 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.


Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
* * * $TTPH Chart Analysis * * *

https://www.sec.gov/cgi-bin/browse-edgar?CIK=TTPH&owner=exclude&action=getcompany
TTPH News: Written Communication Relating to an Issuer or Third Party (sc To-c) 08:51 AM
TTPH News: Amended Statement of Ownership: Solicitation (sc 14d9/a) 06:22 AM
TTPH News: Current Report Filing (8-k) 06:14 AM
TTPH News: Tetraphase Announces Receipt of Proposal from La Jolla Pharmaceutical Company, Determination of Superior Offer & Notice to Me... 06:00 AM
the algo's just wont let it rebreak 3.25 again here......BULLS need to push
On June 4, 2020, Tetraphase Pharmaceuticals, Inc. (the “Company”) received notice that the United States Food and Drug Administration (the “FDA”) approved the Company’s supplemental New Drug application (“sNDA”) for a new strength of XERAVATM (eravacycline) for injection for the treatment of complicated intra-abdominal infections in adult patients containing 100mg of eravacycline per vial as well as an extension of the “in-use” shelf life for XERAVA diluted ready for infusion IV solution from 7 days to 10 days under refrigerated conditions for the existing 50 mg/vial product and for the newly approved 100 mg/vial product.
https://ih.advfn.com/stock-market/NASDAQ/tetraphase-pharmaceuticals-TTPH/stock-news/82607977/current-report-filing-8-k
Melinta Therapeutics to Acquire Tetraphase Pharmaceuticals
https://ih.advfn.com/stock-market/NASDAQ/tetraphase-pharmaceuticals-TTPH/stock-news/82601296/melinta-therapeutics-to-acquire-tetraphase-pharmac
Do the shareholders get to vote to take the Melinta deal? When is the voting?
all cash deal, won't be any ttph shareholders is my understanding
Melinta is the most corrupt company in the world- screwed their shareholders completely-- they will screw TTPH shareholders as well - until TTPH is also bankrupt. Better to stick with ACRX
Looks good. On June 1, 2020, the Company announced that its Board of Directors has determined that the Amended Melinta Proposal to acquire the Company is a “Superior Offer” under the terms of the AcelRx Merger Agreement. In connection with this determination and in accordance with the terms of the AcelRx Merger Agreement, the Company has given notice to AcelRx of such determination and of its intention to consider changing its recommendation of the AcelRx Merger Agreement or terminating the AcelRx Merger Agreement unless AcelRx proposes revisions to the terms of the AcelRx Merger Agreement or makes another proposal on or prior to Wednesday, June 3, 2020 that, if accepted, would result in the Amended Melinta Proposal ceasing to be a Superior Offer. A copy of the press release is attached as Exhibit 99.1 hereto and is incorporated herein by reference. TTPH
Hey where is everybody? The new math- Melinta gozinta tetra phase 39 million carry the nought
Much better, though.still a steal.
pathetic offer goes even lower if TTPH cash balance dips below 5 mil., but they don't say by how much, this is an illusory offer.
Not in interest of shareholders. Management says so because they get paid for the warrants too.
They get more money, we get less and we get more dilution. This is a total ripoff.
ACRX burn rate ate all their cash. We get to hold their stock which is undercapitalized. while they get our 5 mil and all our tech and product pipeline, but I forgot, they might give us a royalty on our products, that's so very nice of them. This needs a NO VOTE.
acrx is using ttph's cash to help buy it (the 5 mil)
notice they never say how many shares outstanding when determining the cvr value per share.
the .72 shares are these existing or newly issued? more dilution?
They get their hands on our 5 mil cash and it costs them basically nothing.
They just issue stock. Then the little bit we may get from the c.v.r. is revenue generated from OUR products. which they keep the lion's share
They are not coming up with anything except .59 cents a share. How much of that is from our 5 mil.
This is a superior offer?
