ”PSTargeting Enhances Anti-Tumor Activity of a Tumor Vaccine(DepoVax), HPV-Induced Tumor” https://www.imvaccine.com
5. PPHM+VANDERBILT+PRECISIONMEDICINE+PROVIDENCECC: 4-3-17/1pm #CT159/25 (Session: Ph2/3 Clinical Trials in Progress), “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” (abstract embargoed, Sunrise Biomarker #3)
Awesome, BS12. No doubt in my mind that Johns Hopkins’ Dr. R.Mehra is working with PPHM/NCCN to tailor the upcoming Bavi+Keytruda Head&Neck Ph2 trial to the new “IFN-y” Sunrise Biomarker #3 that was revealed in the AACR’17 abstract titles. In my mind, anyway!!
DR. RANEE MEHRA (Dir., Head & Neck Oncology Therapeutics, Johns Hopkins Medicine) was co-author of ASCO’16, “Biomarkers & Response to Pembro(Keytruda) in Recurrent/Metastatic Head & Neck Cancer” - Conclusion: “The IFN-y signature score was significantly associated with ORR, PFS, and OS (all, P< 0.001)… PD-L2 & IFN-y signature may be associated with clinical response to Pembro[Keytruda] and may offer addl. strategies to improve prediction of response.” RANEE MEHRA Disclosures: GSK, Bayer, BMS, Genentech, Novartis, Mirati Ther. http://meetinglibrary.asco.org/content/165708-176
MORE: http://tinyurl.com/jsdczj2


Apr1-5: AACR 2017, WashDC http://tinyurl.com/zdsbds8
SUMMARY of PPHM’s 5 AACR’17 ABSTRACTS:
1. MSKCC+PPHM: 4-2-17/1pm #574, “PSTargeting+RAD+AntiPD1 Promotes Anti-Tumor Activity, Melanoma” (same as SITC'16/11-14-16 http://tinyurl.com/js3fca4 )
2. MSKCC+PPHM: 4-3-17/8am #1651, “PSTargeting+Adoptive TCell Transfer (ACT) Eliminates Adv. Tumors w/o Off-Target Toxicities, Melanoma” <=NEW(2nd) Joint MemSloan/PPHM study, see: http://tinyurl.com/h3ylrku
3. PPHM: 4-4-17/8am #3652, “PSTargeting+LAG3+AntiPD1 Significantly Enhances Anti-Tumor Activity, Triple- MBC”
4. IMMUNOVACCINE+PPHM: 4-4-17/8am #3657, ”PSTargeting Enhances Anti-Tumor Activity of a Tumor Vaccine(DepoVax), HPV-Induced Tumor” https://www.imvaccine.com
5. PPHM+VANDERBILT+PRECISIONMEDICINE+PROVIDENCECC: 4-3-17/1pm #CT159/25 (Session: Ph2/3 Clinical Trials in Progress), “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” (abstract embargoed, Sunrise Biomarker #3)
= = = = = = = = = = = = = =
NCCN Bavituximab Trials Announced 9-6-16 - To Begin "Early 2017" http://tinyurl.com/gutgwb5
...#1: Ph1/HepC-Related Hepatocellular(Liver) (Bavi+RAD+Sorafenib), MOFFITT CANCER CENTER - PI: Jessica Frakes, MD - https://clinicaltrials.gov/ct2/show/NCT02989870
...#2: P1-2/Newly Diag. Glioblastoma (Bavi+RAD+Merck’s Temodar), MASS-GEN. CANCER CENTER - PI: Elizabeth Gerstner, MD
...#3: Ph2/Progressive Squamous Head+Neck (Bavi+Merck’s Keytruda), JOHNS-HOPKINS(Sidney Kimmel CC) - PI: Ranee Mehra, MD
N40K, Sorafenib(Nexavar) is Bayer's. I actually think PPHM may be working with the NCCN centers to weave in the latest Sunrise Biomarker selection (AACR/4-3-17 “IFN-y Analysis In Blood & Tissue as a Potential Prognostic and/or Predictive Biomarker” http://tinyurl.com/jmjqzey ) into the selection criteria of the 3 planned NCCN trials. Maybe that's why the Start Date on the Bavi+RAD+Sorafenib trial (Moffitt) was chgd. a few weeks back from Feb. to 4-30-17. ???
NCCN Bavituximab Trials Announced 9-6-16 - To Begin "Early 2017" http://tinyurl.com/gutgwb5
...#1: Ph1/HepC-Related Hepatocellular (Bavi+RAD+Sorafenib), MOFFITT CANCER CENTER - PI: Jessica Frakes, MD - https://clinicaltrials.gov/ct2/show/NCT02989870
...#2: P1-2/Newly Diag. Glioblastoma (Bavi+RAD+Merck’s Temodar), MASS-GEN. CANCER CENTER - PI: Elizabeth Gerstner, MD
...#3: Ph2/Progressive Squamous Head+Neck (Bavi+Merck’s Keytruda), JOHN-HOPKINS(Sidney Kimmel CC) - PI: Ranee Mehra, MD
PS: Is this the Sorafenib article you were referring to?
3-3-17: "A phase II study found that a neoadjuvant regimen of sorafenib, gemcitabine, and cisplatin (SGC) was well tolerated, with promising activity in patients with muscle-invasive urothelial bladder cancer (MIUBC)."
http://www.cancernetwork.com/bladder-cancer/sorafenib-plus-chemotherapy-promising-muscle-invasive-bladder-cancer

Just cleaned them up a bit, added a few more background things on Dr. Wolchok and Drs Fleming & Lyerly. Touch up work really, to improve them for iBox linking.
The PPHM/MSKCC(Jedd Wolchok Lab) Collab: #1/Bavi+PD1+Rad, #2/Bavi+”ACT”
CHRONOLOGICAL HISTORY:
On 2-12-17, AACR’17 revealed a 2nd(new) joint PPHM+MemSloan poster (study) that the Wolchok Lab will present on 4-3-17: “Targeting Phosphatidylserine in Combination with Adoptive T Cell Transfer Eliminates Advanced Tumors without Off-Target Toxicities in a Melanoma Preclinical Model”. This has obviously be known for some time by Mem.Sloan & Peregrine – the deadline for “regular abstracts” was Nov. 17th, and for “late breakers” was Jan. 12th.
Apr1-5 2017: “AACR 2017”, WashDC http://www.aacr.org/Meetings/Pages/MeetingDetail.aspx?EventItemID=105
AACR’17 PPHM+MSKCC/J.Wolchok Lab #1: (same as presented 11-14-16 at SITC’16)
#1. 4-2-17/1pm #574 - Session: CHECKPOINTS 1
“Phosphatidylserine Targeting Antibody in Combination with Tumor Radiation & Immune Checkpoint Blockade Promotes Anti-Tumor Activity in Mouse B16 Melanoma”
=> Sadna Budhu 1, Olivier De Henau 1, Roberta Zappasodi 1, Rachel Giese 1, Luis F. Campesato 1, Christopher Barker 1, Bruce Freimark 2, Jeff Hutchins 2, Jedd D. Wolchok 1, Taha Merghoub [Memorial Sloan Kettering]
1=Memorial Sloan Kettering CC, NYC [ http://www.mskcc.org/research-areas/labs/jedd-wolchok ]
2=Peregrine Pharmaceuticals
NOTE: SAME TITLE AS WAS PRESENTED BY Mem.Sloan 11-14-16 SITC’16: see http://tinyurl.com/js3fca4
ABSTRACT:
Phosphatidylserine (PS) is a phospholipid that is exposed on surface of apoptotic cells, tumor cells and tumor endothelium. PS has been shown to promote immunosuppressive signals in the tumor microenvironment. Antibodies that target PS have been shown to reactivate anti-tumor immunity by polarizing tumor associated macrophages into a pro-inflammatory M1 phenotype, reducing the number of MDSCs in tumors and promoting the maturation of dendritic cells into functional APCs. In a mouse B16 melanoma model, targeting PS in combination with immune checkpoint blockade promoted greater anti-tumor activity than either agent alone. This combination was shown to enhance CD4+ and CD8+ T cell infiltration and activation in the tumors of treated animals. Radiation therapy (RT) is an effective focal treatment of primary solid tumors, but is less effective in treating metastatic solid tumors as a monotherapy. There is evidence that RT induces immunogenic tumor cell death and enhances tumor-specific T cell infiltration in treated tumors. The abscopal effect, a phenomenon in which tumor regression occurs outside the site of RT, has been observed in both preclinical and clinical trials when RT is combined with immunotherapy. In this study, we show that irradiation treatment of B16 melanoma causes an increase in PS expression on the surface of viable tumor and immune infiltrates. We subsequently examined the effects of combining RT with an antibody that targets PS (mch1N11) [“Mouse version of Bavituximab”] and immune checkpoint blockade (anti-PD-1) in B16 melanoma. We found that treatment with mch1N11 synergizes with RT to improve anti-tumor activity and overall survival in tumor bearing mice. In addition, the triple combination of mch1N11, RT and anti-PD-1 treatment displayed even greater anti-tumor and survival benefit. Analysis of local immune responses in the tumors of treated animals revealed an increase in tumor-associated macrophages with a shift towards a pro-inflammatory M1 phenotype after treatment with RT & mch1N11. In addition, analysis of the systemic immune responses in the spleen and tumor draining lymph nodes revealed an increase in CD8 T cell activation, effector cytokine production and differentiation into effector memory cells in the triple combination. This finding highlights the potential of combining these 3 agents to improve outcome in patients with advanced-stage melanoma and other cancers and may inform the design of clinical studies combining PS-targeting antibodies with RT and/or checkpoint blockade.