Well if someone offers you crap, and then someone else offers you crap with 3 grains of sugar on it, well then you could say the latter was a "superior" offer.
https://www.businesswire.com/news/home/20200527005568/en/Tetraphase-Announces-Amendment-Merger-Agreement-AcelRx-Pharmaceuticals/?feedref=JjAwJuNHiystnCoBq_hl-RLXHJgazfQJNuOVHefdHP-D8R-QU5o2AvY8bhI9uvWSD8DYIYv4TIC1g1u0AKcacnnViVjtb72bOP4-4nHK5ieT3WxPE8m_kWI77F87CseT
https://www.prnewswire.com/news-releases/acelrx-pharmaceuticals-announces-revised-merger-agreement-with-tetraphase-301067693.html
TTPH
ACRX
smart move...offer going up...........
I am still holding all my TTPH shares. I figured there was no way they would sell below $5.00 or more as you show below. I do not understand the selling anywhere below $3.00 to $4.00, $5.00 etc.
ACRX has until Friday to counter offer. Melinta's offer of 27 mil. in cash equates to about 3.70 a share
at 7.3 mil shares outstanding plus they also had extras of 12 mil. or 1.65 which puts it over 5 bucks a share, a double from here.
ACRX has until Friday to counter offer. Melinta's offer of 27 mil. in cash equates to about 3.70 a share
at 7.3 mil shares outstanding plus they also had extras of 12 mil. or 1.65 which puts it over 5 bucks a share, a double from here.
No thanks Gaytrader.
* * $TTPH Video Chart 05-22-2020 * *
Link to Video - click here to watch the technical chart video
* * $TTPH Video Chart 05-15-2020 * *
Link to Video - click here to watch the technical chart video
With the current AcelRx deal conversion of .60 share for every TTPH share, isn't it better to just buy AcelRx share right now? Not considering CVR as it is not guaranteed.
* * $TTPH Video Chart 05-07-2020 * *
Link to Video - click here to watch the technical chart video
Market makers do naked shorts. They create more shares than there are. This is supposed to be illegal.
This is one theory. Inescapable not to conclude. They short the shit today above three and sell it back down under 2.50
Could be covering now. Otherwise you would think it would be 4 or 5 dollars.
I know there is a lot of in and out trading. Would be surprised if that's all it was.
Easy--- the merger was contingent upon shareholder approval which vote is set for June 20. 2020.
So, they are not committed to anyone at this point
hoes does a stock with 8M outstanding trade over 40M volume??
TTPH
how does TTPH back out of their other signed offer?
What I hate=Assholes that use the words "non binding" when making offers.
He made an effort to put it in there.
Seen it before many times, last one was srne
Granted the guy would look like a jerk if it does not go through.
Does not help the longs
Legally all it is a an offer to negotiate.
Maybe this guy is a nice guy and sincere.
I hope he knows how many people he is messing with if he is playing games.
i like the potential CVR of $12.5m. at 7.3m shares outstanding, this makes the pps of $4.72. we are still below $3.00. still a strong buy imo.
https://www.investopedia.com/terms/c/cvr.asp
Acquisition offer news
What’s the story here
$TTPH , A No Brainer buy here
TTPH—(+69%/AH)—receives unsolicited buyout offer from LJPC that trumps ACRX’s buyout deal announced on 3/16/20 (#msg-154357912):
https://www.sec.gov/Archives/edgar/data/920465/000092046520000067/exhibitfy20tetraphase.htm
Quote:
On behalf of La Jolla Pharmaceutical Company, I am pleased to submit this non-binding proposal to acquire 100% of the equity of Tetraphase Pharmaceuticals, Inc. for $22 million in cash plus an additional $12.5 million potentially payable under CVRs to be issued in the transaction. The $22 million upfront consideration would include amounts payable under the Black-Scholes put provisions in Tetraphase’s outstanding warrants and be subject to a minimum, to-be-agreed-upon closing net cash balance.
The terms of the CVRs would match those set forth in Tetraphase’s merger agreement with AcelRx Pharmaceuticals, Inc., except that payments pursuant to the CVRs would be made in cash instead of cash or stock at the acquiror’s option.
*** TTPH Analysis 5/4/2020 ***
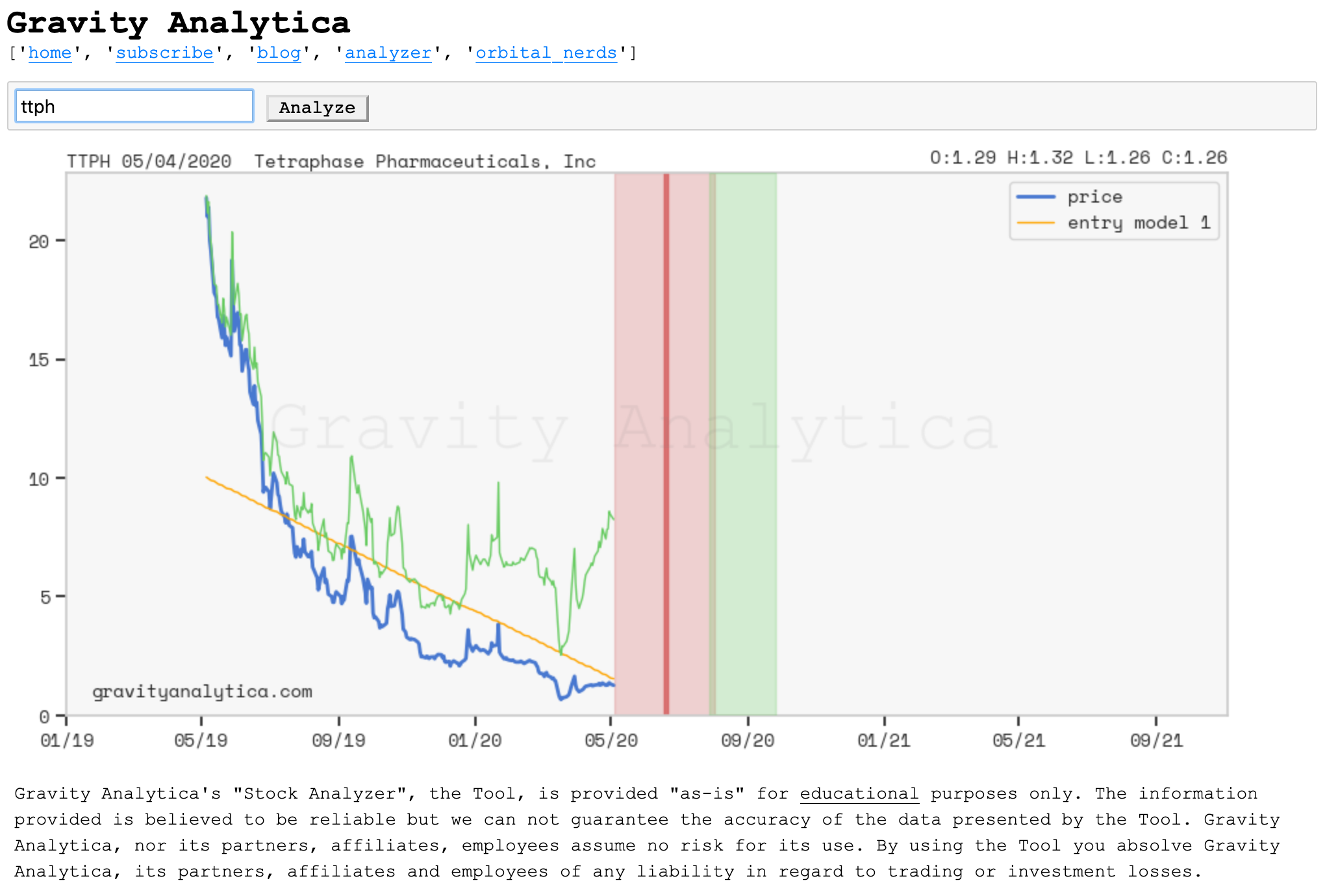
GA
Several promising known drugs stand out as potential inhibitors of SARS-Cov-2 main protease, including Carfilzomib, Eravacycline, Valrubicin, Lopinavir and Elbasvir. Carfilzomib, an approved anti-cancer drug acting as a proteasome inhibitor, has the best MM-PBSA-WSAS binding free energy, -13.8 kcal/mol. The second-best repurposing drug candidate, eravacycline, is synthetic halogenated tetracycline class antibiotic.
https://pubs.acs.org/doi/10.1021/acs.jcim.0c00179
Interesting - haven't been following closely, but I would look at the insty holders in both as they are probably calling the shots.
What are the synergies?
Does one have a stronger IP position than the other?