AACR’17 PPHM+MSKCC/J.Wolchok Lab #2: (NEW, 2nd MSKCC Study)
#2. 4-3-17/8am #1651 - Session: TUMOR MICROENVIRONMENT & CHECKPOINTS
“Targeting Phosphatidylserine in Combination with Adoptive T Cell Transfer Eliminates Advanced Tumors without Off-Target Toxicities in a Melanoma Preclinical Model” <=NEW(2nd) MSK STUDY$$$
…...$$$See: More on the Significance of the New MSK/Wolchok+PPHM “ACT” study: http://tinyurl.com/h3ylrku
=> Daniel Hirschhorn-Cymerman 1, Sara Sara Schad 1, Sadna Budhu 1, Zhong Hong 1, Xia Yang 1, Hutchins T. Jeff 2, Bruce D. Freimark 2, Michael J. Gray 2, Jedd Wolchok 1, Taha Merghoub [Memorial Sloan Kettering]
1=Memorial Sloan Kettering CC, NYC [ http://www.mskcc.org/research-areas/labs/jedd-wolchok ]
2=Peregrine Pharmaceuticals
ABSTRACT:
A viable strategy to treat advanced cancers includes transferring of tumor-specific T cells. T cells that recognize tumor antigens can be expanded and reinvigorated ex-vivo. Furthermore, autologous T cells can be genetically modified to express anti-tumor T cell receptors or chimeric antigen receptors. Although the potency and specificity of tumor-specific T cells can be manipulated ex-vivo, once re-infused into patients, the T cells are subjected to immunosuppressive mechanisms established by the tumor. An important immune checkpoint regulator within tumors is phosphatidylserine (PS). Innate immune cells exposed to PS secrete suppressive cytokines and chemokines that can significantly impair the function and activation of anti-tumor T cells. Therefore, monoclonal antibodies that block PS activity can increase the anti-tumor potency of transferred T cells to treat aggressive cancers. Here we show that a PS targeting monoclonal antibody in combination with CD4+ T cells that recognize the melanoma antigen Trp1 can regress very advanced melanomas in all treated mice. Combination of anti-Trp1 CD4+ T cells with other immunomodulatory modalities such as anti-OX40 antibodies, can achieve equivalent treatment rates but these are typically accompanied by severe immune related adverse events. In contrast, in this setting, PS blockade did not show any off-target toxicities. Flow cytometry analysis revealed lower levels of CD206 expression concomitant with higher activation markers in macrophages and neutrophils in tumors from anti-PS treated mice. These results suggest that diminishing suppressive mechanisms locally in adoptive transfer protocols is a highly desirable strategy that can eliminate tumors while minimizing related adverse events.
----------
NOTE1:
From 3-2014 Immunotherapy article: “Cancer immunotherapy, particularly adoptive cell transfer (ACT), has shown great promise in the treatment of patients with late-stage disease, including those who are refractory to std. Therapies” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4372895
NOTE2:
Through the support from SEAN PARKER, Stand Up To Cancer (SU2C) and the Cancer Research Institute (CRI) formed an Immunology Research Dream Team dedicated to cancer immunology: “Immunologic Checkpoint Blockade & Adoptive Cell Transfer in Cancer Therapy.” The Immunotherapy Dream Team is focused on 2 approaches for this translational cancer research project, which will unite laboratory & clinical efforts towards the immunological treatment, control, and prevention of cancer.
The 1st is investigating blockades (by inhibitory molecules called “checkpoints”) of T lymphocytes’ inhibitory receptors, which block immune responses; and the use of antibodies to remove the checkpoints, once again allowing white blood cells called T lymphocytes to kill the cancer cells.
Second, the Immunotherapy Dream Team is pursuing multiple Adoptive Cell Transfer (ACT) approaches, which increase immunity.”
DREAM TEAM LEADERSHIP: 10 scientists, incl. MSKCC’s Jedd D. Wolchok & Michel Sadelain.
http://parker.org/initiatives/immunotherapy
-------
INTERESTING: Mem. Sloan’s Dr. Jedd. Wolchok is co-author of 9 AACR’17 abstracts. 2 of the 9 are w/PPHM re: PS-Targeting. With biotechs, he has one each with Genocea Biosciences(ex-vivo screening), Infinity Pharm(Ph1), Leap Ther.(Ph1), and two with BMS(P1+3). The 8th is MSKCC ONLY, and the 9th is jointly w/Cedars-Sinai/LA. http://www.abstractsonline.com/pp8/#!/4292 .
PEREGRINE (Joint Mem.Sloan Kettering Wolchok Lab & PPHM):
1. 4-2-17 #574 “Phosphatidylserine Targeting Antibody in Combination with Tumor Radiation & Immune Checkpoint Blockade Promotes Anti-Tumor Activity in Mouse B16 Melanoma” <=Same as SITC’16 11-14-16.
2. 4-3-17 #1651 “Targeting Phosphatidylserine in Combination With Adoptive T Cell Transfer Eliminates Advanced Tumors Without Off-Target Toxicities in a Melanoma Preclin. Model” <=NEW/2nd PPHM+MSK.
NON-PEREGRINE:
3. (MSK ONLY): 4-2-17 #874 “Lifting the iron curtain: Imaging cellular barriers to combination chelation-immune checkpoint therapy”
4. (MSK & Genocea Bio. http://www.genocea.com GNCA/$130mm MktCap) 4-2-17 #632 “Genome-scale neoantigen screening using ATLAS prioritizes candidate antigens for immunotherapy in a NSCLC patient”
5. (MSK & Cedars-Sinai/LA) 4-4-17 #4705 “CTLA4 blockade with HER2-directed therapy yields clinical benefit in women undergoing radiation therapy for HER2+ breast cancer brain metastases”
6. (MSK & Infinity Pharm.) 4-4-17 #CT089 “A Ph1, first-in-human study of IPI-549, a PI3K-y inhibitor, as monotherapy & in combo w/nivolumab in adv. solid tumors”
7. (MSK & Leap Ther.) 4-2-17 #CT018 “Intratumor & peripheral Treg modulation as a pharmacodynamic biomarker of the GITR agonist antibody TRX-518 in the 1st in-human trial”
8. (MSK & BMS) 4-3-17 #CT073 “(Ph1) Immunomodulatory effects of NIVO+IPI or NIVO/mono in adv. melanoma: CheckMate038”
9. (MSK & BMS) 4-3-17 #CT075 “OS results from a Ph3 of NIVO+IPI in treatment-naïve pts w/adv. Melanoma: CheckMate067”
FYI: JULY 2014: Mem. Sloan’s Jedd Wolchok Video: “Immunotherapy for Metastatic Melanoma - PD-1 Clinical Trials”… Dr. Wolchok (1:42), “We will not rest until every patient can have a durable response.” http://cyberspaceandtime.com/kvWeW8Zt0sU.video (1:49)
= = = = = = = = = = = = = = = = = = = = = = = = = = = = = = =
Remember, Dr. Wolchok spoke about Bavi in the 11-14-16/PR (SITC’16, Joint MSKCC & PPHM Poster, “Phosphatidylserine Targeting Antibody in Combination with Checkpoint Blockade & Tumor Radiation Therapy Promotes Anti-Cancer Activity in Mouse Melanoma”)… See: http://tinyurl.com/js3fca4
11-14-16: "Based on these study results, we believe that the targeting of PS is having meaningful activity within the tumor microenvironment in the B16 melanoma model," stated Dr. Jedd Wolchok. "It appears that this activity creates a more immune active environment in which other treatments, including radiation, are able to have a greater anti-tumor impact."