These are just the first questions that come to mind.
Will investigate if I have time, it's always nice to learn about these things even if you don't have a position.
TTPH merging with acrx - 1 share of ttph gives .63 shares of acrx. That being said, ttph and acrx are almost trading at the same price right now. That makes no sense ??
* * $TTPH Video Chart 03-30-2020 * *
Link to Video - click here to watch the technical chart video
This might be a hidden gem the next week or two.. some big boys just picked up an abundant amount and they have good track records.
This one's getting carved up by the Big Boys..
2020-01-31 13G INTRACOASTAL CAPITAL, LLC 725,657 9.40
2020-01-31 13G CVI Investments, Inc. 666,666 9.40
2020-01-28 13G Sabby Management, LLC 666,667 9.37
2020-01-23 13D ARMISTICE CAPITAL, LLC 1,419,507 19.90
2019-07-10 13G/A BlackRock Inc. 1,267,370 2.30
2019-01-30 13G/A INTEGRATED CORE STRATEGIES (US) LLC 11,409 0.00
* * $TTPH Video Chart 12-27-2019 * *
Link to Video - click here to watch the technical chart video
* * $TTPH Video Chart 12-26-2019 * *
Link to Video - click here to watch the technical chart video
What happened here that’s lower than ever been
* * $TTPH Video Chart 09-12-2019 * *
Link to Video - click here to watch the technical chart video
Greetings All bet these products will save A lot of Lives,pray for their Success, Peace
|
Followers
|
45
|
Posters
|
|
|
Posts (Today)
|
0
|
Posts (Total)
|
2296
|
|
Created
|
04/08/13
|
Type
|
Free
|
| Moderators | |||
NASDAQ: TTPH

• Tetraphase's lead candidates have the potential to treat a broad range of serious bacterial infections. This provides a tremendous opportunity to address the global health crisis caused by the increasing number of infections resistant to currently used antibiotics.
• The Tetraphase proprietary drug discovery engine has produced more than 3,000 proprietary compounds with novel molecular structures, reinvigorating one of the best known, safest and most efficacious classes of antibiotics ever discovered.
• Since inception, Tetraphase has developed a strong pipeline with a broad-spectrum antibiotic lead candidate in Phase 3 clinical trials and several additional candidates in preclinical development.
Tetraphase Pipeline
Tetraphase has been using its proprietary chemistry technology to build a pipeline of antibiotic candidates to address the serious and growing unmet medical need in the treatment of multidrug-resistant bacterial infections.

Eravacycline
We are developing our lead product candidate, eravacycline, as a broad-spectrum intravenous and oral antibiotic for the treatment of multidrug-resistant (MDR) infections, including those caused by MDR Gram-negative bacteria. We developed eravacycline using our proprietary chemistry technology. Eravacycline is a novel, fully synthetic tetracycline antibiotic. We are currently investigating the safety and efficacy of eravacycline in a Phase 3 program called IGNITE (Investigating Gram-negative Infections Treated with Eravacycline) for the treatment of complicated intra-abdominal infections (cIAI)(IGNITE 1) and complicated urinary tract infections (cUTI)(IGNITE 2).
TP-271
TP-271, a novel antibiotic currently in preclinical development, is being developed to combat respiratory disease caused by bacterial biothreats and antibiotic-resistant public health pathogens. As development continues, TP-271 is anticipated to protect against certain biothreats agents, including Francisella tularensis, which causes tularemia; Yersinia pestis, which causes bubonic plague; Bacillus anthracis, which causes anthrax disease; and bacterial pathogens associated with community-acquired bacterial pneumonia (CABP).
We are developing TP-271 with the financial assistance of the National Institutes of Health’s (NIH) National Institute of Allergy and Infectious Diseases (NIAID), which awarded us a $36 million contract in October 2011 to support TP-271's development, manufacturing, and clinical activities, from which we may receive up to approximately $13 million in funding.