11-14-16: "We have noted that the combination of PS-targeting treatment and radiation, as well as triple combination of PS-targeting treatment, radiation and anti-PD-1, resulted in clear advantages in anti-tumor activity in the mouse B16 melanoma model," said Dr. Taha Merghoub, PhD, co-director of the Ludwig Collaborative Laboratory at MSK. "We believe that these findings suggest the potential benefit of combining these agents to improve the outcomes of patients with cancer. With this in mind, we think this research may play an important role in designing future clinical trials of PS-targeting agents in melanoma and other cancers."
CONCLUSION SECTION FROM THE JOINT MSKCC/PPHM SITC’16 POSTER:


- - - - - - - - - - - - - -
11-14-16/PR: New Study Demonstrates Anti-Tumor Advantages for Combination Treatment Featuring Peregrine Pharmaceuticals' PS-Targeting Antibodies in a Preclinical Melanoma Model
* Promising Results of MSK Study Evaluating Combinations of PS-Targeting Treatment, Anti-PD-1 and Radiation in Mouse B16 Melanoma Model Presented at SITC 2016
* New Data from Second Study Conducted by Peregrine Shows Triple Combination of PS-Targeting Treatment, Anti-PD-1 and Anti-LAG3 Created Long-Term Immunity in Triple Negative Breast Cancer Model; Protected Animals when Re-Challenged with Breast Cancer Cells
http://ir.peregrineinc.com/releasedetail.cfm?ReleaseID=999202
TUSTIN, Nov. 14, 2016: Peregrine Pharmaceuticals, Inc. (NASDAQ:PPHM/PPHMP), a biopharmaceutical company committed to improving patient lives by manufacturing high quality products for biotechnology and pharmaceutical companies and advancing its proprietary R&D pipeline, today announced the presentation of positive data from multiple new preclinical studies of the company's phosphatidylserine (PS)-targeting antibodies. Study results highlight that PS-targeting antibodies similar to bavituximab synergize with checkpoint inhibitors and radiation to improve anti-tumor activity in various animal tumor models. Importantly, the improved anti-tumor activity seen in these studies was even greater when PS-targeting therapy was a part of triple combination treatment including anti-PD-1 and another therapy. Data were presented by Peregrine scientists, as well as researchers from Memorial Sloan Kettering Cancer Center (MSK), at the Society for Immunotherapy of Cancer (SITC) 2016 Annual Meeting, which was held November 9-13, 2016 in National Harbor, MD. [ http://www.sitcancer.org/2016 ]
Initial results from Peregrine's ongoing collaboration with MSK researchers were featured in a poster presented by Sadna Budhu, PhD, at SITC 2016. A team of MSK researchers led by cancer immunotherapy thought-leaders, Taha Merghoub, PhD and Jedd D. Wolchok, MD, PhD [ http://www.mskcc.org/research-areas/labs/jedd-wolchok ], evaluated the effects of combining PS-targeting, anti-PD-1 and radiation therapies in the mouse B16 melanoma model. Study data showed that PS-targeting antibodies synergize with both anti-PD-1 and radiation therapy to improve anti-cancer activity. PS-targeting treatment in combination with radiation, as well as triple combination of PS-targeting treatment, anti-PD-1 and radiation, led to a reduction in tumor burden. Median survival for the triple combination treatment still had not been reached at the end of the 80-day observation period with other arms in the study showing median survival that ranged from 24-70 days.
Researchers also evaluated the impact of the PS-targeting and radiation combination treatment on the level and type of immune activity. These results demonstrated that the combination led to a change in the tumor microenvironment, shifting it from immunosuppressive in which tumors are protected to immune active in which tumors are more susceptible to treatment. Analysis of local immune responses in the tumors of the treated animals showed that the combination treatment increased the number of tumor associated macrophages and shifted the macrophage polarization from the immunosuppressive M2 type to the immune active M1 type. When systemic immune responses were analyzed following triple combination of PS-targeting treatment, anti-PD-1 and radiation, researchers also saw evidence of increased immune activity. This was illustrated by key indicators of immune activity, including increases in CD8+ T-cell activation, effector cytokine production and differentiation into effector memory cells.
"Based on these study results, we believe that the targeting of PS is having meaningful activity within the tumor microenvironment in the B16 melanoma model," stated Dr. Jedd Wolchok. "It appears that this activity creates a more immune active environment in which other treatments, including radiation, are able to have a greater anti-tumor impact."
"We have noted that the combination of PS-targeting treatment and radiation, as well as triple combination of PS-targeting treatment, radiation and anti-PD-1, resulted in clear advantages in anti-tumor activity in the mouse B16 melanoma model," said Dr. Taha Merghoub, PhD, co-director of the Ludwig Collaborative Laboratory at MSK. "We believe that these findings suggest the potential benefit of combining these agents to improve the outcomes of patients with cancer. With this in mind, we think this research may play an important role in designing future clinical trials of PS-targeting agents in melanoma and other cancers."
[Note: FULL SITC’16 ABSTRACT #199: http://bit.ly/2dHTEVn
...Full Poster Image: http://peregrineinc.com/images/stories/pdfs/sitc_2016_budhu.pdf ]
A second study, conducted by Peregrine, evaluated the effects of combining PS-targeting, anti-PD-1 and anti-LAG3 therapies in the E0771 triple negative breast cancer (TNBC) model. Initial findings from this study were previously reported and demonstrated that eight of the ten (80%) animals receiving the PS-targeting, anti-PD-1 and anti-LAG3 treatment combination experienced complete tumor regressions, whereas there were no animals (0/10) in the anti-PD-1 and anti-LAG3 combination treatment arm that had a complete regression. New data presented for the first time at SITC demonstrated that the triple combination established a specific and prolonged anti-tumor immune response which protected those eight animals that achieved a complete tumor regression against a re-challenge with the same E0771 TNBC model tumor cells. This sustained anti-tumor response demonstrates the ability of the triple combination treatment to trigger immune system memory and support adaptive immune responses against reemerging disease in the E0771 TNBC model.
[Note: FULL SITC’16 ABSTRACT #213: http://bit.ly/2dpUy4C ]
...Full Poster Image: http://peregrineinc.com/images/stories/pdfs/sitc_2016_gray.pdf ]
Further highlighting the immune impact of the PS-targeting/anti-PD-1/anti-LAG3 treatment combination were initial results of a new analysis from this study using the nCounter ® PanCancer Immune Profiling Panel from NanoString Technologies ®. Data from the analysis demonstrated that the triple combination induced a greater shift in the tumor microenvironment from immunosuppressive to immune active as compared to all other treatment groups. This was evidenced by greater increases in the activity of several critical immune activating pathways, including presentation and processing of antigens and signaling and activation of T-cells, for the triple combination as compared to all other treatments.
"It is very encouraging to see the consistent increase in anti-tumor activity triggered by triple combination treatments that combine PS-targeting agents and anti-PD-1 with other cancer treatments. By demonstrating this activity across multiple studies in multiple tumor models, we are continuing to build scientific support for the therapeutic potential of adding PS-targeting therapies in combination with other cancer treatments, including checkpoint inhibitors such as anti-PD-1," said Jeff T. Hutchins, PhD, Peregrine's VP, Preclinical Research. "As cancer research continues to explore the potential of combination treatments that marry complementary mechanisms, we are pleased to see that our efforts continue to generate data supporting the role that PS-targeting agents such as bavituximab may play in this area."
Bavituximab is an investigational monoclonal antibody that targets PS. Signals from PS inhibit the ability of immune cells to recognize and fight tumors. Bavituximab is believed to override PS mediated immunosuppressive signaling by blocking the engagement of PS with its receptors as well as by sending an alternate immune activating signal. Previous studies demonstrated PS-targeting antibodies shift the functions of immune cells in tumors, resulting in multiple signs of immune activation and anti-tumor responses. Peregrine continues to support and guide clinical development through the evaluation of the preclinical equivalent of bavituximab, ch1N11, in animal model studies.