TP-6076 (2nd Generation Gram-negative Program)
We are using our proprietary chemistry technology to pursue the discovery and development of additional tetracycline-derived compounds effective against the most urgent multidrug-resistant Gram-negative bacterial health threats identified by the CDC in a September 2013 report. Pathogens targeted include carbapenem-resistant variants of Klebsiella pneumoniae, Acinetobacter baumanni, Escherichia coli and Pseudomonas aeruginosa. We have generated compounds that have demonstrated potent activity against a broad range of these multidrug-resistant Gram-negative pathogens. We have identified TP-6076 as a lead preclinical candidate from these compounds and are currently evaluating it in IND-enabling studies.
Eravacycline
We are developing our lead product candidate, eravacycline, as a broad-spectrum intravenous and oral antibiotic for the treatment of multidrug-resistant (MDR) infections, including those caused by MDR Gram-negative bacteria. We are currently investigating the safety and efficacy of eravacycline in a Phase 3 program called IGNITE (Investigating Gram-negative Infections Treated with Eravacycline) for the treatment of complicated intra-abdominal infections (cIAI)(IGNITE 1), and complicated urinary tract infections (cUTI)(IGNITE 2). We reported top-line data from IGNITE 1 in December 2014 and expect top-line data for from IGNITE 2 in the third quarter of 2015. We target a U.S. regulatory submission for eravacycline for both indications by the end of 2015.
Eravacycline has been designated by the FDA as a Qualified Infectious Disease Product, or QIDP, for both the cIAI and cUTI indications. The QIDP designation makes eravacycline eligible for priority review and an additional five years of U.S. market exclusivity, if approved. In April 2014, the FDA granted Fast Track designations for both the cIAI and cUTI indications and the IV and oral formulations of eravacycline. Fast Track designation is awarded to expedite the study and regulatory review of drugs intended to treat serious or life-threatening conditions that demonstrate the potential to address unmet medical needs.
Eravacycline is a novel, fully synthetic tetracycline antibiotic. We selected eravacycline for development from tetracycline derivatives that we generated using our proprietary chemistry technology on the basis of the following characteristics of the compound that we observed in in vitro studies of the compound:
In in vitro studies, eravacycline has been highly active against emerging MDR pathogens like Acinetobacter baumannii as well as clinically important species of Enterobacteriaceae, including those isolates that produce ESBLs or that are resistant to the carbapenem class of antibiotics, and anaerobes.
Based on in vitro studies we have completed, eravacycline shares a similar potency profile with carbapenems except that it more broadly covers Gram-positive pathogens like MRSA and enterococci, is active against carbapenem-resistant Gram-negative bacteria and unlike carbapenems like Primaxin and Merrem is not active against Pseudomanas aeruginosa. Eravacycline has demonstrated strong activity in vitro against Gram-positive pathogens, including both nosocomial and community-acquired methicillin susceptible or resistant Staphylococcus aureus strains, vancomycin susceptible or resistant Enterococcus faecium and Enterococcus faecalis, and penicillin susceptible or resistant strains of Streptococcus pneumoniae. In in vitro studies for cIAI, eravacycline consistently exhibited strong activity against enterococci and streptococci. One of the most frequently isolated anaerobic pathogens in cIAI, either as the sole pathogen or often in conjunction with another Gram-negative bacterium, is Bacteroides fragilis. In these studies eravacycline demonstrated activity against Bacteroides fragilis and a wide range of Gram-positive and Gram-negative anaerobes.
Key Differentiating Attributes of Eravacycline
The following key attributes of eravacycline, observed in clinical trials and preclinical studies of eravacycline, differentiate eravacycline from other antibiotics targeting MDR infections.
Additionally, in February 2012, Tetraphase announced a contract award from the Biomedical Advanced Research and Development Authority (BARDA) worth up to $67 million for the development of eravacycline, from which Tetraphase may receive up to approximately $40 million in funding. The contract includes pre-clinical efficacy and toxicology studies; clinical studies; manufacturing activities; and associated regulatory activities to position the broad-spectrum antibiotic eravacycline as a potential empiric countermeasure for the treatment of inhalational disease caused by Bacillus anthracis, Francisella tularensis and Yersinia pestis. The funding under the BARDA Contract is also being used for certain activities in the development of eravacycline to treat certain infections caused by life-threatening multidrug-resistant bacteria.