Peregrine's clinical development strategy for bavituximab currently focuses on small, early-stage, proof-of-concept trials evaluating the drug in combination with other cancer treatments. This approach includes the recently announced grants awarded by the National Comprehensive Cancer Network (NCCN) to support three different clinical trials of bavituximab treatment combinations [See: http://tinyurl.com/gutgwb5 ]. These trials will evaluate novel bavituximab combinations in glioblastoma, head and neck cancer, and hepatocellular carcinoma including an immunotherapy combination. Additionally, Peregrine continues to advance its pre-clinical collaboration with Memorial Sloan Kettering Cancer Center with the goal of evaluating combinations of bavituximab with other checkpoint inhibitors and immune stimulatory agents. The intent behind this strategy is to focus our research and development spending to further validate bavituximab's combination potential as we seek to advance the program though a pharmaceutical or biotechnology partner.
ABOUT PEREGRINE *SNIP*
= = = = = = = = = = = = = = = = = = = = = = = = = = =
MSKCC/Wolchok-Lab & PPHM, Nov11-12 2016, Natl-HarborMD. 3 PS-Targeting/I-O Abstracts – note that the 1st one (#199 Nov. 11, 2016) is the joint MSKCC/PPHM one; its Senior author is Dr. Taha Merghoub (Jedd Wolchok Lab, Memorial Sloan Kettering), who said this in the 5-29-15 PPHM/MSK Collab. Announcement PR (see below): "A key focus of the Wolchok Lab's research is studying novel immunotherapy combinations that work together to enable the immune system to recognize & destroy cancer. This collaboration will allow us to focus on the role & contribution of PS blockade therapy in determining which combination of the current and next generation of immune modulators is likely to increase the extent and amplitude of anti-tumor response. This important pre-clinical & translational work will potentially guide the design of the next generation of clinical studies with bavituximab."
Nov9-13 2016: “(SITC) Society for Immunotherapy of Cancer 31st Annual Meeting”, Natl-Harbor MD
”The premier destination for scientific exchange, education, and networking in the Cancer Immunotherapy Field”
SITC = The Society for Immunotherapy of Cancer http://www.sitcancer.org
SITC 2016 Meeting: http://www.sitcancer.org/2016
Abstracts: http://www.sitcancer.org/2016/abstracts
PEREGRINE/MSKCC ABSTRACTS:
I. 11-11-16 12:15-1:30pm #199: “Phosphatidylserine Targeting Antibody in Combination with Checkpoint Blockade & Tumor Radiation Therapy Promotes Anti-Cancer Activity in Mouse Melanoma” - Sadna Budhu, PhD - Ludwig Collaborative Lab, MSKCC (Memorial Sloan Kettering)
AUTHORS: Sadna Budhu(MSKCC PRESENTING AUTHOR) 1, Olivier De Henau 2, Roberta Zappasodi 1, Kyle Schlunegger 3, Bruce Freimark 4, Jeff Hutchins 5, Christopher A. Barker 6, Jedd D. Wolchok 7, Taha Merghoub(MSKCC SENIOR AUTHOR) 1 [<=See 5-29-15 PPHM/MSKCC PR below]
1/2 Ludwig Collaborative Lab, Memorial Sloan Kettering CC, NYC
6 Memorial Sloan Kettering CC, NYC
7 Dept of Medicine, Memorial Sloan Kettering CC, NYC
3/4/5 Peregrine Pharmaceuticals, Tustin, CA
ABSTRACT: http://bit.ly/2dHTEVn POSTER PDF: http://peregrineinc.com/images/stories/pdfs/sitc_2016_budhu.pdf
II. 11-12-16 11:45-1pm #210: “Antibody Targeting of Phosphatidylserine Enhances the Anti-Tumor Responses of Ibrutinib & anti-PD-1 Therapy in a Mouse Triple Negative Breast Tumor Model” - Jian Gong, PhD - Peregrine Pharmaceuticals
AUTHORS: Jian Gong, Michael Gray, Jeff Hutchins, Bruce Freimark - Peregrine Pharm. ABSTRACT: http://bit.ly/2dpUh1w POSTER PDF: http://peregrineinc.com/images/stories/pdfs/sitc_2016_gong.pdf
III. 11-11-16 12:15-1:30pm #213: ”Monoclonal Antibodies Targeting Phosphatidylserine Enhance Combinational Activity of the Immune Checkpoint Targeting Agents LAG3 & PD-1 in Murine Breast Tumors” - Michael Gray, PhD - Peregrine Pharmaceuticals
AUTHORS: Michael Gray, Jian Gong, Jeff Hutchins, Bruce Freimark - Peregrine Pharm. ABSTRACT: http://bit.ly/2dpUy4C POSTER PDF: http://peregrineinc.com/images/stories/pdfs/sitc_2016_gray.pdf
= = = = = = = = = = = =FULL ABSTRACT OF THE PPHM/MSKCC POSTER:
http://resource-cms.springer.com/springer-cms/rest/v1/content/11027680/data/v1/Volume+4+Supplement+1+PDF+pt+2
#199/SITC’16/11-11-16(MSK+PPHM): “Phosphatidylserine Targeting Antibody in Combination with Checkpoint Blockade & Tumor Radiation Therapy Promotes Anti-Cancer Activity in Mouse Melanoma”
AUTHORS:
Sadna Budhu(MSKCC PRESENTING AUTHOR) 1, Olivier De Henau 2, Roberta Zappasodi 1, Kyle Schlunegger 3, Bruce Freimark 4, Jeff Hutchins 5, Christopher A. Barker 6, Jedd D. Wolchok 7, Taha Merghoub(Memorial Sloan Kettering SENIOR AUTHOR)
BACKGROUND:
Phosphatidylserine (PS) is a phospholipid that is exposed on the surface of apoptotic cells, some tumor cells and tumor endothelium. PS has been shown to promote anti-inflammatory and immunosuppressive signals in the tumor microenvironment. Antibodies that target PS have been shown to reactivate anti-tumor immunity by repolarizing tumor associated macrophages to a M1-like phenotype, reducing the number of MDSCs in tumors and promote the maturation of dendritic cells into functional APCs. In a B16 melanoma model, targeting PS in combination with immune checkpoint blockade has been shown to have a significantly greater anti-cancer effect than either agent alone. This combination was shown to enhance CD4+ and CD8+ T cell infiltration and activation in the tumors of treated animals. Radiation therapy is an effective focal treatment of primary solid tumors, but is less effective in treating metastatic solid tumors as a monotherapy. There is evidence that radiation induces immunogenic tumor cell death and enhances tumor-specific T cell infiltration in irradiated tumors. In addition, the abscopal effect, a phenomenon in which tumor regression occurs outside the site of radiation therapy, has been observed in both preclinical and clinical trials with the combination of radiation therapy and immunotherapy.
METHODS:
We examined the effects of combining tumor radiation therapy with an antibody that targets PS (1 N11) [Note: PGN635 (B2GPI-dep.) is Fully-Human Bavituximab=1N11=AT004; Genentech studying 89Zr-PGN635 as a Tumor Imaging Agent, “indep. of cancer type”] and an immune checkpoint blockade (anti-PD-1) using the mouse B16 melanoma model. Tumor surface area and overall survival of mice were used to determine efficacy of the combinations.
RESULTS:
We examined the expression of PS on immune cells infiltrating B16 melanomas. CD11b + myeloid cells expressed the highest levels of PS on their surface whereas T cells and B16 tumor cells express little to no PS. These data suggest that targeting PS in B16 melanoma would induce a pro-inflammatory myeloid tumor microenvironment. We hypothesize that therapies that induce apoptotic cell death on tumor cells would enhance the activity of PS-targeting antibodies. We therefore examined the effects of combining a PS-targeting antibody with local tumor radiation. We found that the PS-targeting antibody synergizes with both anti-PD-1 and radiation therapy to improve anti-cancer activity and overall survival. In addition, the triple combination of the PS-targeting antibody, tumor radiation and anti-PD-1 treatment displayed even greater anti-cancer and survival benefit.