Antibiotics

Antibiotics that treat bacterial infections can be classified as broad-spectrum or narrow-spectrum. Antibiotics that are active against a mixture of Gram-positive, Gram-negative and anaerobic bacteria are referred to as broad-spectrum. Antibiotics that are active only against a select subset of bacteria are referred to as narrow-spectrum. Because it usually takes from 24 to 72 hours from the time a specimen is received in the laboratory to definitively diagnose a particular bacterial infection, physicians may be required to prescribe antibiotics for serious infections without having identified the bacteria. As such, effective first-line treatment of serious infections requires the use of broad-spectrum antibiotics with activity against a broad range of bacteria at least until the bacterial infection can be diagnosed.
Many strains of bacteria have mutated over time and have developed resistance to existing drugs, resulting in infections that are increasingly serious or more difficult to treat. These drug-resistant pathogens have become a growing menace to all people, regardless of age, gender or socioeconomic background. They endanger people in affluent, industrial societies like the United States, as well as in less-developed nations. Gram-positive bacteria that have developed resistance to existing drugs include:
Gram-negative bacteria that have developed resistance to existing drugs include:
Reducing MRSA, a Gram-positive bacterium, in both the healthcare and community settings continues to be a high priority for the Centers for Disease Control and Prevention, or CDC. However, encouraging results from a CDC study published in the Journal of the American Medical Association and other reports such as the March 2011 CDC Vital Signs article provide evidence that rates of invasive MRSA infections in the United States are being controlled by Gram-positive drugs and falling.
As such, at present, the more acute need is for new drugs to treat multi-drug resistant Gram-negative bacteria. Currently approved products, such as Merrem and Levaquin are becoming increasingly ineffective against Gram-negative bacteria due to increasing resistance, limiting patients’ treatment options, particularly for patients with multi-drug resistant infections, and few new therapeutic agents are in clinical development. A survey of infectious disease specialists published in the June 2012 edition of Clinical Infectious Disease rated multi-drug resistant Gram-negative infections as the most important unmet clinical need in current practice, significantly outranking infections caused by MRSA and multi-drug resistant Mycobacterium tuberculosis. In the survey, 63% of physicians reported treating a patient in the past year whose bacterial infection was resistant to all available antibacterial agents. This resistance was confirmed by the SENTRY Antimicrobial Surveillance Program, which evaluated Enterobacteriaceae and Acinetobacter spp., two Gram-negative species of bacteria, from 31 U.S. medical centers from 2005 to 2009. Specifically, the SENTRY Program found that, with respect to the Enterobacteriaceae family of bacteria, 6.8% of the Escherichia coli strains studied and 15.4% of the Klebsiella spp. strains studied exhibited an extended-spectrum beta lactamase, or ESBL, phenotype, and that 22.2% of Enterobacter spp. strains studies were ceftazidime-resistant. ESBLs are enzymes present in certain multi-drug resistant bacteria that destroy classes of beta lactam antibiotics, such as penicillins, cephalosporins and carbapenems. In addition, Klebsiella pneumoniae carbapenemase, or KPC, producing bacteria have emerged as a highly drug resistant Gram-negative bacteria associated with mortality rates ranging from 32% to 48%, as compared to 9% to 17% for strains of Klebsiella pneumoniae that are not carbapenem-resistant.
As a further example of the seriousness of the threat of Gram-negative bacteria resistant to all available antibacterial agents, in 2012, the national media including The New York Times, The Wall Street Journal and The Washington Post reported that the Clinical Center of the National Institutes of Health had an outbreak of Gram-negative Klebsiella pneumoniae bacteria strains that were resistant to all available antibiotics that resulted in seven deaths. In addition, there have been numerous reports recently that physicians have resorted to prescribing colistin for Gram-negative bacteria resistant to all other drugs. Colistin was discovered in 1949 and has not been widely used for decades because of serious toxicities, including nephrotoxicity. In our Phase 2 intravenous clinical trial, eravacycline dosed once or twice per day as a monotherapy was effective against multi-drug resistant Klebsiella pneumoniae.
The growing issue of antibiotic-resistant bacterial infections has been widely recognized as an increasingly urgent public health threat, including by the World Health Organization, the CDC, and the Infectious Disease Society of America, or IDSA. In April 2011, IDSA issued a report warning that unless significant measures are taken to increase the pipeline of new antibiotics active against drug-resistant bacteria, people will start to die from common, formerly treatable infections, and medical interventions such as surgery, chemotherapy, organ transplantation and care of premature infants will become increasingly risky. In the pre-antibiotic era before penicillin began to be available in 1942, patients frequently died from what subsequently became easily cured infections. The important need for new treatment options for serious bacterial infections was further highlighted by the passage in July 2012 of the Generating Antibiotic Incentives Now Act, which provides incentives for the development of new antibacterial or antifungal drugs intended to treat serious or life-threatening infections that are resistant to existing treatment. In September 2012, the Food & Drug Administration (FDA) announced the formation of an internal task force to support the development of new antibacterial drugs, which they called "a critical public healthcare goal and a priority for the agency."
In February 2012, Tetraphase announced that the Biomedical Advanced Research and Development Authority (BARDA) had awarded a contract worth up to $67 million for the development of eravacycline, Tetraphase's lead antibiotic candidate in development to treat infections caused by multidrug-resistant Gram-negative pathogens. Tetraphase is collaborating on this contract with Buffalo, NY-based CUBRC, Inc.
CUBRC serves as the prime contractor under the BARDA contract, primarily carrying out a program management and administrative role with additional responsibility for the management of certain preclinical studies. Tetraphase serves as lead technical expert on all aspects of the BARDA contract and serves as a subcontractor responsible for management of chemistry, manufacturing and control activities and clinical studies.
In connection with the BARDA contract, in February 2012, Tetraphase entered into with CUBRC a five-year cost plus-fixed-fee subcontract under which Tetraphase may receive funding of up to approximately $40 million, reflecting the portion of the BARDA funding that may be paid to Tetraphase for its activities.
During the second half of 2011, the National Institutes of Health’s (NIH) National Institute of Allergy and Infectious Diseases (NIAID) awarded a contract worth up to $36 million and a grant valued up to $4.3 million for the development of TP-271, Tetraphase’s novel antibiotic for respiratory disease caused by bacterial biothreats and antibiotic-resistant public health pathogens. Tetraphase is collaborating on these awards as a sub-contractor to Buffalo, NY-based CUBRC, Inc.
The NIAID awards cover development, manufacturing, and clinical activities to position TP-271 for further development against certain biothreat agents, including Francisella tularensis, which causes tularemia, Yersinia pestis, which causes bubonic plague, and Bacillus anthracis, which causes anthrax disease, and bacterial pathogens associated with community-acquired bacterial pneumonia (CABP).
CUBRC serves as the prime contractor under the NIAID awards, primarily carrying out a program management and administrative role, though also with responsibility for the management of certain preclinical studies under the NIAID contract. Tetraphase serves as the lead technical expert on all aspects of the NIAID awards and serves as the subcontractor responsible for management of chemistry, manufacturing and control activities and clinical studies.
In connection with the NIAID contract, in October 2011, Tetraphase entered into with CUBRC a five-year cost-plus-fixed-fee subcontract under which Tetraphase may receive funding of up to approximately $13 million, reflecting the portion of the NIAID contract funding that may be paid to Tetraphase for its activities. In connection with the NIAID grant, in November 2011, CUBRC awarded Tetraphase a 55-month, no-fee subaward of approximately $1 million, reflecting the portion of the NIAID grant funding that may be paid to Tetraphase for its activities.
Our Technology
We believe that our proprietary chemistry technology, licensed from Harvard on an exclusive worldwide basis and enhanced at Tetraphase, represents a significant innovation in the creation of tetracycline drugs and has the potential to reinvigorate the clinical and market potential of the class.
The tetracycline class of antibiotics has been used successfully for more than 50 years. Unlike our tetracycline compounds, all tetracyclines on the market and under development of which we are aware are produced semi-synthetically, first in bacteria and then modified in a limited number of ways by available chemistry. These conventional methods have only been able to produce tetracycline antibiotics with limited chemical diversity, making it difficult for conventional technology to create tetracycline antibiotics that address a wide variety of multi-drug resistant bacteria. In part, because of the challenges in creating novel tetracycline molecules, only one tetracycline antibiotic has been developed and approved by the FDA for sale in the United States in the past 30 years.