CONCLUSIONS:
This finding highlights the potential of combining these 3 agents to improve outcome in patients with advanced-stage melanoma and may inform the design of future clinical trials with PS targeting in melanoma and other cancers *end*
...FULL POSTER IMAGE: http://peregrineinc.com/images/stories/pdfs/sitc_2016_budhu.pdf ]
= = = = = = = = = = = =
9-8-16/CC - JEFF HUTCHINS (VP/PreClinical Res.) http://tinyurl.com/jmy77g3
“...I would now like to provide an update on Peregrine's preclinical I-O focused internal efforts and our collaboration with Memorial Sloan Kettering Cancer Center. The goal of this work is to evaluate combinations of PS targeting with other checkpoint inhibitors and immune stimulatory agents for the purpose of developing new and increasingly effective anticancer treatments. These programs are advancing well and to-date, we have seen impressive signs of activity with new combinations of PS targeting and other treatment modalities such as checkpoint blockers, T-cell agonists and radiation. These new combinations are improving overall survival accompanied with increases in cyto-reactive T cells into the tumor tissue. This exciting new internal work will be presented at the AACR/CRI Immunotherapy Meeting in New York later this month [Sept25-28] and at ESMO in early October [Oct7-11: http://tinyurl.com/jxdppyo ]. We expect the first results from our collaboration with MSK’s Jedd Wolchok Lab investigators [See MSK Collab: http://tinyurl.com/zkvebh6 ] to be presented at SITC in November [Nov9-13: http://www.sitcancer.org/2016 Natl.Harbor MD] and we will provide more detailed information as that presentation becomes available.”
= = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = =
5-29-15: Peregrine & Sloan Kettering Enter Collab. to “Investigate Novel PS-Targeting Immunotherapy Combos” http://tinyurl.com/o3k9ux8
...The studies at MSK will be performed under the direction of Taha Merghoub, PhD, [ http://www.mskcc.org/research-areas/labs/members/taha-merghoub-01 ] Associate Attending Biologist, Melanoma and Immunotherapeutics Service, Ludwig Collaborative and the Swim Across America Laboratory, a part of the laboratory of Jedd D. Wolchok, MD, PhD [ http://www.mskcc.org/research-areas/labs/jedd-wolchok ], a leader in the field of cancer immunotherapy. Dr. Wolchok serves as the Chief, Melanoma and Immunotherapeutics Service, Lloyd J. Old Chair for Clinical Investigation as well as an Associate Director of the Ludwig Center for Cancer Immunotherapy at MSK.
----
”The phosphatidylserine (PS) signaling pathway is a very interesting target for modulating the immune system's response to cancer. We look forward to exploring the potential of PS-targeting agents alone and with other immune modulators that may lead to novel advances in cancer therapy," said Dr. Jedd Wolchok.
–--
As part of the collaboration, researchers at MSK will conduct research to further explore the combination of PS-targeting agents, including bavituximab, that block a primary immunosuppressive pathway thereby allowing anti-tumor immune responses with other immuno-stimulatory agents that enhance immune responses. Specifically, MSK researchers will examine the combination of bavituximab alongside models of checkpoint blockade that are unresponsive to inhibition or co-stimulation given the ability of bavituximab to reprogram myeloid derived suppressor cells (MDSC) and increase tumoricidal T-cells in tumors, a mechanism of action that is complementary to checkpoint blockade and T-cell activation.
–--
"A key focus of the Wolchok Lab's research is studying novel immunotherapy combinations that work together to enable the immune system to recognize & destroy cancer. This collaboration will allow us to focus on the role & contribution of PS blockade therapy in determining which combination of the current & next gen. of immune modulators is likely to increase the extent & amplitude of anti-tumor response. This important pre-clinical and translational work will potentially guide the design of the next gen. of clinical studies with bavituximab," said Dr. Taha Merghoub.
–--
"We are delighted to be working with a world-renowned pioneer and leader in the immuno-oncology space, recognizing that there remains significant research in order for more cancer patients to realize the benefits of combination immune therapy," said Jeff T. Hutchins, PhD, VP of Preclinical Research at Peregrine. ”Our internal and collaborative research presented over the last year has established a robust foundation of PS-targeting activity on which to initiate this next chapter in PS research and development."
–--
"This collaboration is an important extension of our established research efforts to further explore and understand the potential of our PS-targeting platform including bavituximab our lead clinical candidate. This research will focus on better understanding how treatment with PS-targeting agents can assist other anti-tumor immunotherapies in order to work better," said Steven King, CEO of Peregrine. ”Our goal is to change the way cancer patients are treated by allowing their immune system to recognize and fight their disease. This collaboration will undoubtedly assist us in identifying potential new opportunities to better treat patients with cancer."
Eb0783, incredible post about the Buckeye Cruise for Cancer, The James Cancer Center, the NCCN, and your many interactions with those researchers. I'm still trying to absorb it all!
What a Major Contribution to this board!!!
PD, interesting re: DNAtrix. MDA's testing their drug+BAVI, but the 1-30-17 article only lists 10 MDA'ers and Dr. Brekken as authors, so I figured we can't jump to calling them a collab. Could lead eventually to something though. I still find it hard to believe OUR list of ACTIVE Bavi Collab Testers include (but not limited to!) the BIG 3 of the U.S. Cancer research world => MSKCC, DUKE, and MDA. Do they get any bigger than that?!!
2-28-17: Collabs with Mem.Sloan(Wolchok), Duke, MDA, Rutgers, ImmunoVaccine, UTSW... http://tinyurl.com/heg9t3v
PD, actually I posted it earlier, but I had to clean it up and add some more info about MDA's Dr. Jason B. Fleming, the senior author. He's an MDA heavyweight.
Add MD-Anderson to our collaborators list. This 1-30-17 article was authored by 10 MDA researchers (LEAD: Jason B. Fleming), joined by UTSW’s Rolf Brekken (PPHM SAB). It’s preclin. results of a study of DNAtrix’s DNX2401 + MouseBAVI in Pancreatic, whereby the abstract states that the combo “further enhanced anticancer activity, possibly through inducing synergistic anticancer immune responses.”...
1-30-17 Mol Cancer Therapy: “Preclinical Evaluation of Sequential Combination of Oncolytic Adenovirus Delta-24-RGD and Phosphatidylserine-Targeting Antibody [1N11=MouseBAVI] in Pancreatic Ductal Adenocarcinoma”
Rec/8-5-16, Rev/12-1-16, Acc/12-15-16, PUB/1-30-17
Dai B 1, Roife D 1, Kang Y 1, Gumin J 2, Rios Perez MV 1, Li X 1, Pratt M 1, Rolf Brekken [PPHM SAB] 3, Fueyo-Margareto J 4, Lang FF 2, Jason B Fleming [MDA]***
1 Dept of Surgical Oncology, Univ. of Texas MDA CC
2 Dept of Neurosurgery, Univ. of Texas MDA CC
3 Hamon Ctr for Therapeutic Oncology Res., Depts Surgery/Pharmacology, UTSW-MC
4 Dept of Neuro-Oncology, Univ. of Texas MDA CC
5 Dept of Surgical Oncology, Univ. of Texas MDA CC
***Lead author: JASON B. FLEMING, “Dir. of the Tissue Acquisition & Biorepository Core for the Pancreas Cancer Res. Pgm at MDA” http://faculty.mdanderson.org/Jason_Fleming/
http://mct.aacrjournals.org/content/early/2017/01/28/1535-7163.MCT-16-0526
ABSTRACT
Delta-24-RGD (DNX-2401) [DNXtrix Co.**] is a conditional replication-competent oncolytic virus engineered to preferentially replicate in and lyse tumor cells with abnormality of p16/RB/E2F pathway. In a phase 1 clinical trial, Delta-24-RGD has shown favorable safety profile and promising clinical efficacy in brain tumor, which prompted us to evaluate its anticancer activity in pancreatic ductal adenocarcinoma (PDAC), which also has high frequency of homozygous deletion and promoter methylation of CDKN2A encoding the p16 protein. Our results demonstrate that Delta-24-RGD can induce dramatic cytotoxicity in a subset of PDAC cell lines with high Cyclin D1 expression. Induction of autophagy & apoptosis by Delta-24-RGD in sensitive PDAC cells was confirmed with LC3B-GFP autophagy reporter and Acridine Orange staining as well as Western blotting analysis of LC3B-II expression. Notably, we found that Delta-24-RGD induced phosphatidylserine (PS) exposure in infected cells independent of cells' sensitivity to Delta-24-RGD, which renders a rationale for combination of Delta-24-RGD viral therapy and PS targeting antibody for PDAC. In a mouse PDAC model derived from a liver metastatic pancreatic cancer cell line, Delta-24-RGD significantly inhibited tumor growth compared with control (p<0.001), and combination of PS targeting antibody 1N11 [mouse version of Bavituximab] further enhanced its anticancer activity (p<0.01) possibly through inducing synergistic anticancer immune responses. Given that these 2 agents are currently in clinical evaluation, our study warrants further clinical evaluation of this novel combination strategy in pancreatic cancer therapy.
**DNX-2401: DNAtrix Corp., Houston TX http://www.dnatrix.com (private company)
“DNAtrix’s lead product, DNX-2401 is a potent oncolytic adenovirus that targets & kills cancer cells, while leaving normal cells intact. Multiple clinical studies in patients with recurrent glioblastoma and gynecologic cancer have shown that DNX-2401 has a favorable safety profile, strong tumor-killing potential, and can trigger an anti-tumor immune response.” http://www.dnatrix.com/clinical-trials
= = = = = = = = = = = = = = = =
I. Phase II Bavi+GEM vs. Front-Line Adv. PANCREATIC (randomized, unblinded, n=70)
Protocol: http://www.clinicaltrials.gov/ct2/show/NCT01272791 (15 U.S. + 4 Ukraine = 19 as of 6-7-2012)
…1-22-13: FTM's post of 13 Ph3 Gem+Treatment Pancreatic Trials ('02-'13) - Mean MOS: GEM=6.4mos., GEM+TR=7.3mos. http://tinyurl.com/al99hx9
......Another FTM Pancreatic Phase3 trials table showing HR's, P-Values, and ORR% stats: http://tinyurl.com/btzkw4l
…6-3-13 ASCO’13/final data: n=70, Ctl=>Bavi MOS 5.2=>5.6mos, ORR 13%=>28% HR=.75 http://tinyurl.com/kq3uv4e
......Promising ‘immuno-indicative’ 1yr SURVIVAL results: GEM-Only(n=31): 0%, Bavi+GEM(n=32): 24.5% - see: http://tinyurl.com/lz5yg4f
...2-13-13 Topline Data: “Bavi+Gem resulted in more than a doubling of ORR” http://tinyurl.com/aqny7ny
...6-25-12: Enrollment complete. http://tinyurl.com/72tvnfj
...6-20-12: Early data (cutoff=6/6/12 bavi=15 ctl=17) presented at AACR Pancreatic Conf. http://tinyurl.com/77m9fw2
...1-5-11: U.S. Ph.2 randomized trial initiated http://tinyurl.com/26hnuzv "up to 70 front-line patients at ~10 clinical sites."
The PPHM/DUKE(H.Lyerly) Collab: Oct’16, AntiPS+PDL1/TNBC, “Greater Anti-Tumor Responses”.
The Full Abstract from Dr. Lyerly’s 10-22-16 AACR/CRI Conf. Poster published 3-2017 in conf. proceedings. Conclusion: “PS expression is upregulated by chemotherapy, radiotherapy, and photodynamic therapy in vitro. A combination therapy of PS-targeting + Anti-PD-L1 appears superior to single agent therapy. Our future plan is to investigate the effect of local irradiation or photodynamic therapy combined with PS-targeting mAb & anti-PD-L1 Ab.”
Oct20-23 2016: “AACR’s Tumor Immunology & Immunotherapy Conf.”, Boston
http://www.aacr.org/Meetings/Pages/MeetingDetail.aspx?EventItemID=92
10-22-16 POSTER SESSION B: “Immunomodulation”
#B36 “Modulating The Tumor Microenvironment to Enhance Cancer Immunotherapy by Inducing Phosphatidylserine Expression on the Tumor Surface”
Kensuke Kaneko 1, Takuya Osada 1, Bruce D. Freimark 2, Herbert Kim Lyerly ** (Duke Univ.) 1
1=Duke University, Durham, NC
2=Peregrine Pharmaceuticals
**Dr. Herbert Kim Lyerly: https://immunology.duke.edu/people/herbert-kim-lyerly-md (Dept. of Immunology, George Barth Geller Professor, Duke Univ. MC; same dept. as Barton Haynes)
ABSTRACT (from Conf. Proceedings – pub. 3/2017):
http://cancerimmunolres.aacrjournals.org/content/5/3_Supplement/B36
BACKGROUND & HYPOTHESIS:
While immune checkpoint blockade, in particular PD-1 or PD-L1 inhibition, has revolutionized cancer immunotherapy, a significant number of patients with solid tumors fail to respond to therapy. An emerging consensus is the need for a local infiltration of immune effector T cells, in combination with PD-1 or PD-L1, for anticancer responses. We are exploring an improved strategy to modulate the tumor microenvironment by targeting phosphatidylserine (PS), which is a phospholipid membrane component maintained on the cytosolic side of the cell membrane in viable cells. When a cell undergoes apoptosis or stress induced by the microenvironment, PS is no longer restricted to the cytosolic domain and gets transposed to the extracellular surface where it serves a variety of functions, including as a ligand for another immune checkpoint, TIM-3. In fact, PS-targeting antibodies induce immunity against weakly immunogenic tumor cells (He at al, 2009), and may serve to enhance anti-cancer immunotherapy. Chemotherapy and radiation therapy are often used to treat cancers. In addition, photodynamic therapy using a photosensitizer conjugated with a target specific molecule has been recognized as an emerging therapeutic strategy. Therefore, we sought to determine the expression of PS following treatment with chemotherapy, radiation, or photodynamic therapy, and to determine if the addition of a PS-targeting antibody could augment antitumor response, especially in combination with PD-1 inhibition.
METHODS & RESULTS:
We first confirmed the upregulation of PS on malignant human cells following treatment with chemotherapy by FACS analysis using PS-targeting antibody mch1N11 [“Mouse version of Bavituximab”]. PS expression was increased (50.2% positive compared to 5.0% in untreated cells) after 18 h of incubation with etoposide (25uM). We then tested PS expression on murine triple negative breast cancer cell lines (E0771-OVA, 4T1) at days 1, 2, and 4 after a single dose of X-ray (30, 40, or 50 Gy). E0771-OVA cells showed increased PS expression at day 2, while 4T1 cell lines increased PS expression at day 4. E0771-OVA cells were also irradiated using a more conventional schedule, specifically daily administration (6 Gy/day 5 days), leading to increase PS expression. Additionally, we tested PS expression on E0771-OVA cells after photodynamic therapy using HS201, which is a synthesized photosensitizer compound constructed of verteporfin and HSP 90 inhibitor. PS expression increased at day 1 when the cells were treated with a single dose of laser (10 or 60J) after 30 minutes conjugation of HS201 (1 or 10 uM). After confirming upregulation of PS by chemotherapy, radiotherapy, and photodynamic therapy, we next tested the combination of PS-targeting mAb mch1N11 with chemotherapy in vivo. We treated C57BL/6 mice bearing E0771-OVA tumors with paclitaxel (PTX), PS-targeting mAb mch1N11, anti-PD-L1 Ab, or combination. As single agents, both mch1N11 & anti-PD-L1 mAbs showed tumor growth suppression; however, combination of those 2 and 3 combination showed stronger effect. On the other hand, PTX didn't seem to add any additional effect.
CONCLUSIONS:
PS expression is upregulated by chemotherapy, radiotherapy, and photodynamic therapy in vitro. A combination therapy blocking PS by PS-targeting mAb and immune checkpoint blockade with anti-PD-L1 mAb appears superior to single agent therapy. Our future plan [a/o 10-22-16] is to investigate the effect of local irradiation or photodynamic therapy combined with PS-targeting mAb & anti-PD-L1 Ab.
------------
10-22-16: Duke’s Herbert K. Lyerly (w/PPHM) poster on AntiPS/TNBC data at AACR’s Tumor Immunotherapy Conf./Boston - ”Modulating The Tumor Microenvironment to Enhance Cancer Immunotherapy by Inducing Phosphatidylserine Expression on the Tumor Surface” http://tinyurl.com/zzryfok
From the PPHM PR: “Peregrine… announced the presentation of preclin. study data demonstrating that PS-targeting antibodies similar to bavituximab are able to enhance the anti-tumor activity of anti-PD-L1 therapy in a model of triple neg. breast cancer (TNBC). Data showed that a combination of anti-PS & anti-PD-L1 therapies, with or without paclitaxel, led to greater anti-tumor responses than any of the treatments administered as single agents or dual treatment combinations with paclitaxel, in the well-characterized E0771 murine model of TNBC. Study results were presented by researchers from Duke University Medical Center [Senior Author: Dr. Herbert Kim Lyerly] at the AACR’s “Tumor Immunology & Immunotherapy Conf.”, Oct. 20-23, 2016 in Boston.
In addition to evaluating the anti-tumor activity of the various treatment combinations, researchers also examined the impact of various traditional cancer therapies on PS expression in cancer cells. Study results confirmed that levels of PS expression were upregulated in E0771 & 4T1 TNBC cells following treatment with chemotherapy, radiation or photodynamic therapy. Photodynamic therapy also was shown to increase PS expression on tumor cells.
DR. JEFF HUTCHINS(VP/Preclin.):
"These study results provide the latest support for the belief that PS-targeting therapies can enhance the anti-tumor activity of checkpoint inhibitors such as anti-PD-L1 therapy in the treatment of TNBC. Just last month [9-27-16 AACR/CRI: http://tinyurl.com/zy9yv78 ], we announced results from another preclinical study in TNBC demonstrating that 80% of animals receiving the triple combination of anti-PS, anti-PD-1 and anti-LAG3 therapies experienced complete tumor regressions, whereas there were no animals in the anti-PD-1 and anti-LAG3 combination treatment arm that had a complete regression. Additionally, these latest study findings related to increased PS expression on the surface of tumor cells following traditional cancer treatments demonstrate important activity within the tumor microenvironment that offers rationale for the potential of anti-PS agents in combating cancer. We plan to continue to work with our collaborators at Duke University Medical Center to further study the therapeutic potential of PS-targeting agents in combination with checkpoint inhibitors like anti-PD-L1 and conventional therapies that augment immunotherapy mechanisms."
= = = = = = = = = = = = = = = = = = = = = = = = = =
RECALL:
11-9-15 SITC'15: New Bavi+Checkpoint Inhibitors preclin. data (UTSW/DUKE's Herbert K. Lyerly) http://tinyurl.com/pbof95w
...Also, collab. with Dr. Bernard Fox (Immunotherapist/Earle A. Chiles Res.Inst.) on new Immuno-Profiling Clinical Test (Opal 6-plex quantitative IF Assay), PPHM roundtable with Raymond Birge (Rutgers), Douglas Graham (Emory), Dmitry Gabrilovich (Wistar), Rolf Brekken (UTSW), Maria Karasarides (AstraZeneca) - ”Combining Bavi w/anti-PD-1 significantly enhanced O/S… significant incr. CD45+, CD8+ and CD3+ T-cells… led a prolonged anti-tumor immune response which protected the animals against a re-challenge w/same tumor.”
Tradero, I now see exactly where you were heading with your original question. It didn't occur to me that Dr. Schroit could have had Sunrise pt. blood samples tested with his Exosomes approach as well - no reason why that couldn't have been done. CP's #289106 really explained that possibility well, in ways that never occurred to me.
Tradero, those tests of Sunrise patient samples would have been for the Biomarkers project, not the Exosomes project.
Ie, THIS:
http://investorshub.advfn.com/boards/read_msg.aspx?message_id=129157843
NOT:
http://investorshub.advfn.com/boards/read_msg.aspx?message_id=128560007
.
.
= = = = = = = = = = =THIS:
10-10-16(JOE SHAN/VP=Reg+Clin.Affairs):
"We would once again like to thank all of the patients, clinical investigators & scientists who participated in the SUNRISE trial and have made it possible for us to continue to collect and analyze a range of key data from the study. While we were disappointed with the trial being discontinued earlier in the year, we are excited by the fact that we are beginning to learn important information from the trial through the ongoing Biomarker analysis program that will be critical in helping guide the future clinical development of bavituximab. It is encouraging that the initial biomarker analysis has identified an important biomarker early in the process and we are optimistic that additional biomarkers associated with improved outcomes for bavituximab-containing treatments will be identified as the analysis continues. We expect to be able to share the emerging data over the coming months at scientific & medical conferences as the more results become available.”
=============NOT THIS:
PPHM's EXOSOME-BASED (PS Positive) CANCER DETECTION & MONITORING TECHNOLOGY ("Liquid Biopsy")
...Excellent Exosome (aka microparticles, microvesicles) info: http://www.exosome-rna.com
2-9-17/PR: PS+ Exosomes Proof-of-Concept Data (N=44, Ovarian, Dr. Alan Schroit/UTSW etal) Published 1-22-17 in OncoTarget http://tinyurl.com/jhv57ua
...Data (blinded plasma from 34 O.C. pts & 10 healthy subjects) supports the “high diagnostic power” of PS+ Exosomes in Ovarian Malignancies.
...Dr. Stephen Worsley (VP/BusDev): “...we believe this has potential applications in several solid tumors beyond ovarian cancer. With that in mind, we look forward to aligning with a partner to help explore the potential of this promising technology."
...PPHM’s PS Exosomes platform advantages outlined: UTSW/website & World Patent #WO/2016/201064: http://tinyurl.com/zbwr7cc
7-14-16: Peregrine Licenses Exosome-based technology from UTSW (Inventors: Alan Schroit/Philip Thorpe) http://tinyurl.com/zszd4fj
...“relates to assays that are able to detect small amts of PS+ Exosomes in a patient's blood sample as a way to detect cancer at a very early stage of development.”
...Dr. Jeff Hutchins (VP/PreclinRES): "Once we have successfully validated this assay, we plan to establish proof-of-concept through an efficient preclinical & clinical testing pgm. We have no intention of conducting further development work beyond the proof-of-concept stage. Rather, we expect to initiate partnering discussions for commercialization of this pgm in 2017."
12-12-16 CEO/S.King: “We are actively evaluating addl. potential biomarkers [beyond #1/B2GPI] and we hope to identify a profile for patients who will receive therapeutic benefit from treatment with bavituximab.”
Halozyme, “working to scale-up/validate/qualify” Avid II(Myford), as a manufacturer of bulk rHuPH20 under the Roche Collaboration, per their 12-31-16 10-K issued 2-28-17. (Thx for the find, BioBS2012 #288235).
HALO’s 12-31-16 10-K, iss. 2-28-17 (pg.12):
“In addition, we are working to scale-up, validate, and qualify a new facility operated by Avid [Avid II, “MYFORD”] as a manufacturer of bulk rHuPH20 for use in the products & product candidates under the Roche Collaboration.”
Pg.9: ROCHE COLLABORATION:
“In Dec. 2006, we and Roche entered into a collaboration & license agreement under which Roche obtained a worldwide, license to develop & commercialize product combinations of rHuPH20 and up to 13 Roche target compounds (the Roche Collaboration). Roche initially had the exclusive right to apply rHuPH20 to 3 pre-defined Roche biologic targets with the option to develop & commercialize rHuPH20 with 10 addl. targets. Roche had the right to exercise this option to identify addl. targets for 10 years. As of the 10 year anniversary of the Roche Collaboration in Dec. 2016, Roche had elected a total of 8 targets, 2 of which are exclusive.”
12-31-16 10-K: https://www.sec.gov/Archives/edgar/data/1159036/000115903617000014/halo-12312016x10k.htm
HALO: http://www.halozyme.com
...About rHuPH20: http://www.halozyme.com/technology-and-products/technology/technology
- - - - - - - - - - - -
12-12-16/CC/S.King: “Our 2 facilities have the potential to generate in excess of $80mm in revenue, leaving addl. capacity for revenue growth beyond the current FY and into next year. Even with this available capacity, we are moving forward with our plans to construct a 3rd Mfg. Facility in order to meet the anticipated commercial needs of our clients, while continuing to grow the business by bringing in new projects.” Current revenue backlog: $73mm, under signed contracts. http://tinyurl.com/hhn4gga
3-9-16/Qtly-PR: “Avid’s new state-of-the-art commercial bio-mfg. suite has been formally commissioned. The new facility will double the company’s prior mfg. capacity, supporting up to an addl. $40mm in revenue each year.” http://tinyurl.com/gom7md5
3-7-16/Avid II: Formal Commissioning of Avid's New 40,000sq "Myford" Facility, “single-use/fully disposable” (potentially $40M addl revs) – S.King: “We have already had a tremendous response to the new facility and look forward to continuing to grow our bio-mfg. business which is an integral part of our overall business strategy." http://tinyurl.com/za2j9mt
12-11-15/BioPharma: Avid Expansion into MYFORD Facility (Avid II) now GMP-run ready (potential +$40mm sales) - contemplating further expansion http://tinyurl.com/z35623w
12-10-15/CC – Robert Garnick: “With the Myford site (Avid II) now in the initial phase of GMP manufacturing, we have seen a significant increase in demand for production capacity. Although, we have just opened the doors at Myford, we are already contemplating our options to increase further mfg. Capacity. Although no decisions have been made, we are pleased to have what appears to be a growing opportunity in this important area of our business.” http://tinyurl.com/jkp885g

= = = = = = = = = = =
AVID BIOSERVICES, Inc. (Peregrine's Mfg. Subsidiary): http://www.avidbio.com
12-12-16: PPHM's Revs & Burns By Qtr Table, FY'07/Q1 thru FY'17/Q2 (q/e 10-31-16): http://tinyurl.com/hhn4gga (since 5-2006: Avid=$202.5mm, Total=$229.1mm, incl.Govt)
......Avid FY17 (fye 4-30-17) revs guidance: $50-55mm; committed 12-12-16 backlog: $73mm. Avid III being designed/already secured 25,000sf loc/expect compl=Late/2017. “Expect future sustainable profitability for the co. in 18mos.”
6-2-16: Corp.Update – Avid Expansion & Drug Development - http://tinyurl.com/zvmhqmr
5-23-16: Pete Gagnon (100pubs/presentations, 12+patents, 30 pending patents) Appointed VP/Process-Services of Avid http://tinyurl.com/hg6abdq – See Oct'15:
Avid picking up Xencor would be nice: 1.2B/Mktcap
http://finance.yahoo.com/quote/XNCR
http://www.xencor.com "Antibodies By Design"
4-15-16: “Since 2012, Mr. Stafford has served as CEO of Ronin Trading LLC. He has also previously served as a board member of Xencor, Inc.”
http://people.equilar.com/bio/john-stafford-aware--inc./salary/499190
Xencor 10K iss. 3-1-17: “We expect to move mfg. services to another contract mfg. organization to support late-stage clinical trials for XmAb5871 as well as commercial supplies.”
Error, CP: the Bavi+RAD+Sorafenib Hepatocellular trial start date was moved to April 30th, not April 1st.
9-6-16: NCCN Awards 3 Bavi Trials, to begin "Early 2017" http://tinyurl.com/gutgwb5
...1: Ph1/Hepatocellular Cancer (Bavi+RAD+Sorafenib), MOFFITT CANCER CENTER, PI: Jessica Frakes, MD (Clinicaltrials has start=4-30-17) https://clinicaltrials.gov/ct2/show/NCT02989870
...2: P1-2/Glioblastoma (Bavi+RAD+Merck’s Temodar), MASS-GEN. CC, PI: Elizabeth Gerstner, MD
...3: Ph2/Head+Neck (Bavi+Merck’s Keytruda), JOHN-HOPKINS(Sidney Kimmel CC), PI: Ranee Mehra, MD
Mem.Sloan/Wolchok, Biomarkers, NCCN/AZN Trials – tightly related imo...
CHRONOLOGICALLY:
5-29-15: Peregrine & Sloan Kettering Enter Collab. to “Investigate Novel PS-Targeting Immunotherapy Combos” http://tinyurl.com/o3k9ux8
JEDD WOLCHOK: ”The phosphatidylserine (PS) signaling pathway is a very interesting target for modulating the immune system's response to cancer. We look forward to exploring the potential of PS-targeting agents alone and with other immune modulators that may lead to novel advances in cancer therapy."
8-24-15: Peregrine & AstraZeneca & Peregrine Enter Collab. to run Ph1/Bavi+Durva/mult. solid tumors http://tinyurl.com/owlxpsf
...and then: 10-15-15: Peregrine & AstraZeneca Expand Collab. to run Ph2/Bavi+Durva/2L_NSCLS http://tinyurl.com/q79bkam
1-6-16: Peregrine enters into Research Collab. with NCCN http://tinyurl.com/zmxtpsb
1-11-16: Peregrine Plans Expansion of Bavi Clinical Pgm http://tinyurl.com/zhdy37a
...New Ph2/Bavi+Chemo/TNBC, which “originated from Peregrine's ongoing collab. W/MSKCC”. One site will be Providence CC/Portland w/P.I.=David Page.
Note1: ProvidenceCC was a SUNRISE site w/P.I.=Rachel Sanborn(Dir./Thoracic-Onology, Providence CC).
Note2: David Page worked & published w/J.Wolchok at MSKCC – ex: http://www.hemonc.theclinics.com/article/S0889-8588(14)00017-3/abstract
9-6-16: NCCN Awards 3 Bavi Trials, to begin "Early 2017" http://tinyurl.com/gutgwb5
...1: Ph1/Hepatocellular Cancer (Bavi+RAD+Sorafenib), MOFFITT CANCER CENTER, PI: Jessica Frakes, MD (Clinicaltrials has start=4-30-17)
...2: P1-2/Glioblastoma (Bavi+RAD+Merck’s Temodar), MASS-GEN. CC, PI: Elizabeth Gerstner, MD
...3: Ph2/Head+Neck (Bavi+Merck’s Keytruda), JOHN-HOPKINS(Sidney Kimmel CC), PI: Ranee Mehra, MD
10-10-16/ESMO’16: Sunrise Biomarker #1 (B2GPI) announced http://tinyurl.com/hp73njt
...”We are optimistic that addl. Biomarkers associated with improved outcomes for bavituximab-containing treatments will be identified as the analysis continues.”
12-7-16/IASLC’16/Vienna: Sunrise Biomarker #2 (Complement Act. & IL-10) revealed in abstracts, but withdrawn due to “data anal. not complete”(IR) http://tinyurl.com/z8cq8vx
...LEAD AUTHOR: David E. Gerber/UTSW, SENIOR AUTHOR: Rachael Sanborn/ProvidenceCC
12-12-17/CC/S.King: “We are currently evaluating addl. Biomarkers that we hope will allow us to identify a profile for patients who will receive therapeutic benefits from a bavituximab-containing treatment regimen.” http://tinyurl.com/hhn4gga
3-1-17/AACR’17: Sunrise Biomarker #3 (INF-y) revealed in abstracts http://tinyurl.com/zdsbds8
...LEAD AUTHOR: N.Kallinteris (PPHM), SENIOR AUTHOR: Rachael Sanborn/ProvidenceCC
= = = =MY OPINIONS:
1. In think the newly revealed 4-3-17 AACR’17 Biomarker #3 (IFN-y) supplants the previous two. I think they kept searching for better & better ones, and #3 is the latest & greatest. Thus, it’s THE ONE they chose to show off at AACR’17.
2. I think that Jedd Wolchok and his Lab are deeply involved with helping PPHM put together the final protocol’s for the 3 NCCN trials and the planned AZN “Mult. Tumor Types” trial. You see Providence CC’s Dr. Rachael Sanborn appear as Senior Author of the last 2 Biomarker Abstracts, with ties back to MSKCC/Wolchok thru Providence Co-Oncologist David Page, who prev. worked with Dr. Jedd at Mem.Sloan. PPHM+MSK+PROVIDENCE, tightly working together on future Bavi Trials.
3. No better evidence as to how close PPHM & Mem.Sloan/Wolchok have become than to look at AACR’17 (See http://tinyurl.com/zzldh9n ). The new (2nd) PPHM+MSK study revealed by the 3-1-17 abstracts is a complete mindblower (to me!):
#2. MSKCC+PPHM: 4-3-17 #1651, “PSTargeting+Adoptive TCell Transfer (ACT) Eliminates Adv. Tumors w/o Off-Target Toxicities, Melanoma” <=NEW(2nd) Joint MemSloan/PPHM study, see: http://tinyurl.com/h3ylrku

.
.
= = = = = = = = = = = = = = = = = = = =
Dr. Wolchok spoke about Bavi in the 11-14-16/PR (SITC’16, Joint MSKCC & PPHM Poster, “Phosphatidylserine Targeting Antibody in Combination with Checkpoint Blockade & Tumor Radiation Therapy Promotes Anti-Cancer Activity in Mouse Melanoma”)…
FULL SITC’16 ABSTRACT #199: http://bit.ly/2dHTEVn
11-14-16/JEDD WOLCHOK: "Based on these study results, we believe that the targeting of PS is having meaningful activity within the tumor microenvironment in the B16 melanoma model. It appears that this activity creates a more immune active environment in which other treatments, including radiation, are able to have a greater anti-tumor impact." http://tinyurl.com/js3fca4
11-14-16/TAHA MERGHOUB (Co-Dir., MSK’s Ludwig Collab. Lab): "We have noted that the combination of PS-targeting treatment and radiation, as well as triple combination of PS-targeting treatment, radiation and anti-PD-1, resulted in clear advantages in anti-tumor activity in the mouse B16 melanoma model. We believe that these findings suggest the potential benefit of combining these agents to improve the outcomes of patients with cancer. With this in mind, we think this research may play an important role in designing future clinical trials of PS-targeting agents in melanoma and other cancers." http://tinyurl.com/js3fca4