By contrast, our proprietary technology makes it possible to create novel tetracycline antibiotics using a practical, fully synthetic process for what we believe is the first time. This fully synthetic process avoids the limitations of bacterially derived tetracyclines and allows us to chemically modify many positions in the tetracycline scaffold, including most of the positions that we believe could not practically be modified by any previous method. Using our proprietary chemistry technology, we can create a wider variety of tetracycline-based compounds than was previously possible, enabling us to pursue novel tetracycline derivatives for the treatment of multi-drug resistant bacteria that are resistant to existing tetracyclines and other classes of antibiotic products.
The diagram below illustrates the tetracycline core scaffold. Scaffold positions marked with dots have been modified to date using conventional chemistry to create either tetracycline drugs that have been marketed or drug candidates of which we are aware that are currently in development. Our fully synthetic process also allows for modification of the positions marked with dots, but with greater opportunity for substitution than is possible using conventional chemistry. The scaffold positions marked with stars in the diagram below indicate useful positions that we have modified through our fully synthetic process that could not practically be modified by conventional chemistry.

While the four positions on the bottom of the scaffold in the diagram above that are not marked with dots or stars can also be modified using our proprietary chemistry technology, these positions are involved in the binding of tetracyclines to the bacterial ribosome and, consequently, changes to these positions greatly reduce antibacterial activity of compounds. As a result, we are not pursuing compounds based on modifications of these positions.
We believe that our approach to tetracycline drug development provides us with strong intellectual property protection. We hold or have licensed rights under patents and patent applications that protect both our synthetic processes for developing tetracyclines and the compositions of matter of the individual compounds themselves. These include patents and patent applications directed towards the composition of matter for key intermediates like the one used in the synthesis of eravacycline and our other product candidates. Unless a new synthetic method is created, we believe that, for the life of our intellectual property, our proprietary chemistry technology will be the only practical way of modifying the positions on the tetracycline core scaffold that have not been previously modified using conventional chemistry.
Our proprietary chemistry technology has allowed us to develop compounds that have been highly active in in vitro studies against tetracycline-resistant bacterial strains, including multi-drug resistant Gram-negative bacteria, and that have novel pharmacokinetic properties. To date, we have used our proprietary chemistry technology to create more than 2,800 new tetracycline derivatives that we believe could not be practically created with conventional methods. Our discovery program is focused on identifying novel compounds that will be effective against the toughest multi-drug resistant Gram-negative bacteria.
History of Tetracyclines
The tetracycline class of antibiotics comprises a distinct family of substituted hydronaphthalene compounds produced by strains of Streptomyces aureofaciens and Streptomyces rimosus. The first member of the group to be discovered was chlorotetracycline (Aureomycin) in the late 1940s by Dr. Benjamin Duggar, a scientist employed by Lederle Laboratories, who derived the substance from a soil-dwelling bacterium named Streptomyces aureofaciens. Two years later, Finlay and coworkers reported the isolation of Terramycin produced by Streptomyces rimosus. Nobel laureate Robert B. Woodward determined the structure of oxytetracycline enabling Pfizer chemists, led by Lloyd H. Conover, to successfully produce tetracycline itself as a synthetic product.
Few new tetracycline antibiotics have been developed and approved in recent years. The most recently approved tetracycline derivative, Tygacil® (tigecycline, Pfizer), was introduced in 2005 to treat infections resistant to other antimicrobials. Prior to this, the last time a tetracycline derivative gained approval from the U.S. Food & Drug Administration was 1971.
To date, chemically modified tetracycline analogs have invariably been prepared by semi-synthesis, a process in which isolated natural products are chemically transformed.
Tetracyclines are proven antibacterial agents and represent one of the most trusted classes of antibiotics. Tetraphase’s use of its synthetic chemistry platform allows its researchers to build polyfunctional tetracycline molecules with previously inaccessible structural variability, going beyond the limitations of current traditional methods to build diverse, potent, and novel compounds.
Stock Information
As of June 30, 2015, Tetraphase had cash and cash equivalents of $242.1 million and 36.4 million shares outstanding. The company expects that its cash and cash equivalents, as well as expected revenue from its U.S. government awards, will be sufficient to fund operations into the first quarter of 2017.
Daily Chart
Weekly Chart
| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |



