 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.





Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
it is undervalued at this point. way undervalued
SELL YOUR SHARES!!!
http://www.courant.com/business/hc-alexion-shakeup-20170524-story.html
THIS COMPANY IS TANKING.. NOT A BUY!
The company went from 43 BILLION evaluation to 23 BILLION in a short time. Why would you buy?
They are laying off in droves, projections of sales are way off base and nothing good in the pipeline.
If you're smart, you'll sell all your shares while you can!
ALXN's Soliris is administered by a 2 hour Intravenous Transfusion at a medical facility vs. Omeros' OMS721 administered by a shot at home
Omeros Corporation (NASDAQ:OMER)
Q4 2016 Earnings Conference Call
March 16, 2017, 16:30 ET
Executives
Mark Metcalf - IR
Greg Demopulos - Chairman & CEO
Mike Jacobsen - Chief Accounting Officer
Analysts
Tyler Van Buren - Cowen & Company
Thomas Yip - FBR and Company
Liana Moussatos - Wedbush Securities
Steve Brozak - WBB Securities
Serge Balenger - Needham & Company
Elemer Piros - Cantor Fitzgerald
Jason Kolbert - Maxim Group
Operator
Welcome to today's conference call for Omeros Corporation. At this time, all participants are in listen-only mode. After the company's remarks, we will conduct a question-and-answer session. Please be advised that this call is being recorded at the company's request and a replay will be available on the company's website for one week from today.
I'll turn over the call to Mark Metcalf from Omeros. Sir, you may begin.
Mark Metcalf
Good afternoon and thank you for joining the call today. I'd like to remind you that some of the statements that will be made on the call today will be forward-looking. These statements are based on management's beliefs and expectations as of today only and are subject to change. All forward-looking statements involve risks and uncertainties that could cause the company's actual results to differ materially. Please refer to the Risk Factor section of the company's annual report on Form 10-K which was filed today with the SEC for a discussion of these risks and uncertainties.
Dr. Greg Demopulos, Chairman and CEO of Omeros will take you through a corporate update and then Mike Jacobsen, our Chief Accounting Officer will provide an overview of our fourth quarter and year-end financial results. We have some time reserved for questions after the financial overview.
Now, I would like to turn the call over to Dr. Greg Demopulos.
Greg Demopulos
Thank you Mark and good afternoon everyone. We appreciate all of you joining us today. 2017 is shaping up to become a breakout year for Omeros. In 2016 we laid the foundation that will make that possible. Much of that groundwork was solidified in the achievements and successes of the fourth quarter of 2016. Since the broad market launch of a Omidria our commercial product for use during cataract and lens replacement surgery and net revenues have consistently delivered double digit quarter over quarter growth and the fourth quarter of 2016 was no exception. Net revenues of Omidria for the quarter were $12.9 million. This represents a 14% increase over the third quarter of 2016 and on a year over year basis a 212% increase over 2015.
This revenue growth was the result of broad based successes including one, an increase in the number of what we call standard of use accounts or those using Omidria in more than 50% of their procedures Two, an increase in the number of new accounts ordering Omidria, three, an increase in the total number of unique accounts purchasing Omidria during the quarter and four, an increase in the number of daily orders.
Total vials sold in the fourth quarter increased at an even greater rate, 22% over the third quarter and 223% year over year. The difference between the gross and net revenue and the greater growth in vials sold as a reflection of increased gross to net the deductions in the fourth quarter. This increase in gross to net was anticipated and primarily driven by the increased utilization of the Omidria share reimbursement assistance services and our volume discount purchase program which we introduced in November.
The volume discount program provides ambulatory surgery centers or ASCs with rebates based on certain minimum purchase levels of a Omidria. Although this program has been in the market for a relatively short time we have seen early success among the growing number of participants with broader utilization in existing accounts as well and as a meaningful increase in new accounts enabling us to provide the benefits of Omidria to even more patients.
Earlier last year we also initiated an inventory on consignment program for a Omidria. This together with our volume discount program has helped to accelerate growth of Omidria sales. Going forward we expect that facilities will increasingly make use of both volume discounts and consignment. While these programs expand our gross to net deductions, the deduction should be more than offset by the increased growth in Omidria sales. As has been one of our objectives, sales of Omidria at hospitals have continued to grow and mirror the split nationally for cataract surgery. Roughly 35% in hospital outpatient departments and 65% in ambulatory surgery centers. We have focused on increasing our penetration in the hospitals because while perhaps slower to adopt new products once they do adopt they tend to remain long term customers. Teaching hospitals or academic centers are particularly important given their ability to influence physician practices locally and regionally.
This effect on regional practice patterns as enhanced through the residency programs at these teaching institutions. Graduating residents also often incorporate the methods, procedures and products that they used during their training. This is especially true of surgical residents including a foul mix surgery residence [ph]. Omidria is currently in use at approximately 20 large academic centers including New York Eye and Ear, the highest volume cataract surgery hospital in the country. Other major academic centers using Omidria include Massachusetts Eye and Ear, Duke University, Wake Forest University, Yale University, Weill Cornell Medical Center, University of California, San Francisco, Indiana University [indiscernible] Medical Center, University of Kentucky, Moran Eye Center at the University of Utah, University of Virginia and University of Minnesota. Support for Omidria also continues to grow among a [indiscernible] surgeons. As an increasing number of cataract thought leaders and physicians accumulate experience with Omidria podium and panel discussions of the product are regular features at cataract surgery conferences. Omidria received positive and prominent exposure at ophthalmology meetings throughout 2016 and this exposure has accelerated into 2017. In November we announced the successful completion of the post marketing Omidria paediatric clinical trial. In the trial Omidria was well tolerated with adverse event rates consistent with those seen in paediatric cataract surgery and in the control group.
We plan to submit a supplemental NDA this year requesting expanded label language to cover patients of any age. We also expect that this submission will result in an additional six months of regulatory exclusivity for Omidria. International sales of Omidria also began in the fourth quarter. Under our agreement with ITROM distribution of Omidria was initiated in the Kingdom of Saudi Arabia. Local regulatory applications are pending approval in the region including in the United Arab Emirates. Approvals are expected throughout this year which should lead to expanded sales across the Middle East. In addition to our partnership in the Middle East we are currently exploring similar arrangements for the sale of Omidria in other international regions. So we continue to grow Omidria revenues in the U.S. and now internationally as well.
We have seen the resistance to adoption of Omidria fade particularly with respect to any lingering questions about clinical efficacy. The data are clear, there is no product that provides the clinical benefits of a Omidria. Reimbursement concerns are also dissipating as payer coverage continues to increase and more and more facilities access our Omidria share reimbursement services. Our volume purchase discount program is driving additional sales in existing accounts and enabling new accounts to begin building and growing their experience with Omidria.
We are seeing growth across both hospitals and ambulatory surgery centers that mirrors the national %age splits for cataract surgery in these two settings.
Omidria became cash flow positive as a program within three quarters of its launch. Our objective now is for Omidria to generate sufficient revenues to fund our pipeline as well and we expect to achieve that. We also are working hard to secure a separate payment for Omidria following expiration of pass through on January 1, 2018. Our efforts on this front are focused on both legislative and administrative solutions and while we alone do not control the outcome we expect that we will be successful because providing Medicare beneficiaries with broad access to innovative drugs used during surgical procedures is the right thing to do. Stated conversely denying Medicare beneficiaries access to innovative drugs is an untenable position.
Let's turn now to our pipeline, because of their importance I'm going to focus on the following assets. Our complement programs, our PDE and addiction programs and our GPCR's. I'll begin with our complement program focused on Mannan-binding lectin-associated serine protease-2 or MASP-2. MASP-2 is the effector enzyme of the lectin pathway of the complement system, a key component of the immune response. OMS721 is our highly potent and selective antibody against MASP-2 and currently is being evaluated in three clinical programs, typical Hemolytic Uremic Syndrome or aHUS, IgA nephropathy and hematopoietic stem cell transplant-associated TMA, thrombotic microangiopathy or stem cell transplant associated TMA. Enrolment opened this year for our OMS721 Phase 3 program in aHUS. As previously reported from our Phase 2 trial we have seen improvements across TMA markers in aHUS patients treated with OMS721 and to-date a good number of patients have been able to discontinue dialysis. Fastrack status for aHUS was granted by FDA. The Phase 3 trial design was discussed with both FDA and DMA and will consist of one study that will be single arm and open label in other words no control arm and we expect that this one study will satisfy both regulatory agencies. The design will be similar to that conducted for Solaris in the same indication. Based on our discussions with both FDA and DMA 40 patients could provide full approval in Europe and approximately the same number of patients would be required for accelerated approval in the U.S. FDA suggested that we consider and we plan to pursue accelerated approval. To-date we have also received orphan drug designation from the FDA for TMA's broadly including aHUS. Additional data on our aHUS program will be presented at the World Congress of Nephrology in late April. We also have an ongoing Phase 2 program in patients with IgA nephropathy and other glomerulopathies. In October we released statistically significant positive data on IgA patients treated with OMS721. OMS721 significantly improved key end points of renal function and patients achieved partial remission with just 12 weeks of dosing. We continue to follow these patients and after dosing was stopped renal function continued to improve and to our knowledge none of these patients have relapsed. Subsequent data in additional IgA nephropathy patients have demonstrated similar benefits.
Given our data and that there is no current treatment for IgA nephropathy we will submit a full application for breakthrough designation and have discussed with FDA both accelerated approval and a significantly shortened timeline to full approval. We also are preparing a submission for EMA's priority medicines or prime designed to accelerate evaluation of drugs that based on early clinical data offer a major therapeutic advantage over existing treatments or benefit patients for whom there is no treatment option at all. Our Phase 3 program and IgA nephropathy is slated to begin later this year. We continue to evaluate data from our Phase 2 glomerulopathy trials and plan to share more study results in the near future.
Our other OMS721 Phase 2 program is evaluating the drug in patients with stem cell transplant associated TMA. Here again last quarter we announced statistically significant positive Phase 2 clinical data OMS721 in these patients. To-date we have treated nine patients with life threatening post-transplant TMA's and seven of those patients improved. The other two patients received only two to three weeks of OMS721 treatment due to reasons unrelated to the drug. They were managed palliative and died. In contrast patients who completed protocol specified treatment with OMS721 showed meaningful improvement in platelet counts and measures of red blood cell destruction specifically lactate dehydrogenase and haptoglobin levels. These data were presented in February at the tandem meeting of the American Society of Blood and Marrow transplantation and the Center for International Blood and Marrow Transplant Research.
OMS721 has received FDA's orphan drug designation for TMA's. As with IgA nephropathy there is no approved treatment for stem cell transplant associated TMA and here again we plan to pursue breakthrough designation and accelerated approval from FDA as well as the EMA's prime designation. Our Phase 3 program stem cell associated TMA like our Phase 3 program for IgA nephropathy is planned to initiate later this year. Our OMS721 compassionate use program continues to provide treatment to patients internationally. These are patients who for whatever reason are not eligible for our clinical trials and do not and who do not have or have exhausted other treatment options. This program has provided OMS721 treatment to patients with a aHUS, stem cell transplant associated TMA and glomerulopathy including patients who have failed or not tolerated treatment with Solaris.
To provide some perspective here is an example of a compassionate use patient, a 15 year old girl with Diamond-Blackfan anemia which is a congenital disorder that almost exclusively affects red blood cells. The patient underwent stem cell transplantation and subsequently developed TMA. She was treated with Solaris, responded but developed pulmonary edema and Solaris treatment was stopped.
Her TMA relapsed and she again was treated with Solaris, this time at a low dose and again developed pulmonary edema. She was requiring platelet transfusions every day together with haemodialysis almost every other day to keep her alive. Her physician requested that we provide OMS721 under compassionate use and of course we did. Within three weeks of beginning OMS721 she came off dialysis. Her platelets recovered and her transfusions were tapered and then discontinued. By Christmas she was at home with her family and she continues to do well.
The girl's recovery while more dramatic because of her young age is consistent with the improvements in TMA markers that we have observed in stem cell TMA patients who have been treated with OMS721 in the clinical trial. The mortality rate for severe TMA is 90% or higher and again we have observed TMA improvement in all patients who completed treatment with OMS721.
Now I'd like to discuss the other half of our complement franchise, our MASP-3 inhibitor OMS906. The Omeros team was the first to identify MASP-3 as the primary activator of the alternative pathway. So from a patent perspective we control the key activators of two of the three pathways in the complement system namely the lectin pathway and the alternative pathway and we now are also developing molecules that inhibit the key activators of the third or the classical pathway. We have reported positive data and well except in animal models of arthritis and paroxysmal nocturnal hemoglobinuria, or PNH. Given the substantial advantages demonstrated over a C-5 inhibitor in these PNH studies we are preliminarily slating PNH as the first clinical indication for OMS906. Currently we are finalizing selection of our lead and backup molecules and are preparing to initiate scale up for clinical trials.
With respect to how we plan to deliver our MASP-2 and MASP-3 inhibitors for OMS721 we have both intravenous and subcutaneous formulations and we plan to commercialize both for different indications. For OMS906 we plan to develop a subcutaneous formulation to add to our IV formulation. In both our OMS721 and OMS906 programs we also are aggressively developing small molecule inhibitors against MASP-2 and MASP-3 respectively.
Let's now turn to our phosphodiesterase 7 or PDE7 inhibitor program for addiction and compulsive disorders. PDE7 is considered one of the most exciting targets for addiction and Omeros through our issued patent position controls the use of any PDE7 inhibitor for the treatment of any form of addiction or any compulsive disorder. With consistently positive pre-clinical results in cocaine, alcohol, nicotine and opioids as well as in binge eating the data show that our PDE7 inhibitors decrease craving as well as both cue and stress induced relapse. Importantly studies demonstrate that PDE7 inhibitors accomplish these effects without depressing the reward system, a problem that seriously hinders the use of currently approved and the addiction agents. We believe that we have elucidated the mechanism for PDE7 inhibitors and addiction and we are finalizing a manuscript for submission to a leading peer reviewed scientific journal outlining this mechanism.
IND enabling studies are underway as this is the selection of the initial indication and we are currently targeting the submission of an IND or CTA in late 2017 for clinical trials to begin in early 2018. The other half of our addiction franchise is OMS405 our PPAR-gamma agonist program. Omeros has broad issued and pending patents covering the use of any PPAR-gamma agonist in the treatment of any form of addiction or compulsive disorder. During the fourth quarter, we announced positive results from a Phase 2 clinical trial evaluating the effects of a PPAR-gamma agonist in patients with cocaine use disorder. This trial demonstrates that the PPAR-gamma agonist reduces craving and improves the integrity of brain white matter in patients with cocaine use disorder.
We also announced positive data from a Phase 2 clinical trial of evaluating the effects of a PPAR-gamma agonist in heroin dependent subjects. The clinical drug trial administered a PPAR-gamma agonist for up to three weeks in heroin users who are maintained on sub-lingual combination of buprenorphine and naloxone. The findings demonstrated a statistically significant reduction both in drug craving and in measures of anxiety.
With respect to our phosphodiesterase 10 or PDE10 inhibitor program we're evaluating the data from Pfizer's clinical trial in Huntington's disease and Takeda's clinical trial in schizophrenia using their respective PDE10 inhibitors. Each of those trials failed to meet its end point. In retrospect, our decision to await these data before launching into one or more large clinical trials in these indications appears to have been a wise one. Despite the recent misses by Pfizer and Takeda we believe that there is a role for PDE10 inhibition in CNS disorders. We are evaluating other potential indications and assessing our options to move forward. Given our successes in the other programs that we have discussed today we currently have prioritized those programs over PDE10.
Let's wrap up the overview of our development progress with a brief update on our GPCR program. We believe that Omeros exclusively controls [indiscernible] or functionally active compounds for 54 of the 81 Class A orphan GPCRs. We are advancing pre-clinical programs on a number of these exciting targets for which Omeros alone has compounds. The indications include triple negative breast cancer, demyelinating diseases such as multiple sclerosis, appetite and eating disorders and osteoporosis and seasonal effective disorder. In the fourth quarter, we also release data around another receptor that we control GPR174. GPR174 appears to play a unique role in the immune system and we believe that Omeros is the only entity with compounds that block GPR174. We have shown that our compounds in human lymphocytes and monocytes boost the immune response by elevating levels of specific cytokines also resulting in reduction of regulatory t-cells or t-regs. Inhibiting GPR174 represents a novel approach to immune therapies for cancer and potentially for treating other immunologic disorders. Compound optimization and animal studies are ongoing and we expect that you will hear more about this program over the coming months.
With that I will turn the call over to Mike who will lead us through our fourth quarter financial results.
Mike Jacobsen
Thanks, Greg. As Greg noted revenue for the fourth quarter was $12.9 million, all of which was from Omidria products sales. This is an increase of $1.6 million over the third quarter. Our net loss for the fourth quarter was $19.6 million or $0.45 per share, this includes a loss on early extinguishment of debt of $5.6 million or $0.13 per share related to the prepayment of our previous loan agreement. During the fourth quarter, noncash expenses were $5.2 million or $0.12 per share.
Now I will address some details regarding the third versus the fourth quarter. Our reported revenue for the quarter increased 14% from the third quarter while vials of a Omidria sold to our distributors increased by 22% over the third quarter. The difference between these two values is primarily the result of increased gross net deductions in the fourth quarter as the overall price that we receive per unit sold was reduced as we had expected due primarily to the November introduction of our volume purchase discount program. This program has had a net positive impact on our unit sales because we gained new customers and saw the volume of purchases increase in existing accounts that participated in the program. In addition for those existing accounts our incremental revenues were greater than the rebates earned.
Costs and operating expenses for the fourth quarter were $24.8 million, an increase of $1.4 million from the third quarter. The increase was primarily related to noncash employee stock options grants made during the fourth quarter for 2015 performance. As I mentioned earlier during the fourth quarter we incurred a $5.6 million loss on early extinguishment debt related to the prepayment of our previous loan agreement.
Turning to the balance sheet in October 2016 we entered into a six year $125 million secured debt facility with CRG. The facility is interest only through December 31, of 2020 and incurs interest at 12.25%, 4% of which we can defer and add to the outstanding principal at our option through March of 2021. This facility is secured by substantially all of our assets. We borrowed the first tranche of $80 million at closing and used most of the proceeds to retire previously existing debt. We also have the ability to borrow an additional $25 million through September 19th of 2017 if we achieved at least $18 million of Omidria product revenue during any consecutive three month period prior to June 30, 2017 or achieve an average market cap of $700 million during any consecutive three months prior to the June 30, 2017.
We can also borrow an additional $20 million through March 21 of 2018 assuming we achieved Omidria product revenue of at least $25 million during any consecutive three month period or an average market cap of $1 billion during any consecutive three month period prior to December 31, 2017. The new CRT facility has substantially lower annual revenue covenants and our previous loan agreement while also providing an alternative means to satisfy the covenants by achieving market cap thresholds. The revenue requirement for 2017 which is defined as total GAAP revenue is $55 million and the market cap at our current borrowing levels is about or approximately $525 million. In addition any revenue short fall that we could possibly incur can be addressed by paying the amount of the shortfall towards the outstanding principal from qualified borrowings or sales of our common stock.
As of December 31, 2016 we had $45.3 million of cash, cash equivalents and short term investments available for general operations. In addition, we had $5 million of restricted cash as required by our loan agreement and then addition $835,000 of restricted cash and investments available to support our building leases and other operating leases.
Now let's take a look ahead, with regards to revenue we expect that our Omidria revenues will continue to grow throughout 2017. With respect to R&D we have stated in prior calls that we will adjust our research and development spending up or down based on a variety of factors including Omidria product revenues, licensing opportunities, clinical results and overall business conditions. We anticipate that during 2017 the majority of our research and development expenses will be related to Phase 3 and Phase 2 clinical programs or OMS721 and the preparation for commercial manufacturing of 721. Selling, general and administrative expenses for 2017 are expected to increase slightly from the fourth quarter of 2016's run rate. This is primarily due to the costs associated with sales and marketing programs and increased legal costs and pursue the patent infringement claims against Par Pharmaceuticals effort to receive FDA approval for a generic version of Omidria. Interest expense associated with the $80 million outstanding under our credit facility will be approximately $3 million per quarter of which approximately $800,000 can be deferred at our option.
With that I would like to turn the call back over to Greg for Q&A.
Greg Demopulos
Thanks Mike. Let's open the call to questions.
Question-and-Answer Session
Operator
[Operator Instructions]. Our first question comes from Tyler Van Buren from Cowen & Company. Your line is now open.
Tyler Van Buren
Congratulations on the disclosure of beginning the enrolment of the Phase 2 trial and aHUS for 721, clearly a very positive update. So just you know and for what is a disease a very severe patients have to imagine that the agency has a lot of confidence in the efficacy of 721 to allow you guys to go ahead and go into a Phase 3 trial so curious maybe to just hear a little bit more about your end of Phase 2 meeting discussions with the FDA and how that went?
Greg Demopulos
We don't discuss specifics about those meetings Tyler and first thank you for your comments, appreciate it. What we have disclosed from that meeting was our discussion around the design and specifically that the design for the Phase 3 trial will be a single study, single arms so open label, no control arm and the design will be very similar to that which was required for Solaris approval for their BLA. So we again remain confident as you pointed out in our drug and we look forward to completing that clinical trial. Really the interesting part of this is as we've been moving forward with aHUS we have had two other programs sort of rapidly accelerating through development and those as you are the IgA nephropathy study as well as the other nephropathies meaning membranous, lupus nephritis and also our stem cell transplant related TMA studies. So we really have a full plate here with OMS721. To-date we have not found a maximally tolerated dose with 721, we're feeling very good about the safety profile of the drug and clearly we're feeling good about the efficacy that we see at least the apparent efficacy that we see with the drug.
Tyler Van Buren
Okay. Can you tell us what the plan dosing regimen is for Phase 3 and also in terms of timelines when we might see the top-line data from the study?
Greg Demopulos
Phase 3 will be, we expect primarily subcutaneous administration. With respect to the timelines on data we've not made those public yet. We'll keep you informed Tyler as we have more information about timelines and additional data from that study.
Tyler Van Buren
Okay, great. And just one final one 721, as you think about the broader Phase 2 patient population and the efficacy data and try to compare that to what we've seen historically with Solaris. What do you think are the most relevant end points to compare and perhaps can you give us any insight into maybe the percent of patients with the complete TMA response or event free status? Curious to maybe hear a little bit more about that and maybe also potential timing on a publication or plans to submit one?
Greg Demopulos
We haven't released the data that you're requesting there from the Phase 2 program I mean certainly we think that our drug will compare well to Solaris, we also are pleased with the potential safety differences between them. As I mentioned in our initial comments that we will have additional data from the aHUS study in late April at the International Meeting that I mentioned.
Tyler Van Buren
Okay, great. And on Omidria with respect to the C-code transition that you referred to at the end of the year and going into 2018 maybe just a little more granularity on the mechanics there and how should we expect the price to potentially change for the product, any insight there would be helpful.
Greg Demopulos
Yes I think with respect to granularity of our efforts you know we don't want to get too specific about what we're doing other than that we are pursuing a dual pronged approach, one is legislatively and the second is administratively. So we're obviously working through congressional avenues, the second working with CMS directly. I think that there is a good amount of support for the concept that drugs use during surgical procedure should not be packaged. So stated conversely again that drugs used during surgical procedures should be separately paid, really just like almost all other drugs. And we expect again that we will be successful in this effort. With respect to pricing following January 1, 2018 I think that it's a bit premature to discuss that. We're doing well with the product now, let's see how we've progress throughout the year and I think that's a discussion that we can have once hopefully we are successful in securing a long term reimbursement for Omidria.
Operator
Our next question comes from Thomas Yip from FBR and Company. Your line is now open.
Thomas Yip
Very happy to see progress in Omidria and also 721 there earlier, [indiscernible] as well. So first a question regarding the Phase 3 trial of 721 and aHUS. So the finalization of the trial designs and specifically in clinicatrials.gov is that contingent on the FDAs decision on the accelerated approval application that you will file?
Greg Demopulos
No, as you know there is no specific accelerated approval application. Accelerated approval is a process and that is pursued through ongoing discussions with FDA and is based upon in good part data that we present to the FDA from the Phase 3 program.
Thomas Yip
Right. So what factors do you think the FDA will look at most importantly in making that decision in a Phase 3 data? Are there other factors that could persuade them to approve accelerated approval?
Greg Demopulos
I think it will depend on the data that we generate, it will depend on classes of patients, groups of patients that we can treat that perhaps Solaris cannot, it may also tie into potential safety differences between the two drugs remember that 721 does not inhibit the [indiscernible] of the classical pathway which is required for antigen anti-body complexing that is your -- remember the classical pathway is your acquired immune response. So I think there are multiple areas, Thomas, I hope that answered your question.
Thomas Yip
Yes I guess the most important thing to see is some preliminary data from Phase 3 and also we expect to hear more about the ongoing Phase 3 trial as well. So I'm going to switch gears and talk about Omidria a little bit, at which revenue level do you expect to begin providing revenue guidance for Omidria?
Greg Demopulos
I'm not sure, it's a good question. We have made the decision at present that we're not going to add and we have not guided. I think at some point as the market stabilizes, as we are able to appropriately and relatively accurately project those revenues we will consider it I think that now though that that is premature.
Operator
Our next question comes from Liana Moussatos from Wedbush Securities. Your line is now open.
Liana Moussatos
For OMS721 you're going to have data presentations in April at the World Congress and in June at Renal Diseases, how are those data sets different from what we've already seen that you probably disclosed, will there be more patients, will all the patient data be presented -- what's going to be different at those two meetings?
There will be data at those meetings and in those presentations that will be from ongoing clinical work.
Liana Moussatos
Okay. So there will be interim preliminary data that we haven’t seen yet or full data from?
Greg Demopulos
Yes.
Operator
Our next question comes from Steve Brozak from WBB Securities. Your line is now open.
Steve Brozak
Let me dive into a couple of quick questions, since lots has asked and answered. On the OMS721 you're going to be conceivably running multiple trials 721 where you could in theory see data that actually comes back that is better in some areas than in others, can you give us any feedback in terms of what you're seeing as far as what the clinicians are giving you on that kind of guidance because obviously you know one of the things that is really important are the specific clinicians that are treating the patients, what do they expect and what's what your feedback on that so far?
Greg Demopulos
Well obviously from the incidence of compassionate use request, I would think that they are seeing the data as positive and helpful to their patients. I think you've raised a good point. We have multiple trials running at one time, Steve and really the question is how do we get OMS721 across the finish line meaning how do we get it commercialized as quickly as possible and that's really our focus here and I think the beauty of what we are seeing now is that we really do have multiple shots on goal within 721.
Steve Brozak
About those multiple goals with IgA and stem cell, can you go into more detail about that because that's something that I think you mentioned but it is critically important.
Greg Demopulos
Yes I can to whatever extent I am allowed to do here but I will tell you that look we're very pleased. Let me take a step back, we're in a Phase 3 program on aHUS, we've met with FDA and EMA, we're feeling comfortable with what we need to do to get that indication approved for OMS721. So let's put right now aHUS aside and talk about what I think you're asking which is the IgA and stem cell transplant programs for 721. I will tell you that we are very excited about the data that we are seeing in both of those indications. I believe that also you had mentioned how are the physicians viewing those data. I think it is fair to say that those physicians who treat these patients are equally excited about the potential for OMS721 in these indications. We have had dialogue with FDA around these programs. We will continue to do so. We will put out additionally more data from these programs. I think and I think I see where you're going with this, I want to make sure I'm answering your question Steve but these programs each of them or both of them could accelerate quite quickly and we are really looking at all three of these programs and we're controlling the dials across all three and again the objective is to get OMS721 into the market as quickly as possible with really any of the three indications and that will continue to build upon itself, that's the objective, that's our focus from what we're seeing today with all of the appropriate caveat we do expect that we will be successful.
Steve Brozak
Right, I will quickly switch and last question. On Omidria, you obviously you iterated all the significant teaching centers that you're in right now. Given the fact that you transition from teaching centers obviously to other hospital forms regionals and as such, can you give us some feedback even if it's anecdotal on what you've seen on how the teaching centers have started to adopt Omidria and what you would expect to happen as far as how it will start to translate and obviously penetrate the healthcare system.
Greg Demopulos
Sure. Let's just take an example of one of those institutions I mentioned New York Eye and Ear, New York Eye and Ear performs more cataract surgery procedures annually than any other hospital in the United States. These types of institutions are usually slower to adopt just because of their size, just because of the layers of bureaucracy, but their physicians and frankly the pharmacist as well when looking at all of our data pushed hard for the ability to bring Omidria into the facility. Utilization within that facility has continued to expand, the number of physicians using it within the facility has continued to increase and the procedures have increased and then you get the satellite effect from other institutions located other facilities located around New York Eye and Ear that look to New York Eye and Ear to see what is New York Eye and Ear doing in-patient care and when they see that Omidria is an important component of that patient care you know that has an effect and I think that we're seeing that not just in New York Eye and Ear but really at all of those institutions that I mentioned. Duke, Wake Forest, Mass Eye and Ear, UCSF, all of those that I mentioned have that satellite effect or that ripple effect that that really does translate to increased utilization regionally not just locally but I think regionally and the importance of that is also the residency programs right, I mean these are young surgeons in training who are likely going to have more difficulty performing surgery than those who are well versed with years of experience in cataract surgery. Certainly these are young doctors who can benefit from Omidria. And also once they use that product in their training program they tend and very frequently tend to adopt those same routines, those same products, those same practices when they move into private practice or when they move into an academic position at some other institution. So it's an effect seeding future use of Omidria and I think we've seen that pretty clearly.
Operator
Our next question comes from Serge Balenger from Needham & Company. Your line is now open.
Serge Balenger
A couple questions first on Omidria, Greg in lieu of the 2017 guidance can you talk maybe about -- if you're seeing some of the same seasonality we saw last year in the early part of '17 and where do you expect growth to come from in Omidria and -- do you expect any impact on pricing given that we should see additional use of the volume discount program.
Greg Demopulos
In response to your first question, yes we see some of the seasonality not to the same extent that we have previously but certainly. I don't think it's any secret that cataract surgery and other surgical procedures are slower in the early part of the year simply because of how insurance rolls over and those deductible period start anew at the beginning of the year which tends to have patients putting off surgery until a good part of that deductible is already eaten through and they don't have to absorb all of that cost in the early part of January but as I said we're seeing not -- the extent of that is less than what we had previously seen.
With respect to where we think the growth is coming from and will come from in the future I think it's going to come from hospitals and ASC's I think it's coming from expanding utilization within our existing accounts and from a wholly new accounts who are starting to use Omidria. Certainly I think that the very early resistance that we had around Omidria that certainly seems to have waned substantially particularly as I mentioned earlier just the clinical pushback that, gee is this really a product necessary? Does it really do what we need it to do? I think that it is very difficult for someone to take an opposing position to the fact that Omidria does do all of that. I think it's very difficult to take that opposing position credibly when you look at the data. The third question that you asked is what about pricing with respect to the discount program. We still have been able to almost wholly maintain our ASP even with these discount programs. We continue to expect to do these programs in a very smart way and we're monitoring it closely you know remember that our price initially was set as a requirement to qualify for pass through, there's a threshold above which the price needs to be to qualify for pass through. But at some point here we're not going to be limited to that threshold but we're still comfortable with how our pricing is progressing .
Serge Balenger
Back to the -- you're to make further entry into the hospital segment, can you talk about the evaluation process that these P&T committees go through usually pretty focused on costs just how they look at Omidria?
Greg Demopulos
Certainly we've been successful. I mean our distribution across hospitals and ASCs now as we've said reflects exactly what the distribution across the U.S. is. Approximately 35% in hospitals, 65% in ASCs, so we've clearly been successful there. You are correct that they do focus on cost. They also do though focus on clinical benefit and I think that we clearly make a very strong case with respect to clinical benefit. Remember too that a number of these hospitals, these large institutions are 340B facilities. So these are facilities that qualifies 340Bs by treating a sufficient percentage or number of indigent patients and by virtue of their being 340B or having 340B status they are then afforded government mandated discounts. So the 340B program also helps in sort of the entrée search to these hospitals and those initial discussions with the P&T committees and then I think it's really the clinical data that ends up carrying the day and closing that arrangement.
Serge Balenger
Okay. And then just regarding potential European partnerships on Omidria, is that still the plan to enter partnership into '17, if I remember correctly that EU marketing authorization have a shelf-life and how will that affect your partnership discussion?
Greg Demopulos
Once again you're spot on and yes we do plan to partner in 2017, but that’s all I will say about that at this point.
Operator
Our next question comes from Elemer Piros from Cantor. Your line is now open.
Elemer Piros
What I would like to ask is when I look at the historical numbers, quarter and quarter there is a very steady, predictable linear growth in Omidria sales. So my question is that do you see at some point in 2017 perhaps and what would precipitate a divergence from this trend and we're hoping for an upgrade for this to become more of an exponential sort of growth.
Greg Demopulos
Yes I understand, yes we would much prefer that to be a kink up than a kink down. And answer to your question about the kink in that curve yes that's clearly one of our major objectives is to put an upward kink in that curve. We do believe that we can do that. We believe that the programs were initiating help to do that. We also believe that at some point there's a threshold of critical mass with respect to users and once we exceed that we also think that that will help bend that curve upward more steeply than that linear growth that you referenced. Surgeons in general and it appears that a mix surgeons perhaps even more so than many others are conservative but they're slow to adopt new products but once they reach that initial threshold then that growth really picks up. I'll use as an example Viscoelastics, if you look at the adoption rate of this Viscoelastics in their early years of availability to a [indiscernible] surgeon, the percentage penetration was really minimal, low single digits and yet now when you look at Viscoelastic devices what you see is that they are mainstay. They're used in effectively in all procedures and I think that this is somewhat reflective of surgery in general but certainly I think of [indiscernible] surgery in particular.
Elemer Piros
And in the 721 trial would you please confirm that in previous patients, previously treated aHUS patients you also used subcutaneous dosing.
Greg Demopulos
I will neither confirm nor deny that at this point.
Elemer Piros
But in the Phase 3 we're doing that subcu?
Greg Demopulos
Yes.
Elemer Piros
And often would they be dosed?
Greg Demopulos
We've not discussed dosing regimen publicly.
Elemer Piros
Okay. And one last question on the nephrology conference that you highlighted, if you could tell us just qualitative maybe somewhat quantitatively how many patients worth of data would we see, would we see a follow up data from the very earliest patients that you treated?
Greg Demopulos
I will answer that question in this way Elemer, we have to-date put out only two patients from the IgA study. I am confident in telling you that at the conference presentation you will see more patients than what we have already put out publicly and you will see additional data on those patients for whom we have already released data. So you will see more data on the existing patients for those who are already out in the public domain and you will see -- I expect new patients and their data as well.
Elemer Piros
And would we have some aHUS patients data as well?
Greg Demopulos
At the renal program?
Elemer Piros
Yes.
Greg Demopulos
That well I need to check with our clinical group, I know that aHUS data is coming up later in April at the World Congress.
Operator
Our next question comes from Jason Kolbert from Maxim Group. Your line is now open.
Jason Kolbert
I'd like to talk a little bit about OMS721 particularly as it relates to TMA's and stem cell transplantation. Can you do me a favor and just help me understand kind of the origins of the TMA and kind of what the treatment paradigm would look like for when 721 is going to be used in those patients so I can get a handle on what the market size might be. Thanks.
Greg Demopulos
Right. There's a lot in that question so I'll try to take it in a stepwise progression, Jason. First of all the mechanism, endothelial damage, we believe is the inciting event and endothelial damage activating the lectin pathway specifically. We do know that endothelial damage activates the lectin pathway, we know that MASP-2 is the effector enzyme of the lectin pathway and therefore inhibiting MASP-2 as does OMS721 should have a positive effect in disorders associated or temporarily downstream related to endothelial damage. The endothelial damage in stem cell transplant patients well you know that very well with the conditioning required and the drugs used, both pre and post stem cell transplants, so clearly endothelial damage is there. With respect to what patients specifically the patients who we have treated with OMS721 are those patients who really have severe thrombotic microangiopathy.
So these are patients who are sick very, very sick and these are patients whose mortality rate I think as I mentioned would be expected to be 90% or greater, those are the patients that we are initially treating. With respect to what patient population would be served potentially by OMS721 were clearly those patients. So those patients who have already undergone -- who have TMA's and have undergone revision or modification in calcine urine inhibitors or other immunotherapies and TMA continues certainly those patients are the ones we're treating now.
So I would expect that would be a population amenable to treatment but then I would start to look upstream meaning again temporarily upstream to those patients potentially and again you're asking me and I'm giving you my thoughts I want to be very clear about that but this is a PMA following a stem cell transplant as you know very well is an extremely severe disorder. So could want to imagine moving temporally upstream to those demonstrating changes in any markers of TMA, sure, potentially I could imagine that I think you could too. So with respect to ultimately the population of patients with TMA following stem cell transplant we would treat I think it's likely broader than those patients who we are currently treating now.
Jason Kolbert
So it's sounds like the market initially becomes not quite ultra-orphan but ultra-orphan and I'm assuming ultra-orphan like pricing but eventually it could broaden out that kind of much significantly larger segment of the market.
Greg Demopulos
Yes especially when you think of what other disorders are associated with TMA's. There probably there are over 20,000 stem cell transplants U.S. alone, but then you start to think about the other disorders associated with stem cell transplant and there I'm talking about graft versus host disease or GVHD or of veno-occlusive disease as well and you start to think about, gee, what are their opportunities as well and I can tell you that certainly we are considering those as potential opportunities.
Operator
Thank you. And that completes the Q&A part of the call. I would like to turn the call back over to Dr. Demopulos for closing comments.
Greg Demopulos
Well thank you very much, that ends our call for today and I would like to thank everyone for taking the time to listen in today as I said earlier 2017 promises to hold a series of important milestones throughout the year and we do expect to provide additional information on a number of the programs that we discussed today and perhaps others as the year progresses. As always to each of you we appreciate your continued interest and support. Have a good day and we look forward to talking with you again soon.
Operator
Ladies and gentleman thank you for your participation in today's call. This does conclude the program. You may all disconnect. Everyone have a great day.
Copyright policy: All transcripts on this site are the copyright of Seeking Alpha.
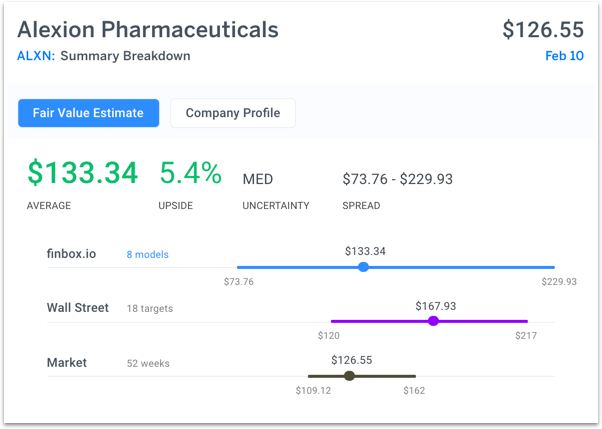
Alexion is scheduled to report earnings on Thursday. The Wall Street consensus price target of $167.93 is above finbox.io's fair value estimate of $133.34. Both estimates imply positive margin of safety:
Six Healthcare Stocks with Nice Upside Potential
$31 BILLION FRAUD WITH $3.5 BILLION DEBT AND A MONSTER PE OF 85 = FANTASTIc Short opp ..Fair Value $40-45 at MAX
$ALXN being shorted to death today......shorties are going to get burned this week.
reloaded calls when it dipped to $111....looking for $115-$120 soon a complete and idiotic overreaction unless something is not being disclosed.
An 11 year veteran CFO from Honeywell would not take the job of there were problems.
Totally oversold. look for this whole loss to be regained by Friday.
HEADS UP! BUYOUT/HOSTILE TAKEOVER!
PPS IS dangerously low. This is territory for a buyout or hostile takeover.
Time to keep an eye on this 1 hit wonder!
Here’s Our Highlight From the Latest Alexion Pharmaceuticals Update
http://marketexclusive.com/heres-highlight-latest-alexion-pharmaceuticals-inc-nasdaqalxn-update/6330/?icd1
Here’s how to get an Exposure to Moderna’s Private Pipeline - article mentions Alexion
http://marketexclusive.com/heres-how-to-get-an-exposure-to-modernas-private-pipeline/1275/
U.S JUSTICE DEPARTMENT INVESTIGATING ALEXION
GOOGLE IT
A look at the charts for you....
Like many biotechs, this one has made giant rally in the last 3+years. but it also shows a topping pattern this year.
To my eyes,it does look like it has topped in the past year and making this pullback now, could be a healthy pullback if the fundamentals are all good. but the chart patterns I'm used to watching with Elliott wave might look at this chart and say we have one more pullback downwave to go in this pattern.

Theres some interesting things to see on this chart. Right now is a key time in the price action as the 50ma and20 ma converge here at 179. this could be a Resistance line that if it doesnt break thru now, could reverse and try to retest the bottom zone, the 200ma is a target there.and shoulder support base around 120 area.
Overhead is a resistance shoulder around the 180-190 area so that resistance zone is right here.
closer view...

Megaphone pattern at the top(higher high and lower low in the recent waves)
Like most biotech stocks and their indexes,its been a Big rally for the past 3+ years. but I think that 200ma is still in play as a pullback target again.

the Fibonacci tools and elliott wave I think they are suggesting a middle zone here around 175 but its also a critical balance point, with the 50ma/20ma as the magnet zone. the Fib retraces have all come to this sensitive point 165-175-185 area that needs to hold for rally momentum to make new upwaves continue. and below this would favor the 200ma as a target. This whole price zone is at a topping shoulder zone in the big picture.
The chart has a few of these bearish aspects,like the shoulder zone is where the Resistance can roll over and go down again.
The key bullish line is around 170 and has Failed several times.
A Range Pattern would have the 200ma and the zone extending to 120 as a Bottom range in play.
This chart will be interesting to watch right now as price bangs up against the Key 20ma/50ma at the sensitive 175 balance area.
Tomorow is all about the financials.
Not sure if their overpaid Synagva will hinder good news. We shall see
KANUMA DRUG TO BE APPROVED
By the end of November, you will see this approved. INCREDIBLE DRUG!
ALEXION LOOKING TO EXPAND
Alexion has quite a bit of money in their billfold and are looking to partner and acquire as we speak.
Although they are Recovering from of the Synageva acquisition, they have their feelers out. They've been riding low on the radar screen for a while now.
Their second drug has been submitted to the FDA pending approval.
Invest people!
CONGRATULATIONS ALEXION!
Drug approval came in just before the close of week!
This drug which is already marketed overseas will cost a patient 1.2M for treatment per year. The most expensive drug in the world!
Their other drug Is set for approval by the end of November. Another blockbuster drug!!
You're going to see some new altime highs shortly!
$ALXN recent news/filings
bearish
## source: finance.yahoo.com
Fri, 08 May 2015 13:21:01 GMT ~ Alexion Pharmaceuticals, Inc. (ALXN) in Focus: Stock Jumps 5.1% - Tale of the Tape
read full: http://finance.yahoo.com/news/alexion-pharmaceuticals-inc-alxn-focus-132101538.html
*********************************************************
Thu, 07 May 2015 20:25:08 GMT ~ Alexion to Buy Synageva for $8.4B: Alexion Down, Synageva Up - Analyst Blog
read full: http://finance.yahoo.com/news/alexion-buy-synageva-8-4b-202508497.html
*********************************************************
Thu, 07 May 2015 20:03:39 GMT ~ Morgan Stanley: Market's Reaction To Linger For Alexion Pharmaceuticals
read full: http://finance.yahoo.com/news/morgan-stanley-markets-reaction-linger-200339280.html
*********************************************************
Thu, 07 May 2015 19:30:13 GMT ~ Here's What Canaccord Learned After Spending A Day With Synageva's Management
read full: http://finance.yahoo.com/news/heres-canaccord-learned-spending-day-193013776.html
*********************************************************
Thu, 07 May 2015 14:59:00 GMT ~ The Lesson From Alexion & Synageva? 'Don't Sleep on M&A'
read full: http://blogs.barrons.com/stockstowatchtoday/2015/05/07/the-lesson-from-alexion-synageva-dont-sleep-on-ma/?mod=yahoobarrons&ru=yahoo
*********************************************************
$ALXN charts
basic chart ## source: stockcharts.com
basic chart ## source: stockscores.com
big daily chart ## source: stockcharts.com
big weekly chart ## source: stockcharts.com
$ALXN company information
## source: otcmarkets.com
Link: http://www.otcmarkets.com/stock/ALXN/company-info
Ticker: $ALXN
OTC Market Place: Not Available
CIK code: 0000899866
Company name: Alexion Pharmaceuticals, Inc.
Incorporated In: DE, USA
Business Description: OTC Markets | Official site of the OTCQX, OTCQB and OTC Pink Marketplaces featuring Free Stock & Bond Quotes, Trade Prices, Chart, Financials and Company News & Information for Investors, Companies and Traders - OTCMarkets.com (window.NREUM||(NREUM={})).loader_config={xpid:"UwMGWVdSGwQIU1RQAgQ="};window.NREUM||(NREUM={}),__nr_require=function(t,e,n){function r(n){if(!e[n]){var o=e[n]={exports:{}};t[n][0].call(o.exports,function(e){var o=t[n][1][e];return r(o?o:e)},o,o.exports)}return e[n].exports}if("function"==typeof __nr_require)return __nr_require;for(var o=0;od;d++)c[d].apply(u,n);return u}function a(t,e){f[t]=s(t).concat(e)}function s(t){return f[t]||[]}function c(){return n(e)}var f={};return{on:a,emit:e,create:c,listeners:s,_events:f}}function r(){return{}}var o="nr@context",i=t("gos");e.exports=n()},{gos:"7eSDFh"}],ee:[function(t,e){e.exports=t("QJf3ax")},{}],3:[function(t){function e(t){try{i.console&&console.log(t)}catch(e){}}var n,r=t("ee"),o=t(1),i={};try{n=localStorage.getItem("__nr_flags").split(","),console&&"function"==typeof console.log&&(i.console=!0,-1!==n.indexOf("dev")&&(i.dev=!0),-1!==n.indexOf("nr_dev")&&(i.nrDev=!0))}catch(a){}i.nrDev&&r.on("internal-error",function(t){e(t.stack)}),i.dev&&r.on("fn-err",function(t,n,r){e(r.stack)}),i.dev&&(e("NR AGENT IN DEVELOPMENT MODE"),e("flags: "+o(i,function(t){return t}).join(", ")))},{1:23,ee:"QJf3ax"}],4:[function(t){function e(t,e,n,i,s){try{c?c-=1:r("err",[s||new UncaughtException(t,e,n)])}catch(f){try{r("ierr",[f,(new Date).getTime(),!0])}catch(u){}}return"function"==typeof a?a.apply(this,o(arguments)):!1}function UncaughtException(t,e,n){this.message=t||"Uncaught error with no additional information",this.sourceURL=e,this.line=n}function n(t){r("err",[t,(new Date).getTime()])}var r=t("handle"),o=t(6),i=t("ee"),a=window.onerror,s=!1,c=0;t("loader").features.err=!0,t(5),window.onerror=e;try{throw new Error}catch(f){"stack"in f&&(t(1),t(2),"addEventListener"in window&&t(3),window.XMLHttpRequest&&XMLHttpRequest.prototype&&XMLHttpRequest.prototype.addEventListener&&window.XMLHttpRequest&&XMLHttpRequest.prototype&&XMLHttpRequest.prototype.addEventListener&&!/CriOS/.test(navigator.userAgent)&&t(4),s=!0)}i.on("fn-start",function(){s&&(c+=1)}),i.on("fn-err",function(t,e,r){s&&(this.thrown=!0,n(r))}),i.on("fn-end",function(){s&&!this.thrown&&c>0&&(c-=1)}),i.on("internal-error",function(t){r("ierr",[t,(new Date).getTime(),!0])})},{1:10,2:9,3:7,4:11,5:3,6:24,ee:"QJf3ax",handle:"D5DuLP",loader:"G9z0Bl"}],5:[function(t){t("loader").features.ins=!0},{loader:"G9z0Bl"}],6:[function(t){function e(){}if(window.performance&&window.performance.timing&&window.performance.getEntriesByType){var n=t("ee"),r=t("handle"),o=t(1),i=t(2);t("loader").features.stn=!0,t(3),n.on("fn-start",function(t){var e=t[0];e instanceof Event&&(this.bstStart=Date.now())}),n.on("fn-end",function(t,e){var n=t[0];n instanceof Event&&r("bst",[n,e,this.bstStart,Date.now()])}),o.on("fn-start",function(t,e,n){this.bstStart=Date.now(),this.bstType=n}),o.on("fn-end",function(t,e){r("bstTimer",[e,this.bstStart,Date.now(),this.bstType])}),i.on("fn-start",function(){this.bstStart=Date.now()}),i.on("fn-end",function(t,e){r("bstTimer",[e,this.bstStart,Date.now(),"requestAnimationFrame"])}),n.on("pushState-start",function(){this.time=Date.now(),this.startPath=location.pathname+location.hash}),n.on("pushState-end",function(){r("bstHist",[location.pathname+location.hash,this.startPath,this.time])}),"addEventListener"in window.performance&&(window.performance.addEventListener("webkitresourcetimingbufferfull",function(){r("bstResource",[window.performance.getEntriesByType("resource")]),window.performance.webkitClearResourceTimings()},!1),window.performance.addEventListener("resourcetimingbufferfull",function(){r("bstResource",[window.performance.getEntriesByType("resource")]),window.performance.clearResourceTimings()},!1)),document.addEventListener("scroll",e,!1),document.addEventListener("keypress",e,!1),document.addEventListener("click",e,!1)}},{1:10,2:9,3:8,ee:"QJf3ax",handle:"D5DuLP",loader:"G9z0Bl"}],7:[function(t,e){function n(t){i.inPlace(t,["addEventListener","removeEventListener"],"-",r)}function r(t){return t[1]}var o=(t(1),t("ee").create()),i=t(2)(o),a=t("gos");if(e.exports=o,n(window),"getPrototypeOf"in Object){for(var s=document;s&&!s.hasOwnProperty("addEventListener");)s=Object.getPrototypeOf(s);s&&n(s);for(var c=XMLHttpRequest.prototype;c&&!c.hasOwnProperty("addEventListener");)c=Object.getPrototypeOf(c);c&&n(c)}else XMLHttpRequest.prototype.hasOwnProperty("addEventListener")&&n(XMLHttpRequest.prototype);o.on("addEventListener-start",function(t){if(t[1]){var e=t[1];"function"==typeof e?this.wrapped=t[1]=a(e,"nr@wrapped",function(){return i(e,"fn-",null,e.name||"anonymous")}):"function"==typeof e.handleEvent&&i.inPlace(e,["handleEvent"],"fn-")}}),o.on("removeEventListener-start",function(t){var e=this.wrapped;e&&(t[1]=e)})},{1:24,2:25,ee:"QJf3ax",gos:"7eSDFh"}],8:[function(t,e){var n=(t(2),t("ee").create()),r=t(1)(n);e.exports=n,r.inPlace(window.history,["pushState"],"-")},{1:25,2:24,ee:"QJf3ax"}],9:[function(t,e){var n=(t(2),t("ee").create()),r=t(1)(n);e.exports=n,r.inPlace(window,["requestAnimationFrame","mozRequestAnimationFrame","webkitRequestAnimationFrame","msRequestAnimationFrame"],"raf-"),n.on("raf-start",function(t){t[0]=r(t[0],"fn-")})},{1:25,2:24,ee:"QJf3ax"}],10:[function(t,e){function n(t,e,n){t[0]=o(t[0],"fn-",null,n)}var r=(t(2),t("ee").create()),o=t(1)(r);e.exports=r,o.inPlace(window,["setTimeout","setInterval","setImmediate"],"setTimer-"),r.on("setTimer-start",n)},{1:25,2:24,ee:"QJf3ax"}],11:[function(t,e){function n(){f.inPlace(this,p,"fn-")}function r(t,e){f.inPlace(e,["onreadystatechange"],"fn-")}function o(t,e){return e}function i(t,e){for(var n in t)e[n]=t[n];return e}var a=t("ee").create(),s=t(1),c=t(2),f=c(a),u=c(s),d=window.XMLHttpRequest,p=["onload","onerror","onabort","onloadstart","onloadend","onprogress","ontimeout"];e.exports=a,window.XMLHttpRequest=function(t){var e=new d(t);try{a.emit("new-xhr",[],e),u.inPlace(e,["addEventListener","removeEventListener"],"-",o),e.addEventListener("readystatechange",n,!1)}catch(r){try{a.emit("internal-error",[r])}catch(i){}}return e},i(d,XMLHttpRequest),XMLHttpRequest.prototype=d.prototype,f.inPlace(XMLHttpRequest.prototype,["open","send"],"-xhr-",o),a.on("send-xhr-start",r),a.on("open-xhr-start",r)},{1:7,2:25,ee:"QJf3ax"}],12:[function(t){function e(t){var e=this.params,r=this.metrics;if(!this.ended){this.ended=!0;for(var i=0;c>i;i++)t.removeEventListener(s,this.listener,!1);if(!e.aborted){if(r.duration=(new Date).getTime()-this.startTime,4===t.readyState){e.status=t.status;var a=t.responseType,f="arraybuffer"===a||"blob"===a||"json"===a?t.response:t.responseText,u=n(f);if(u&&(r.rxSize=u),this.sameOrigin){var d=t.getResponseHeader("X-NewRelic-App-Data");d&&(e.cat=d.split(", ").pop())}}else e.status=0;r.cbTime=this.cbTime,o("xhr",[e,r,this.startTime])}}}function n(t){if("string"==typeof t&&t.length)return t.length;if("object"!=typeof t)return void 0;if("undefined"!=typeof ArrayBuffer&&t instanceof ArrayBuffer&&t.byteLength)return t.byteLength;if("undefined"!=typeof Blob&&t instanceof Blob&&t.size)return t.size;if("undefined"!=typeof FormData&&t instanceof FormData)return void 0;try{return JSON.stringify(t).length}catch(e){return void 0}}function r(t,e){var n=i(e),r=t.params;r.host=n.hostname+":"+n.port,r.pathname=n.pathname,t.sameOrigin=n.sameOrigin}if(window.XMLHttpRequest&&XMLHttpRequest.prototype&&XMLHttpRequest.prototype.addEventListener&&!/CriOS/.test(navigator.userAgent)){t("loader").features.xhr=!0;var o=t("handle"),i=t(2),a=t("ee"),s=["load","error","abort","timeout"],c=s.length,f=t(1);t(4),t(3),a.on("new-xhr",function(){this.totalCbs=0,this.called=0,this.cbTime=0,this.end=e,this.ended=!1,this.xhrGuids={}}),a.on("open-xhr-start",function(t){this.params={method:t[0]},r(this,t[1]),this.metrics={}}),a.on("open-xhr-end",function(t,e){"loader_config"in NREUM&&"xpid"in NREUM.loader_config&&this.sameOrigin&&e.setRequestHeader("X-NewRelic-ID",NREUM.loader_config.xpid)}),a.on("send-xhr-start",function(t,e){var r=this.metrics,o=t[0],i=this;if(r&&o){var f=n(o);f&&(r.txSize=f)}this.startTime=(new Date).getTime(),this.listener=function(t){try{"abort"===t.type&&(i.params.aborted=!0),("load"!==t.type||i.called===i.totalCbs&&(i.onloadCalled||"function"!=typeof e.onload))&&i.end(e)}catch(n){try{a.emit("internal-error",[n])}catch(r){}}};for(var u=0;c>u;u++)e.addEventListener(s,this.listener,!1)}),a.on("xhr-cb-time",function(t,e,n){this.cbTime+=t,e?this.onloadCalled=!0:this.called+=1,this.called!==this.totalCbs||!this.onloadCalled&&"function"==typeof n.onload||this.end(n)}),a.on("xhr-load-added",function(t,e){var n=""+f(t)+!!e;this.xhrGuids&&!this.xhrGuids[n]&&(this.xhrGuids[n]=!0,this.totalCbs+=1)}),a.on("xhr-load-removed",function(t,e){var n=""+f(t)+!!e;this.xhrGuids&&this.xhrGuids[n]&&(delete this.xhrGuids[n],this.totalCbs-=1)}),a.on("addEventListener-end",function(t,e){e instanceof XMLHttpRequest&&"load"===t[0]&&a.emit("xhr-load-added",[t[1],t[2]],e)}),a.on("removeEventListener-end",function(t,e){e instanceof XMLHttpRequest&&"load"===t[0]&&a.emit("xhr-load-removed",[t[1],t[2]],e)}),a.on("fn-start",function(t,e,n){e instanceof XMLHttpRequest&&("onload"===n&&(this.onload=!0),("load"===(t[0]&&t[0].type)||this.onload)&&(this.xhrCbStart=(new Date).getTime()))}),a.on("fn-end",function(t,e){this.xhrCbStart&&a.emit("xhr-cb-time",[(new Date).getTime()-this.xhrCbStart,this.onload,e],e)})}},{1:"XL7HBI",2:13,3:11,4:7,ee:"QJf3ax",handle:"D5DuLP",loader:"G9z0Bl"}],13:[function(t,e){e.exports=function(t){var e=document.createElement("a"),n=window.location,r={};e.href=t,r.port=e.port;var o=e.href.split("://");return!r.port&&o[1]&&(r.port=o[1].split("/")[0].split("@").pop().split(":")[1]),r.port&&"0"!==r.port||(r.port="https"===o[0]?"443":"80"),r.hostname=e.hostname||n.hostname,r.pathname=e.pathname,r.protocol=o[0],"/"!==r.pathname.charAt(0)&&(r.pathname="/"+r.pathname),r.sameOrigin=!e.hostname||e.hostname===document.domain&&e.port===n.port&&e.protocol===n.protocol,r}},{}],14:[function(t,e){function n(t){return function(){r(t,[(new Date).getTime()].concat(i(arguments)))}}var r=t("handle"),o=t(1),i=t(2);"undefined"==typeof window.newrelic&&(newrelic=window.NREUM);var a=["setPageViewName","addPageAction","setCustomAttribute","finished","addToTrace","inlineHit","noticeError"];o(a,function(t,e){window.NREUM[e]=n("api-"+e)}),e.exports=window.NREUM},{1:23,2:24,handle:"D5DuLP"}],"7eSDFh":[function(t,e){function n(t,e,n){if(r.call(t,e))return t[e];var o=n();if(Object.defineProperty&&Object.keys)try{return Object.defineProperty(t,e,{value:o,writable:!0,enumerable:!1}),o}catch(i){}return t[e]=o,o}var r=Object.prototype.hasOwnProperty;e.exports=n},{}],gos:[function(t,e){e.exports=t("7eSDFh")},{}],handle:[function(t,e){e.exports=t("D5DuLP")},{}],D5DuLP:[function(t,e){function n(t,e,n){return r.listeners(t).length?r.emit(t,e,n):(o[t]||(o[t]=[]),void o[t].push(e))}var r=t("ee").create(),o={};e.exports=n,n.ee=r,r.q=o},{ee:"QJf3ax"}],id:[function(t,e){e.exports=t("XL7HBI")},{}],XL7HBI:[function(t,e){function n(t){var e=typeof t;return!t||"object"!==e&&"function"!==e?-1:t===window?0:i(t,o,function(){return r++})}var r=1,o="nr@id",i=t("gos");e.exports=n},{gos:"7eSDFh"}],G9z0Bl:[function(t,e){function n(){var t=p.info=NREUM.info,e=f.getElementsByTagName("script")[0];if(t&&t.licenseKey&&t.applicationID&&e){s(d,function(e,n){e in t||(t[e]=n)});var n="https"===u.split(":")[0]||t.sslForHttp;p.proto=n?"https://":"http://",a("mark",["onload",i()]);var r=f.createElement("script");r.src=p.proto+t.agent,e.parentNode.insertBefore(r,e)}}function r(){"complete"===f.readyState&&o()}function o(){a("mark",["domContent",i()])}function i(){return(new Date).getTime()}var a=t("handle"),s=t(1),c=(t(2),window),f=c.document,u=(""+location).split("?")[0],d={beacon:"bam.nr-data.net",errorBeacon:"bam.nr-data.net",agent:"js-agent.newrelic.com/nr-632.min.js"},p=e.exports={offset:i(),origin:u,features:{}};f.addEventListener?(f.addEventListener("DOMContentLoaded",o,!1),c.addEventListener("load",n,!1)):(f.attachEvent("onreadystatechange",r),c.attachEvent("onload",n)),a("mark",["firstbyte",i()])},{1:23,2:14,handle:"D5DuLP"}],loader:[function(t,e){e.exports=t("G9z0Bl")},{}],23:[function(t,e){function n(t,e){var n=[],o="",i=0;for(o in t)r.call(t,o)&&(n=e(o,t[o]),i+=1);return n}var r=Object.prototype.hasOwnProperty;e.exports=n},{}],24:[function(t,e){function n(t,e,n){e||(e=0),"undefined"==typeof n&&(n=t?t.length:0);for(var r=-1,o=n-e||0,i=Array(0>o?0:o);++r
$ALXN share structure
## source: otcmarkets.com
Market Value: $32,523,030,276 a/o May 07, 2015
Shares Outstanding: 199,576,769 a/o Apr 21, 2015
Float: Not Available
Authorized Shares: Not Available
Par Value: 0.0001
$ALXN extra dd links
Company name: Alexion Pharmaceuticals, Inc.
## STOCK DETAILS ##
After Hours Quote (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/after-hours
Option Chain (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/option-chain
Historical Prices (yahoo.com): http://finance.yahoo.com/q/hp?s=ALXN+Historical+Prices
Company Profile (yahoo.com): http://finance.yahoo.com/q/pr?s=ALXN+Profile
Industry (yahoo.com): http://finance.yahoo.com/q/in?s=ALXN+Industry
## COMPANY NEWS ##
Market Stream (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/stream
Latest news (otcmarkets.com): http://www.otcmarkets.com/stock/ALXN/news - http://finance.yahoo.com/q/h?s=ALXN+Headlines
## STOCK ANALYSIS ##
Analyst Research (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/analyst-research
Guru Analysis (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/guru-analysis
Stock Report (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/stock-report
Competitors (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/competitors
Stock Consultant (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/stock-consultant
Stock Comparison (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/stock-comparison
Investopedia (investopedia.com): http://www.investopedia.com/markets/stocks/ALXN/?wa=0
Research Reports (otcmarkets.com): http://www.otcmarkets.com/stock/ALXN/research
Basic Tech. Analysis (yahoo.com): http://finance.yahoo.com/q/ta?s=ALXN+Basic+Tech.+Analysis
Barchart (barchart.com): http://www.barchart.com/quotes/stocks/ALXN
DTCC (dtcc.com): http://search2.dtcc.com/?q=Alexion+Pharmaceuticals%2C+Inc.&x=10&y=8&sp_p=all&sp_f=ISO-8859-1
Spoke company information (spoke.com): http://www.spoke.com/search?utf8=%E2%9C%93&q=Alexion+Pharmaceuticals%2C+Inc.
Corporation WIKI (corporationwiki.com): http://www.corporationwiki.com/search/results?term=Alexion+Pharmaceuticals%2C+Inc.&x=0&y=0
## FUNDAMENTALS ##
Call Transcripts (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/call-transcripts
Annual Report (companyspotlight.com): http://www.companyspotlight.com/library/companies/keyword/ALXN
Income Statement (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/financials?query=income-statement
Revenue/EPS (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/revenue-eps
SEC Filings (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/sec-filings
Edgar filings (sec.gov): http://www.sec.gov/cgi-bin/browse-edgar?action=getcompany&CIK=0000899866&owner=exclude&count=40
Latest filings (otcmarkets.com): http://www.otcmarkets.com/stock/ALXN/filings
Latest financials (otcmarkets.com): http://www.otcmarkets.com/stock/ALXN/financials
Short Interest (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/short-interest
Dividend History (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/dividend-history
RegSho (regsho.com): http://www.regsho.com/tools/symbol_stats.php?sym=ALXN&search=search
OTC Short Report (otcshortreport.com): http://otcshortreport.com/index.php?index=ALXN
Short Sales (otcmarkets.com): http://www.otcmarkets.com/stock/ALXN/short-sales
Key Statistics (yahoo.com): http://finance.yahoo.com/q/ks?s=ALXN+Key+Statistics
Insider Roster (yahoo.com): http://finance.yahoo.com/q/ir?s=ALXN+Insider+Roster
Income Statement (yahoo.com): http://finance.yahoo.com/q/is?s=ALXN
Balance Sheet (yahoo.com): http://finance.yahoo.com/q/bs?s=ALXN
Cash Flow (yahoo.com): http://finance.yahoo.com/q/cf?s=ALXN+Cash+Flow&annual
## HOLDINGS ##
Major holdings (cnbc.com): http://data.cnbc.com/quotes/ALXN/tab/8.1
Insider transactions (yahoo.com): http://finance.yahoo.com/q/it?s=ALXN+Insider+Transactions
Insider transactions (secform4.com): http://www.secform4.com/insider-trading/ALXN.htm
Insider transactions (insidercrow.com): http://www.insidercow.com/history/company.jsp?company=ALXN
Ownership Summary (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/ownership-summary
Institutional Holdings (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/institutional-holdings
Insiders (SEC Form 4) (nasdaq.com): http://www.nasdaq.com/symbol/ALXN/insider-trades
Insider Disclosure (otcmarkets.com): http://www.otcmarkets.com/stock/ALXN/insider-transactions
## SOCIAL MEDIA AND OTHER VARIOUS SOURCES ##
PST (pennystocktweets.com): http://www.pennystocktweets.com/stocks/profile/ALXN
Market Watch (marketwatch.com): http://www.marketwatch.com/investing/stock/ALXN
Bloomberg (bloomberg.com): http://www.bloomberg.com/quote/ALXN:US
Morningstar (morningstar.com): http://quotes.morningstar.com/stock/s?t=ALXN
Bussinessweek (businessweek.com): http://investing.businessweek.com/research/stocks/snapshot/snapshot_article.asp?ticker=ALXN
$ALXN DD Notes ~ http://www.ddnotesmaker.com/ALXN
I still believe they'll do well in the next months from here. Building a small position
Major beat down today! Overpaid for GEVA.
Hell of a chart here! 90% success when trading long from May to September
Closed above 190. > ALL TIME HIGH!
I'm curious to see what they are doing with the Moderna spinoff.
http://modernatx.com/
ALXN Weekly Chart: the 3rd week of Oct. ALXN closed above resistance,...,...w/ Sat.'s huge news ALXN is set up for a breakout.....MA's(50 & 100) have been providing solid support on pullbacks.......AXLN is currently riding in the Very Bullish Upper Bollinger Band channel between Upper BB resistance & MA's(7 & 10) support.......
AXLN on close above 125 for the week & Breakout radar..........$$$
Soliris® (eculizumab) Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (aHUS)
2013-11-09 21:23 ET - News Release
- New Data from theLargest Prospective Trial of Adult Patients with aHUS and First Prospective Trial in Pediatric Patients with aHUS Confirm the Safety and Efficacy Profile of Soliris --
- ASN Meeting Also Features Three-year Update Data Highlighting Long-term Benefits of Chronic Soliris Therapy in Patients with aHUS -
CHESHIRE, CT, Nov. 9, 2013 /CNW/ - Alexion Pharmaceuticals, Inc. (Nasdaq: ALXN) today announced that researchers presented data from four clinical trials, all demonstrating the clinical benefits of Soliris® (eculizumab) for the treatment of atypical hemolytic uremic syndrome (aHUS), a genetic, chronic, ultra-rare disease associated with vital organ failure and premature death. Soliris is the first and only approved safe and effective treatment for pediatric and adult patients with aHUS. In two large, prospective, multinational studies, Soliris inhibited systemic complement-mediated thrombotic microangiopathy (TMA, the formation of blood clots in small blood vessels throughout the body) and improved renal function in both pediatric and adult patients with aHUS.1,2 The data were presented at Kidney Week 2013, the annual meeting of the American Society of Nephrology (ASN) in Atlanta.
The ASN meeting also featured the presentation of three-year update data from two pivotal Phase 2 extension studies that highlighted the long-term benefits of Soliris therapy in patients with aHUS. In these studies, ongoing Soliris treatment at the three-year update was associated with sustained inhibition of complement-mediated TMA, as indicated by stabilization or continued improvement in key hematologic and renal endpoints, and quality of life.3,4 Additionally, investigators presented initial characteristics from patients enrolled in a global aHUS Registry, which is prospectively collecting information to enhance understanding of the disease process in order to help optimize care and improve quality of life for patients with aHUS.5
aHUS is an ultra-rare, life-threatening, chronic genetic disease that can progressively damage vital organs, leading to stroke, heart attack, kidney failure, and death.6 The morbidities and premature mortality in aHUS are caused by chronic, uncontrolled activation of the complement system, resulting in systemic TMA.7,8 Soliris, a first-in-class terminal complement inhibitor, specifically targets uncontrolled complement activation, and is the first and only approved treatment for patients with aHUS in the United States, European Union, Japan and other countries.
"Results from four prospective studies demonstrate a significant and sustained inhibition of complement-mediated TMA with Soliris treatment and support the chronic use of Soliris in pediatric and adult patients with aHUS," said Leonard Bell, Chief Executive Officer of Alexion. "These studies further underscore the rationale for initiating Soliris therapy at the time of clinical diagnosis of aHUS and chronic treatment of patients to achieve optimal outcomes."
Soliris in Pediatric Patients with aHUS (Abstract SA-PO0849)
In a poster presentation today, researchers presented positive results from the first prospective trial of Soliris in pediatric patients with aHUS, which follows the previously presented positive results of a retrospective study in pediatric patients with aHUS.9 This open-label, prospective, single-arm, multinational trial enrolled a heterogeneous population of patients who were >1 month old and <18 years of age. It included 22 pediatric patients with aHUS, of whom 16 (73%) were newly diagnosed. Prior PE/PI was not required for inclusion in the study. Most patients enrolled in the study (12/22, 55%) received Soliris as their first aHUS specific treatment and had not received plasma exchange or infusion (PE/PI) therapy prior to Soliris therapy. Two patients (9%) had received a prior kidney transplant. The primary endpoint of the study was the proportion of patients with a complete TMA response, defined as platelet count normalization, lactate dehydrogenase (LDH) normalization, and >25% improvement in serum creatinine from baseline, during 26 weeks of treatment.1
In the study, the median time from current manifestation of aHUS to first dose of Soliris was six days. Nineteen patients (86%) completed the initial 26 weeks of Soliris therapy, and 14 of 22 patients (64%) achieved the study's primary endpoint of complete TMA response at 26 weeks, which required significant improvement in renal function (>25% decrease in creatinine). Platelet count normalization was achieved in 21 of the 22 patients (95%); the median time to platelet count normalization was seven days and the mean improvement in platelet count from baseline was 164 x109/L (p<0.0001). Hematologic normalization was observed in 18 of 22 patients (82%). Of the 10 patients on PE/PI at baseline, all (100%) discontinued by the end of the 26-week study.1
In terms of renal parameters, the mean estimated glomerular filtration rate (eGFR) increase from baseline was 64 mL/min/1.73m2 (P<0.001) and 19 patients (86%) achieved an improvement in eGFR from baseline of at least 15 mL/min/1.73m2 after 26 weeks. By Week 26, 16 patients (73%) had experienced at least a 25% decrease from baseline in serum creatinine. Importantly, 9 of 11 patients (82%) who were on dialysis at baseline discontinued dialysis for the duration of the study and all 12 patients who were not on dialysis at baseline continued dialysis-free through 26 weeks.1
"This was the first prospective study of pediatric patients with aHUS, and demonstrated that chronic Soliris treatment led to rapid and sustained improvement in platelet counts and significant improvement in kidney function, including discontinuation of dialysis," said Larry Greenbaum, M.D., Ph.D., Director of Pediatric Nephrology at Emory University and Children's Healthcare of Atlanta.10 "The safety and efficacy demonstrated in this prospective trial confirm the results observed in the previous retrospective pediatric study as well as the published Phase 2 prospective adult trials, and support the recommendation of Soliris as a first-line treatment in children with aHUS."
Soliris was generally well tolerated in the study. The most common adverse events (AEs) were fever (50%) and cough (36%). One patient had a human anti-human antibody response, and continued chronic Soliris treatment without apparent adverse effect. There were no meningococcal infections and no deaths during the 26-week study.1
Soliris in Adult Patients with aHUS (Abstract FR-OR057)
In an oral presentation on November 8, researchers presented positive new data from the largest prospective trial of Soliris in adult patients with aHUS. This open-label, single-arm, multinational trial enrolled 41 adult patients with aHUS representing a broad patient population. Prior PE/PI was not required for inclusion in the study, and the median time from aHUS manifestation to first dose of Soliris was approximately 2 weeks. Thirty of 41 patients (73%) in the study were newly diagnosed, six patients (15%) had no PE/PI during the current clinical manifestation, 24 patients (59%) were on dialysis at baseline, nine patients (22%) had a prior kidney transplant, and 20 patients (49%) had an identified complement factor mutation. All endpoints were evaluated at 26 weeks of treatment in an intent-to-treat analysis, and 38 (93%) of enrolled patients completed the 26-week study period. The primary endpoint of the study was the proportion of patients with complete TMA response, as measured by platelet count normalization, LDH normalization and preservation of renal function (<25% increase in serum creatinine from baseline), at 26 weeks.2
The study met its primary endpoint, with 30 of 41 patients (73%) achieving a complete TMA response at 26 weeks. Forty of 41 patients (98%) achieved platelet count normalization (=150 x109/L) by week 26, and the mean increase in platelet count from baseline was 135x109/L (P<0.0001), demonstrating inhibition of TMA.2
Soliris significantly improved renal function with a mean increase in eGFR from baseline of 29 mL/min/1.73m2 (P<0.0001). Most importantly, of the 24 patients who were on dialysis at baseline, 20 patients (83%) discontinued dialysis by week 26.2
"This is the largest study in aHUS and the results confirm those from previous prospective trials, in which ongoing Soliris treatment led to sustained inhibition of complement-mediated TMA, rapid and sustained improvements in hematological parameters, and continued, on-going improvement in renal function in adult patients with aHUS,"said Fadi Fakhouri, M.D., Ph.D., Centre Hospitalier Universitaire de Nantes, Nantes, France.11 "Results from this study also support the recent guidelines recommending immediate treatment with Soliris in adults with aHUS once an unequivocal diagnosis has been made."
Soliris was generally well tolerated in the study. The most common AEs were headache (37%), diarrhea (32%) and peripheral edema (22%). There were two cases of meningococcal infections; both patients recovered, with one patient continuing on Soliris therapy and one discontinuing therapy with subsequent deterioration of renal function that necessitated dialysis support. There were no deaths in the study.2
Soliris in aHUS Patients with a Long Duration of Disease and Chronic Kidney Damage (Previously Receiving Prolonged PE/PI): Three-year Update (Abstract SA-PO850)
In a poster presentation today, researchers presented findings from a three-year update of a prospective, open-label, single-arm Phase 2 trial of Soliris in 20 adult and adolescent patients with a long duration of aHUS and chronic kidney disease (CKD) who were undergoing prolonged PE/PI before starting treatment with Soliris. Patients had been diagnosed with aHUS a median of 48 months prior to starting the study. Twenty patients were enrolled in the initial study and received Soliris for 26 weeks. Nineteen of the 20 patients continued into a long-term extension phase; 16 patients were treated for 30 months or more and 10 patients remained enrolled in the trial at 3 years. Patients were evaluated for a median duration of 156 weeks. The co-primary endpoints were TMA event-free status and hematologic normalization.3
According to investigators, in aHUS patients with long disease duration and CKD, long-term treatment with Soliris led to improvements in hematologic and renal function over 3 years. Treatment with Soliris resulted in achievement of TMA event-free status (at least 12 consecutive weeks of stable platelet count, no PE/PI, and no new dialysis) and hematologic normalization in most patients by 3 years. By the 3-year update, 19 of 20 patients (95%) had achieved TMA event-free status and 18 of 20 (90%) had achieved hematologic normalization. Significant improvements in eGFR were observed by week 4 (P<0.01). Additionally, Soliris treatment maintained long-term improvement in patients' quality of life, as measured by the EuroQoL5D (EQ-5D) scale, at 3 years (P=0.0001). Soliris therapy was safe and there were no meningococcal infections in patients over 3 years of treatment.3
"These data indicate that significant and time-dependent improvement in kidney function can be obtained with long-term eculizumab therapy, even in aHUS patients with a history of chronic kidney damage," stated Yahsou Delmas, M.D., Ph.D., at Nephrology Unit, Clearing University Hospital, Bordeaux in Bordeaux, France.12
Soliris in aHUS Patients with Progressing TMA Despite Intensive PE/PI: Three-year Update (Abstract SA-PO852)
In another poster presented today, researchers presented results from a three-year update of a prospective, open-label, single-arm Phase 2 study in 17 adult and adolescent patients with aHUS who had presented with active, progressing TMA. Seventeen patients were enrolled in the initial study and received Soliris for 26 weeks. Thirteen of the 17 patients continued into a long-term extension phase.4
In patients with aHUS and clinical evidence of progressing TMA, investigators reported that long-term Soliris treatment inhibited complement-mediated TMA, as measured by rapid and sustained improvement in platelet count over three years (mean change from baseline, P=0.0001 at 26 weeks and P<0.0001 at 3 years), as well as early achievement of hematologic normalization and TMA event-free status (at least 12 consecutive weeks of stable platelet count, no PE/PI, and no new dialysis). Additionally, long-term Soliris treatment was associated with a rapid and sustained improvement in mean change of eGFR over 3 years (mean change from baseline, 32 ml/min/1.73m2, P=0.001 at 26 weeks and 38 ml/min/1.73m2, P<0.0001 at the three-year update).4
"The three-year safety and efficacy update data from this study highlight the durability of Soliris and support the benefit of continued therapy in patients with aHUS," concluded A. Osama Gaber, Professor of Surgery at Weill Cornell Medical College and Director of the Methodist J.C. Walter Transplant Center at The Methodist Hospital in Houston, Texas.13 "The data also support that continued treatment with Soliris maintains beneficial long-term patient outcomes in patients at risk from life-threatening complications of TMA."
Initial Patient Characteristics from Global aHUS Registry (Abstract SA-PO853)
Also on November 9, Christoph Licht, M.D., FASN, Associate Professor of Paediatrics, Division of Nephrology at The Hospital for Sick Children, University of Toronto, presented baseline demographics from the initial patients enrolled in the global aHUS Registry, which was established in April 2012 to prospectively collect information on patients with aHUS. As of September 2013, a total of 211 patients had enrolled in the global aHUS patient registry. The results and analyses collected within the Registry will increase awareness and understanding of aHUS disease history and progression in order to help optimize care and improve quality of life for patients with aHUS.5
About aHUS
aHUS is a chronic, ultra-rare, and life-threatening disease in which a genetic deficiency in one or more complement regulatory genes causes chronic uncontrolled complement activation, resulting in complement-mediated thrombotic microangiopathy (TMA), the formation of blood clots in small blood vessels throughout the body.14,15 Permanent, uncontrolled complement activation in aHUS causes a life-long risk for TMA, which leads to sudden, catastrophic, and life-threatening damage to the kidney, brain, heart, and other vital organs, and premature death.14,16 Sixty-five percent of all patients with aHUS die, require kidney dialysis, or have permanent kidney damage within the first year after diagnosis despite plasma exchange or plasma infusion (PE/PI).8,17 The majority of patients with aHUS who receive a kidney transplant commonly experience subsequent systemic TMA, resulting in a 90% transplant failure rate in these TMA patients.18
aHUS affects both children and adults. Complement-mediated TMA also causes reduction in platelet count (thrombocytopenia) and red blood cell destruction (hemolysis). While mutations have been identified in at least ten different complement regulatory genes, mutations are not identified in 30-50% of patients with a confirmed diagnosis of aHUS.7
About Soliris
Soliris is a first-in-class terminal complement inhibitor developed from the laboratory through regulatory approval and commercialization by Alexion. Soliris is approved in the US (2007), European Union (2007), Japan (2010) and other countries as the first and only treatment for patients with paroxysmal nocturnal hemoglobinuria (PNH), a debilitating, ultra-rare and life-threatening blood disorder, characterized by complement-mediated hemolysis (destruction of red blood cells). Soliris is indicated to reduce hemolysis. Soliris is also approved in the US (2011), European Union (2011), and Japan (2013) as the first and only treatment for patients with atypical hemolytic uremic syndrome (aHUS), a debilitating, ultra-rare and life-threatening genetic disorder characterized by complement-mediated thrombotic microangiopathy, or TMA (blood clots in small vessels). Soliris is indicated to inhibit complement-mediated TMA. The effectiveness of Soliris in aHUS is based on the effects on TMA and renal function. Prospective clinical trials in additional patients, the preliminary results of which are reported here at ASN, are ongoing to confirm the benefit of Soliris in patients with aHUS. Soliris is not indicated for the treatment of patients with Shiga toxin E. coli related hemolytic uremic syndrome (STEC-HUS). For the breakthrough innovation in complement inhibition, Alexion and Soliris have received the pharmaceutical industry's highest honors: the 2008 Prix Galien USA Award for Best Biotechnology Product with broad implications for future biomedical research and the 2009 Prix Galien France Award in the category of Drugs for Rare Diseases. More information including the full prescribing information on Soliris is available at www.soliris.net.
Important Safety Information
The US product label for Soliris includes a boxed warning: "Life-threatening and fatal meningococcal infections have occurred in patients treated with Soliris. Meningococcal infection may become rapidly life-threatening or fatal if not recognized and treated early. Comply with the most current Advisory Committee on Immunization Practices (ACIP) recommendations for meningococcal vaccination in patients with complement deficiencies. Immunize patients with a meningococcal vaccine at least 2 weeks prior to administering the first dose of Soliris, unless the risks of delaying Soliris therapy outweigh the risk of developing a meningococcal infection. (See Serious Meningococcal Infections (5.1) for additional guidance on the management of meningococcal infection.) Monitor patients for early signs of meningococcal infections and evaluate immediately if infection is suspected. Soliris is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS). Under the Soliris REMS, prescribers must enroll in the program. Enrollment in the Soliris REMS program and additional information are available by telephone: 1-888-soliris (1-888-765-4747)."
In patients with PNH, the most frequently reported adverse events observed with Soliris treatment in clinical studies were headache, nasopharyngitis (runny nose), back pain and nausea. Soliris treatment of patients with PNH should not alter anticoagulant management because the effect of withdrawal of anticoagulant therapy during Soliris treatment has not been established. In patients with aHUS, the most frequently reported adverse events observed with Soliris treatment in clinical studies were hypertension, upper respiratory tract infection, diarrhea, headache, anemia, vomiting, nausea, urinary tract infection, and leukopenia. Please see full prescribing information for Soliris, including boxed WARNING regarding risk of serious meningococcal infection.
About Alexion
Alexion Pharmaceuticals, Inc. is a biopharmaceutical company focused on serving patients with severe and ultra-rare disorders through the innovation, development and commercialization of life-transforming therapeutic products. Alexion is the global leader in complement inhibition and has developed and markets Soliris® (eculizumab) as a treatment for patients with PNH and aHUS, two debilitating, ultra-rare and life-threatening disorders caused by chronic uncontrolled complement activation. Soliris is currently approved in nearly 50 countries for the treatment of PNH, and in the United States, European Union, Japan and other countries for the treatment of aHUS. Alexion is evaluating other potential indications for Soliris in additional severe and ultra-rare disorders beyond PNH and aHUS, and is developing other highly innovative biotechnology product candidates across multiple therapeutic areas. This press release and further information about Alexion Pharmaceuticals, Inc. can be found at: www.alexionpharma.com.
Safe Harbor Statement
This news release contains forward-looking statements, including statements related to anticipated clinical development, regulatory and commercial milestones and potential health and medical benefits of Soliris® (eculizumab) for the potential treatment of patients with aHUS. Forward-looking statements are subject to factors that may cause Alexion's results and plans to differ from those expected, including for example, decisions of regulatory authorities regarding marketing approval or material limitations on the marketing of Soliris for its current or potential new indications, and a variety of other risks set forth from time to time in Alexion's filings with the Securities and Exchange Commission, including but not limited to the risks discussed in Alexion's Quarterly Report on Form 10-Q for the period ended September 30, 2013, and in Alexion's other filings with the Securities and Exchange Commission. Alexion does not intend to update any of these forward-looking statements to reflect events or circumstances after the date hereof, except when a duty arises under law.
References
(1) Greenbaum LA, Fila M, Tsimaratos M, et al. Eculizumab (ECU) inhibits thrombotic microangiopathy (TMA) and improves renal function in pediatric atypical hemolytic uremic syndrome (aHUS) patients (pts). Presented at American Society of Nephrology (ASN) Kidney Week 2013, Atlanta, Ga., November 9, 2013. Abstract SA-PO849.
(2) Fakhouri F, Hourmant M, Campistol JM, et al. Eculizumab (ECU) inhibits thrombotic microangiopathy (TMA) and improves renal function in adult patients (pts) with atypical hemolytic uremic syndrome (aHUS). Presented at American Society of Nephrology (ASN) Kidney Week 2013, Atlanta, Ga., November 8, 2013. Abstract FR-OR057.
(3) Delmas Y, Loirat C, Muus P, et al. Eculizumab (ECU) in atypical hemolytic uremic syndrome (aHUS) patients (pts) with long disease duration and chronic kidney disease (CKD): sustained efficacy at 3 years. Presented at American Society of Nephrology (ASN) Kidney Week 2013, Atlanta, Ga., November 8, 2013. Abstract FR-PO536.
(4) Gaber O, Loirat C, Greenbaum L, et al. Eculizumab (ECU) maintains efficacy in atypical hemolytic uremic syndrome (aHUS) patients (pts) with progressing thrombotic microangiopathy (TMA): 3-year (yr) update. Presented at American Society of Nephrology (ASN) Kidney Week 2013, Atlanta, Ga., November 9, 2013. Abstract SA-PO852.
(5) Licht C, Ardissino G, Ariceta G, et al. An observational, non-interventional, multicenter, multinational registry of patients (pts) with atypical hemolytic uremic syndrome (aHUS): initial pt characteristics. Presented at American Society of Nephrology (ASN) Kidney Week 2013, Atlanta, Ga., November 9, 2013. Abstract SA-PO853.
(6) Noris M, Remuzzi G. Atypical hemolytic-uremic syndrome. N Engl J Med. 2009;361:1676-87.
(7) Noris M, Caprioli J, Bresin E, et al. Relative role of genetic complement abnormalities in sporadic and familial aHUS and their impact on clinical phenotype. Clin J Am Soc Nephrol. 2010;5:1844-59.
(8) Caprioli J, Noris M, Brioschi S, et al. The impact of MCP, CFH, and IF mutations on clinical presentation, response to treatment, and outcome. Blood. 2006;108:1267-9.
(9) Vilalta R, Al-Akash S, Davin J, et al. Eculizumab therapy for pediatric patients with atypical hemolytic uremic syndrome: efficacy and safety outcomes of a retrospective study [abstract 1155]. Haematologica. 2012;97(suppl 1):479.
(10) Dr. Larry Greenbaum receives research support from Alexion Pharmaceuticals, Inc. and is a consultant to the company.
(11) Dr. Fadi Fakhouri receives research support from Alexion Pharmaceuticals, Inc. and is a consultant to the company.
(12) Dr. Yahsou Delmas receives research support from Alexion Pharmaceuticals, Inc. and is a consultant to the company.
(13) Dr. A. Osama Gaber receives research support from Alexion Pharmaceuticals, Inc. and is a consultant to the company.
(14) Benz K, Amann K. Thrombotic microangiopathy: new insights. Curr Opin Nephrol Hypertens. 2010;19(3):242-7.
(15) Ariceta G, Besbas N, Johnson S, et al. Guideline for the investigation and initial therapy of diarrhea-negative hemolytic uremic syndrome. Pediatr Nephrol. 2009;24:687-96.
(16) Tsai HM. The molecular biology of thrombotic microangiopathy. Kidney Int. 2006;70(1):16-23.
(17) Loirat C, Garnier A, Sellier-Leclerc AL, Kwon T. Plasmatherapy in atypical hemolytic uremic syndrome. Semin Thromb Hemost. 2010;36:673-81.
(18) Bresin E, Daina E, Noris M, et al. Outcome of renal transplantation in patients with non-Shiga toxin-associated hemolytic uremic syndrome: prognostic significance of genetic background. Clin J Am Soc Nephrol. 2006;1:88-99.
Earnings reported on 10/24 before market opening. should be pretty good.
Alxn - wtf just happened wow
Wells Fargo Conference
Discuss about aHUS & more at conference..
Read here
7:33AM Alexion Pharma received a Warning Letter from the U.S. Food and Drug Administration regarding compliance with current Good Manufacturing Practices at its Rhode Island manufacturing facility (ALXN) 93.92 : In an 8-K released this morning, the co reported that on March 27, 2013, Alexion Pharmaceuticals received a Warning Letter from the U.S. Food and Drug Administration (FDA) regarding compliance with current Good Manufacturing Practices (cGMP) at its Rhode Island manufacturing facility. The Warning Letter follows an FDA inspection which concluded on August 6, 2012. At the conclusion of that inspection, the FDA issued a Form 483 Inspectional Observations, to which Alexion responded in August 2012 and provided additional information to the FDA in September and December 2012. The observations concern commercial and clinical manufacture of Soliris at this facility.
"Based on current information, we believe that the supply of Soliris to patients will not be interrupted and that the Warning Letter does not restrict production of Soliris or shipment of Soliris from the Rhode Island facility. We continue to manufacture products, including Soliris, in this facility. Additionally, a third party manufacturing facility is currently approved worldwide for production of Soliris. Further, an additional third party manufacturing facility was validated in 2012 for production of Soliris, and we are currently completing our regulatory submissions for this facility. We anticipate first approval for this additional facility to occur in Q4 of 2013. Finally, we estimate that our current inventory of Soliris licensed for commercial sale is sufficient for at least four-thousand patient-years of patient treatment."
"Unless and until we are able to correct outstanding issues to the FDA's satisfaction, the FDA may withhold approval of requests for export certificates for certain countries. The FDA may also withhold approval of pending drug applications listing the Rhode Island facility. We will notify appropriate international regulatory authorities of the Warning Letter, and it is possible that the letter may impact our ability to supply Soliris manufactured at our Rhode Island facility outside the United States."
Alexion Pharmaceuticals Inc. Stock Buy Recommendation Reiterated (ALXN)
By TheStreet Wire 01/18/13 - 09:00 AM EST
Find out if (ALXN) is in Cramer's Portfolio.
Editor's Note: TheStreet ratings do not represent the views of TheStreet's staff or its contributors. Ratings are established by computer based on metrics for performance (which includes growth, stock performance, efficiency and valuation) and risk (volatility and solvency). Companies with poor cash flow or high debt levels tend to earn lower ratings in our model.
NEW YORK (TheStreet) -- Alexion Pharmaceuticals (Nasdaq:ALXN) has been reiterated by TheStreet Ratings as a buy with a ratings score of B . The company's strengths can be seen in multiple areas, such as its robust revenue growth, largely solid financial position with reasonable debt levels by most measures, expanding profit margins, good cash flow from operations and impressive record of earnings per share growth. We feel these strengths outweigh the fact that the company has had somewhat disappointing return on equity.
EXCLUSIVE OFFER: Jim Cramer's Protégé, Dave Peltier, only buys Stocks Under $10 that he thinks could potentially double. See what he's trading today with a 14-day FREE pass
Highlights from the ratings report include:
The revenue growth greatly exceeded the industry average of 5.4%. Since the same quarter one year prior, revenues rose by 44.1%. Growth in the company's revenue appears to have helped boost the earnings per share.
ALXN's debt-to-equity ratio is very low at 0.09 and is currently below that of the industry average, implying that there has been very successful management of debt levels. Along with this, the company maintains a quick ratio of 3.36, which clearly demonstrates the ability to cover short-term cash needs.
ALEXION PHARMACEUTICALS INC has improved earnings per share by 35.3% in the most recent quarter compared to the same quarter a year ago. The company has demonstrated a pattern of positive earnings per share growth over the past year. We feel that this trend should continue. During the past fiscal year, ALEXION PHARMACEUTICALS INC increased its bottom line by earning $0.91 versus $0.53 in the prior year. This year, the market expects an improvement in earnings ($2.05 versus $0.91).
The net income growth from the same quarter one year ago has greatly exceeded that of the S&P 500, but is less than that of the Biotechnology industry average. The net income increased by 40.6% when compared to the same quarter one year prior, rising from $65.57 million to $92.18 million.
The gross profit margin for ALEXION PHARMACEUTICALS INC is currently very high, coming in at 90.80%. It has increased from the same quarter the previous year. Along with this, the net profit margin of 31.33% is above that of the industry average.
Alexion Pharmaceuticals, Inc., a biopharmaceutical company, engages in the discovery, development, and commercialization of biologic therapeutic products in the United States, Europe, Latin America, Japan, and the Asia Pacific. Alexion has a market cap of $19.08 billion and is part of the health care sector and drugs industry. The company has a P/E ratio of 86.9, above the S&P 500 P/E ratio of 17.7. Shares are up 4.8% year to date as of the close of trading on Wednesday.
6:36AM Alexion Pharma beats by $0.13, reports revs in-line; co raises and guides FY12 EPS above consensus, raises rev guidance, in-line (ALXN) 100.94 : Reports Q3 (Sep) earnings of $0.60 per share, $0.13 better than the Capital IQ Consensus Estimate of $0.47; revenues rose 44.2% year/year to $294.1 mln vs the $294.02 mln consensus. Co raises and issues upside guidance for FY12, sees EPS of $1.99-2.04 vs. $1.89 Capital IQ Consensus Estimate and above prior guidance of $1.78-1.88; sees FY12 revs of toward higher end of $1.12-1.13 bln vs. $1.13 bln Capital IQ Consensus Estimate, which is above prior guidance of $1.110-1.125 bln. The upward revision reflects continued global growth of Soliris in PNH and growth from the ongoing launch of Soliris in aHUS. Revenue performance for the quarter reflected steady additions of new patients with paroxysmal nocturnal hemoglobinuria commencing Soliris therapy in Alexion's core territories of the US, Western Europe and Japan, as well as in new countries. Revenues were further augmented by an increasing number of new patients with atypical hemolytic uremic syndrome commencing Soliris treatment.
6:36AM Alexion Pharma beats by $0.11, beats on revs; raises FY12 EPS most of range above consensus, raises FY12 revs above consensus (ALXN) 97.55 : Reports Q2 (Jun) earnings of $0.47 per share, excluding non-recurring items, $0.11 better than the Capital IQ Consensus Estimate of $0.36; revenues rose 50.6% year/year to $279.7 mln vs the $262.97 mln consensus. Co raised guidance for FY12, sees EPS of $1.78-1.88 from prior guidance of $1.65-1.75 vs. $1.78 Capital IQ Consensus Estimate; raised FY12 revs to $1.110-1.125 bln from prior guidance of $1.065-1.085 bln vs. $1.09 bln Capital IQ Consensus Estimate. The European Commission has granted orphan designation for eculizumab as a treatment for patients with STEC-HUS, a severe, ultra-rare, and life-threatening inflammatory disorder. Separately, enrollment continues in a Company-sponsored, multi-national, living-donor kidney transplant trial in patients at elevated risk of acute humoral rejection, also known as antibody mediated rejection, and the Company has initiated a deceased-donor kidney transplant study with enrollment expected to begin later this year.
12:40AM Alexion Pharma presents data show majority of patients with aHUS experienced systemic multi-organ complications prior to treatment (ALXN) 93.31 : Co announces the presentation of data that underscore the critical need for testing patients at high risk for paroxysmal nocturnal hemoglobinuria and new data on the potentially life-threatening, systemic complications in patients with atypical hemolytic uremic syndrome. A retrospective analysis of 30 pediatric and adult patients with aHUS showed that the majority of patients experienced severe complications of the disease across multiple organs, despite receiving supportive care, including plasma exchange or plasma infusion. These data underscore the risk for sudden and potentially fatal systemic complications of aHUS.1 In a separate analysis of 19 pediatric patients with aHUS, Soliris significantly reduced thrombotic microangiopathy, or TMA, leading to improved kidney function and eliminating the need for dialysis in half of patients who previously required it before starting on Soliris therapy. In a poster session on Friday, June 15, researchers presented retrospective data from an analysis of 30 pediatric and adult patients with aHUS prior to receiving Soliris. All 30 patients (100%) showed evidence of kidney impairment. Extra-renal, systemic organ complications were reported in 63% of patients (19 of 30), and extra-renal thrombi were reported in 37% of patients (11 of 30).1 These complications spanned the cardiovascular (47% of patients), gastrointestinal (37%) and neurological (20%) systems, and were similarly reported in aHUS patients with or without identified genetic complement mutation.
<<< $ALXN Links! >>> ~ MAC's Quick DD Links without the charts.


PennyStockTweets ~ http://www.pennystocktweets.com/stocks/profile/ALXN
OTC Markets Company Info ~ http://www.otcmarkets.com/stock/ALXN/company-info
OTC Markets Charts ~ http://www.otcmarkets.com/stock/ALXN/chart
OTC Markets Quote ~ http://www.otcmarkets.com/stock/ALXN/quote
OTC Markets News ~ http://www.otcmarkets.com/stock/ALXN/news
OTC Markets Financials ~ http://www.otcmarkets.com/stock/ALXN/financials
OTC Markets Short Sales ~ http://www.otcmarkets.com/stock/ALXN/short-sales
OTC Markets Insider Disclosure ~ http://www.otcmarkets.com/stock/ALXN/insider-transactions
OTC Markets Research Reports ~ http://www.otcmarkets.com/stock/ALXN/research

Google Finance Summary ~ http://www.google.com/finance?q=ALXN
Google Finance News ~ http://www.google.com/finance/company_news?q=ALXN
Google Finance Option chain ~ http://www.google.com/finance/option_chain?q=ALXN
Google Finance Financials ~ http://www.google.com/finance?q=ALXN&fstype=ii#
Google Finance Historical prices Daily ~ http://www.google.com/finance/historical?q=ALXN
Google Finance Historical prices Weekly ~ http://www.google.com/finance/historical?q=ALXN&histperiod=weekly#

Y! < Company >
Y! Profile ~ http://finance.yahoo.com/q/pr?s=ALXN+Profile
Y! Key Stat's ~ http://finance.yahoo.com/q/ks?s=ALXN+Key+Statistics
Y! Headlines ~ http://finance.yahoo.com/q/h?s=ALXN+Headlines
Y! Summary ~ http://finance.yahoo.com/q?s=ALXN
Y! Historical Prices ~ http://finance.yahoo.com/q/hp?s=ALXN+Historical+Prices
Y! Order Book ~ http://finance.yahoo.com/q/ecn?s=ALXN+Order+Book
Y! Message Boards ~ http://messages.finance.yahoo.com/mb/ALXN
Y! Market Pulse ~ http://finance.yahoo.com/marketpulse/ALXN
Y! Technical Analysis ~ http://finance.yahoo.com/q/ta?s=ALXN+Basic+Tech.+Analysis
Y! < Analyst Coverage >
Y! Analyst Opinion ~ http://finance.yahoo.com/q/ao?s=ALXN+Analyst+Opinion
Y! Analyst Estimates ~ http://finance.yahoo.com/q/ae?s=ALXN+Analyst+Estimates
Y! Research Reports ~ http://finance.yahoo.com/q/rr?s=ALXN+Research+Reports
Y! Star Analysts ~ http://finance.yahoo.com/q/sa?s=ALXN+Star+Analysts
Y! < Ownership >
Y! Major Holders ~ http://finance.yahoo.com/q/mh?s=ALXN+Major+Holders
Y! Insider Transactions ~ http://finance.yahoo.com/q/it?s=ALXN+Insider+Transactions
Y! Insider Roster ~ http://finance.yahoo.com/q/ir?s=ALXN+Insider+Roster
Y! < Financials >
Y! Income Statement ~ http://finance.yahoo.com/q/is?s=ALXN+Income+Statement&annual
Y! Balance Sheet ~ http://finance.yahoo.com/q/bs?s=ALXN+Balance+Sheet&annual
Y! Cash Flow ~ http://finance.yahoo.com/q/cf?s=ALXN+Cash+Flow&annual

FINVIZ ~ http://finviz.com/quote.ashx?t=ALXN&ty=c&ta=0&p=d
Investorshub Trades ~ http://ih.advfn.com/p.php?pid=trades&symbol=ALXN
Investorshub Board Search ~ http://investorshub.advfn.com/boards/getboards.aspx?searchstr=ALXN
Investorshub PostStream ~ http://investorshub.advfn.com/boards/poststream.aspx?ticker=ALXN
Investorshub Messages ~ http://investorshub.advfn.com/boards/msgsearch.aspx?SearchStr=ALXN
Investorshub Videos ~ http://ih.advfn.com/p.php?pid=ihvse&ihvqu=ALXN
Investorshub News ~ http://ih.advfn.com/p.php?pid=news&btn=s_ok&ctl00%24sb3%24tbq1=Get+Quote&as_values_IH=&ctl00%24sb3%24stb1=Search+iHub&symbol=ALXN&s_ok=OK&from_month=3&from_day=15&from_year=2012&order=desc&selsrc%5B%5D=prnca&selsrc%5B%5D=prnus&selsrc%5B%5D=zacks&selsrc%5B%5D=money2&selsrc%5B%5D=djn&selsrc%5B%5D=bw&selsrc%5B%5D=globe&selsrc%5B%5D=edgar&selsrc%5B%5D=mwus&force=1&last_ts=1331855999&p_n=1&p_count=&p_ts=1331794260
CandlestickChart ~ http://www.candlestickchart.com/cgi/chart.cgi?symbol=ALXN&exchange=US
Barchart Quote ~ http://barchart.com/quotes/stocks/ALXN?
Barchart Detailed Quote ~ http://barchart.com/detailedquote/stocks/ALXN
Barchart Options Quotes ~ http://barchart.com/options/stocks/ALXN
Barchart Technical Chart ~ http://barchart.com/charts/stocks/ALXN&style=technical
Barchart Interactive Chart ~ http://barchart.com/charts/stocks/ALXN&style=interactive
Barchart Technical Analysis ~ http://barchart.com/technicals/stocks/ALXN
Barchart Trader's Cheat Sheet ~ http://barchart.com/cheatsheet.php?sym=ALXN
Barchart Barchart Opinion ~ http://barchart.com/opinions/stocks/ALXN
Barchart Snapshot Opinion ~ http://barchart.com/snapopinion/stocks/ALXN
Barchart News Headlines ~ http://barchart.com/news/stocks/ALXN
Barchart Profile ~ http://barchart.com/profile//ALXN
Barchart Key Statistics ~ http://barchart.com/profile.php?sym=ALXN&view=key_statistics
OTC: American Bulls ~ http://www.americanbulls.com/StockPage.asp?CompanyTicker=ALXN&MarketTicker=OTC&TYP=S
NASDAQ: American Bulls ~ http://www.americanbulls.com/StockPage.asp?CompanyTicker=ALXN&MarketTicker=NASD&TYP=S
NYSE: American Bulls ~ http://www.americanbulls.com/StockPage.asp?CompanyTicker=ALXN&MarketTicker=NYSE&Typ=S

Marketwatch Profile ~ http://www.marketwatch.com/investing/stock/ALXN/profile
Marketwatch Analyst Estimates ~ http://www.marketwatch.com/investing/stock/ALXN/analystestimates
Marketwatch Historical Quotes ~ http://www.marketwatch.com/investing/stock/ALXN/historical
Marketwatch Financials ~ http://www.marketwatch.com/investing/stock/ALXN/financials
Marketwatch Overview ~ http://www.marketwatch.com/investing/stock/ALXN
Marketwatch SEC Filings ~ http://www.marketwatch.com/investing/stock/ALXN/secfilings
Marketwatch Picks ~ http://www.marketwatch.com/investing/stock/ALXN/picks
Marketwatch Hulbert ~ http://www.marketwatch.com/investing/stock/ALXN/hulbert
Marketwatch Insider Actions ~ http://www.marketwatch.com/investing/stock/ALXN/insideractions
Marketwatch Options ~ http://www.marketwatch.com/investing/stock/ALXN/options
Marketwatch Charts ~ http://www.marketwatch.com/investing/stock/ALXN/charts
Marketwatch News ~ http://bigcharts.marketwatch.com/news/symbolsearch/symbolnews.asp?news=markadv&symb=ALXN&sid=1795093&framed=False
The Lion ~ http://thelion.com/bin/aio_msg.cgi?cmd=search&msg=&si=1&tw=1&tt=1&rb=1&ih=1&fo=1&iv=1&yf=1&sa=1&fb=1&gg=1&symbol=ALXN
Search NYSE ~ http://www.nyse.com/about/listed/lcddata.html?ticker=ALXN

StockTA ~ http://www.stockta.com/cgi-bin/analysis.pl?symb=ALXN&num1=567&cobrand=&mode=stock
StockHouse ~ http://www.stockhouse.com/financialtools/sn_overview.aspx?qm_symbol=ALXN
StockHouse Delayed LII ~ http://www.stockhouse.com/financialtools/sn_level2.aspx?qm_page=46140&qm_symbol=ALXN

AlphaTrade ~ http://tools.alphatrade.com/index.php?t1=mc_quote_module&t2=mc_quote_module2&t3=historical&template=historical2html&sym=ALXN&client_id=2740&a_width=680&a_height=1000&language=english&showVol=1&chtype=8

Reuters ~ http://www.reuters.com/finance/stocks/companyOfficers?symbol=ALXN.PK&WTmodLOC=C4-Officers-5
StockWatch ~ http://www.stockwatch.com/Quote/Detail.aspx?symbol=ALXN®ion=U
Search NASDAQ ~ http://www.nasdaq.com/symbol/ALXN
NASDAQ Divy History ~ http://www.nasdaq.com/symbol/ALXN/dividend-history
NASDAQ Short Interest ~ http://www.nasdaq.com/symbol/ALXN/short-interest
NASDAQ Institutional Ownership ~ http://www.nasdaq.com/symbol/ALXN/institutional-holdings
NASDAQ FlashQuotes ~ http://www.nasdaq.com/aspx/flashquotes.aspx?symbol=ALXN&selected=ALXN
NASDAQ InfoQuotes ~ http://www.nasdaq.com/aspx/infoquotes.aspx?symbol=ALXN&selected=ALXN
NASDAQ After Hours Quote ~ http://www.nasdaq.com/symbol/ALXN/after-hours
NASDAQ Pre-Market Quote ~ http://www.nasdaq.com/symbol/ALXN/premarket
NASDAQ Historical Quote ~ http://www.nasdaq.com/symbol/ALXN/historical
NASDAQ Option Chain ~ http://www.nasdaq.com/symbol/ALXN/option-chain
NASDAQ Company Headlines ~ http://www.nasdaq.com/symbol/ALXN/news-headlines
NASDAQ Press Releases ~ http://www.nasdaq.com/symbol/ALXN/news-headlines
NASDAQ Sentiment ~ http://www.nasdaq.com/symbol/ALXN/sentiment
NASDAQ Analyst Summary ~ http://www.nasdaq.com/symbol/ALXN/analyst-research
NASDAQ Guru Analysis~ http://www.nasdaq.com/symbol/ALXN/guru-analysis
NASDAQ Stock Report ~ http://www.nasdaq.com/symbol/ALXN/stock-report
NASDAQ Competitors ~ http://www.nasdaq.com/symbol/ALXN/competitors
NASDAQ Stock Consultant ~ http://www.nasdaq.com/symbol/ALXN/stock-consultant
NASDAQ Stock Comparison ~ http://www.nasdaq.com/symbol/ALXN/stock-comparison
NASDAQ Call Transcripts ~ http://www.nasdaq.com/symbol/ALXN/call-transcripts
NASDAQ Annual Reports ~ http://www.nasdaq.com/aspx/annualreport.aspx?symbol=ALXN&selected=ALXN
NASDAQ Financials ~ http://www.nasdaq.com/symbol/ALXN/financials
NASDAQ Revenue & Earnings Per Share (EPS) ~ http://www.nasdaq.com/symbol/ALXN/revenue-eps
NASDAQ SEC Filings ~ http://www.nasdaq.com/symbol/ALXN/sec-filings
NASDAQ Ownership Summary ~ http://www.nasdaq.com/symbol/ALXN/ownership-summary
NASDAQ Institutional Ownership ~ http://www.nasdaq.com/symbol/ALXN/institutional-holdings
NASDAQ (SEC Form 4) ~
--------- All Trades ~ http://www.nasdaq.com/symbol/ALXN/insider-trades
--------- Buys ~ http://www.nasdaq.com/symbol/ALXN/insider-trades/buys
--------- Sells ~ http://www.nasdaq.com/symbol/ALXN/insider-trades/sells
The Motley Fool ~ http://caps.fool.com/Ticker/ALXN.aspx
The Motley Fool Earnings/Growth ~ http://caps.fool.com/Ticker/ALXN/EarningsGrowthRates.aspx?source=itxsittst0000001
The Motley Fool Ratios ~ http://caps.fool.com/Ticker/ALXN/Ratios.aspx?source=itxsittst0000001
The Motley Fool Stats ~ http://caps.fool.com/Ticker/ALXN/Stats.aspx?source=icasittab0000006
The Motley Fool Historical ~ http://caps.fool.com/Ticker/ALXN/Historical.aspx?source=icasittab0000004
The Motley Fool Scorecard ~ http://caps.fool.com/Ticker/ALXN/Scorecard.aspx?source=icasittab0000003
The Motley Fool Statements ~ http://caps.fool.com/Ticker/ALXN/Statements.aspx?source=icasittab0000009

MSN Money ~ http://investing.money.msn.com/investments/stock-ratings?symbol=ALXN
YCharts ~ http://ycharts.com/companies/ALXN
YCharts Performance ~ http://ycharts.com/companies/ALXN/performance
YCharts Dashboard ~ http://ycharts.com/companies/ALXN/dashboard
InsideStocks Opinion ~ http://www.insidestocks.com/texpert.asp?sym=ALXN&code=XDAILY
InsideStocks Profile ~ http://www.insidestocks.com/profile.asp?sym=ALXN&code=XDAILY
InsideStocks Quote ~ http://www.insidestocks.com/quote.asp?sym=ALXN&code=XDAILY
InsideStocks Projection ~ http://charts3.barchart.com/procal.asp?sym=ALXN
Zacks Quote ~ http://www.zacks.com/stock/quote/ALXN
Zacks Estimates ~ http://www.zacks.com/research/report.php?type=estimates&t=ALXN
Zacks Company Reports ~ http://www.zacks.com/research/report.php?type=report&t=ALXN

Knobias ~ http://knobias.10kwizard.com/files.php?sym=ALXN
StockScores ~ http://www.stockscores.com/quickreport.asp?ticker=ALXN
Trade-Ideas ~ http://www.trade-ideas.com/StockInfo/ALXN/HOT_TOPIC.html
Morningstar ~ http://performance.morningstar.com/stock/performance-return.action?region=USA&t=ALXN&culture=en-US
Morningstar Shareholders ~ http://investors.morningstar.com/ownership/shareholders-overview.html?t=ALXN®ion=USA&culture=en-us
Morningstar Transcripts~ http://www.morningstar.com/earnings/NoTranscript.aspx?t=ALXN®ion=USA
Morningstar Key Ratios ~ http://financials.morningstar.com/ratios/r.html?t=ALXN®ion=USA&culture=en-US
Morningstar Executive Compensation ~ http://insiders.morningstar.com/trading/executive-compensation.action?t=ALXN®ion=USA&culture=en-us
Morningstar Valuation ~ http://financials.morningstar.com/valuation/price-ratio.html?t=ALXN®ion=USA&culture=en-us
CCBN (Thompson Reuters) ~ http://ccbn.aol.com/company.asp?client=aol&ticker=ALXN

TradingMarkets ~ http://pr.tradingmarkets.com/?lid=leftPRbox&sym=ALXN

OTCBB ~ http://www.otcbb.com/asp/SiteSearch.asp?Criteria=ALXN&searcharea=e&image1.x=0&image1.y=0
Insidercow ~ http://www.insidercow.com/history/company.jsp?company=ALXN&B1=Search%21
Forbes News ~ http://search.forbes.com/search/find?tab=searchtabgeneraldark&MT=ALXN
Forbes Press Releases ~ http://search.forbes.com/search/find?&start=1&tab=searchtabgeneraldark&MT=ALXN&pub=businesswire,prnewswire&searchResults=pressRelease&tag=pr&premium=on
Forbes Web ~ http://search.forbes.com/search/web?MT=UNGS&start=1&max=10&searchResults=web&tag=web&sort=null

YouTube Symbol Search ~ http://www.youtube.com/results?search_query=ALXN
Buy-Ins ~ http://www.buyins.net/tools/symbol_stats.php?sym=ALXN
Quotemedia ~ http://www.quotemedia.com/results.php?qm_page=47556&qm_symbol=ALXN

Earnings Whispers ~ http://www.earningswhispers.com/stocks.asp?symbol=ALXN
Bloomberg Snapshot ~ http://investing.businessweek.com/research/stocks/snapshot/snapshot.asp?ticker=ALXN
Bloomberg People ~ http://investing.businessweek.com/research/stocks/people/people.asp?ticker=ALXN
Financial Times ~ http://markets.ft.com/Research/Markets/Tearsheets/Summary?s=ALXN
Investorpoint ~ http://www.investorpoint.com/ enter "ALXN" and click search.
Hotstocked ~ http://www.hotstocked.com/ enter "ALXN" and click search.
Raging Bull ~ http://ragingbull.quote.com/mboard/boards.cgi?board=ALXN
Hoovers ~ http://www.hoovers.com/search/company-search-results/100003765-1.html?type=company&term=ALXN
DD Machine ~ http://www.ddmachine.com/default.asp?m=stocktool_frame.asp?symbol=ALXN
SEC Form 4 ~ http://www.secform4.com/insider/showhistory.php?cik=ALXN
OTCBB Pulse ~ http://www.otcbbpulse.com/cgi-bin/pulsequote.cgi?symbol=ALXN
Failures To Deliver ~ http://failurestodeliver.com/default2.aspx enter "ALXN" and click search.
http://www.coordinatedlegal.com/SecretaryOfState.html
http://regsho.finra.org/regsho-Index.html
http://www.shortsqueeze.com/?symbol=ALXN&submit=Short+Quote%99

DTCC (PENSON/TDA) Check - (otc and pinks) - Note ~ I did not check for this chart blast. However, I try and help you to do so with the following links.
IHUB DTCC BOARD SEARCH #1 http://investorshub.advfn.com/boards/msgsearchbyboard.aspx?boardID=18682&srchyr=2011&SearchStr=ALXN
IHUB DTCC BOARD SEARCH #2: http://investorshub.advfn.com/boards/msgsearchbyboard.aspx?boardID=14482&srchyr=2011&SearchStr=ALXN
Check those searches for recent ALXN mentions. If ALXN is showing up on older posts and not on new posts found in link below, The DTCC issues may have been addressed and fixed. Always call the broker if your security turns up on any DTCC/PENSON list.
http://investorshub.advfn.com/boards/msgsearchbyboard.aspx?boardID=18682&srchyr=2011&SearchStr=Complete+list
For a complete list see the pinned threads at the top here ---> http://tinyurl.com/TWO-OLD-FARTS
 MACDlinks
MACDlinks
~ Tuesday! $ALXN ~ Q1 Earnings posted, pending or coming soon! In Charts and Links Below!
~ $ALXN ~ Earnings expected on Tuesday *
Want more like this? Search Keyword: MACMONEY >>> http://tinyurl.com/MACMONEY <<<
One or more of many earnings sites has alerted this security has or will be posting earnings on or around the day of this message.


http://stockcharts.com/h-sc/ui?s=ALXN&p=D&b=3&g=0&id=p88783918276&a=237480049

http://stockcharts.com/h-sc/ui?s=ALXN&p=W&b=3&g=0&id=p54550695994

 ~ Google Finance: http://www.google.com/finance?q=ALXN
~ Google Finance: http://www.google.com/finance?q=ALXN
~ Google Fin Options: hhttp://www.google.com/finance/option_chain?q=ALXN#
 ~ Yahoo! Finance ~ Stats: http://finance.yahoo.com/q/ks?s=ALXN+Key+Statistics
~ Yahoo! Finance ~ Stats: http://finance.yahoo.com/q/ks?s=ALXN+Key+Statistics
~ Yahoo! Finance ~ Profile: http://finance.yahoo.com/q/pr?s=ALXN
 Finviz: http://finviz.com/quote.ashx?t=ALXN
Finviz: http://finviz.com/quote.ashx?t=ALXN
 ~ BusyStock: http://busystock.com/i.php?s=ALXN&v=2
~ BusyStock: http://busystock.com/i.php?s=ALXN&v=2

<<<<<< http://www.earningswhispers.com/stocks.asp?symbol=ALXN >>>>>>


http://investorshub.advfn.com/boards/post_prvt.aspx?user=251916
*If the earnings date is in error please ignore error. I do my best.
Alexion (ALXN), with its only product Soliris, bases its strategy on treating ultra-rare diseases. This company established itself quite quickly on the market where it had no competitor for its niche. Soliris holds a world record for the most expensive medicine. This certainly helps Alexion's incredible earnings growth rate.
http://seekingalpha.com/article/489571-questcor-a-strong-play-in-pharma?source=yahoo
~ $ALXN ~ Earnings posted, pending or coming soon! In Charts and Links Below!
~ $ALXN ~ Earnings expected on Monday *
This Week In Earnings: Earnings are coming or are already posted! This is what the charts look like! If you play the earnings these posts can be very helpful to you!
Want more like this? Search Keyword: MACMONEY >>> http://tinyurl.com/MACMONEY <<<
One or more of many earnings sites has alerted this security has or will be posting earnings on or around the day of this message.
http://stockcharts.com/h-sc/ui?s=ALXN&p=D&b=3&g=0&id=p88783918276&a=237480049
http://stockcharts.com/h-sc/ui?s=ALXN&p=W&b=3&g=0&id=p54550695994
 ~ Barchart: http://barchart.com/quotes/stocks/ALXN?
~ Barchart: http://barchart.com/quotes/stocks/ALXN?
 ~ OTC Markets: http://www.otcmarkets.com/stock/ALXN/company-info
~ OTC Markets: http://www.otcmarkets.com/stock/ALXN/company-info
~ Google Finance: http://www.google.com/finance?q=ALXN
~ Google Fin Options: hhttp://www.google.com/finance/option_chain?q=ALXN#
~ Yahoo! Finance ~ Stats: http://finance.yahoo.com/q/ks?s=ALXN+Key+Statistics
~ Yahoo! Finance ~ Profile: http://finance.yahoo.com/q/pr?s=ALXN
Finviz: http://finviz.com/quote.ashx?t=ALXN
~ BusyStock: http://busystock.com/i.php?s=ALXN&v=2
 ~ CandlestickChart: http://www.candlestickchart.com/cgi/chart.cgi?symbol=ALXN&exchange=US
~ CandlestickChart: http://www.candlestickchart.com/cgi/chart.cgi?symbol=ALXN&exchange=US
 ~ Investorshub Trades: http://ih.advfn.com/p.php?pid=trades&symbol=ALXN
~ Investorshub Trades: http://ih.advfn.com/p.php?pid=trades&symbol=ALXN
~ Investorshub Board Search: http://investorshub.advfn.com/boards/getboards.aspx?searchstr=ALXN
~ Investorshub PostStream Search: http://investorshub.advfn.com/boards/poststream.aspx?ticker=ALXN
~ Investorshub Goodies Search: http://investorshub.advfn.com/boards/msgsearchbyboard.aspx?boardID=18582&srchyr=2011&SearchStr=ALXN
~ Investorshub Message Search: http://investorshub.advfn.com/boards/msgsearch.aspx?SearchStr=ALXN
 ~ MarketWatch: http://www.marketwatch.com/investing/stock/ALXN/profile
~ MarketWatch: http://www.marketwatch.com/investing/stock/ALXN/profile
 ~ E-Zone Chart: http://www.windchart.com/ezone/signals/?symbol=ALXN
~ E-Zone Chart: http://www.windchart.com/ezone/signals/?symbol=ALXN
~ 5-Min Wind: http://www.windchart.com/stockta/analysis?symbol=ALXN
~ 10-Min Wind: http://www.windchart.com/stockta/analysis?symbol=ALXN&size=l&frequency=10&color=g
~ 30-Min Wind: http://www.windchart.com/stockta/analysis?symbol=ALXN&size=l&frequency=30&color=g
~ 60-Min Wind: http://www.windchart.com/stockta/analysis?symbol=ALXN&size=l&frequency=60&color=g
http://investorshub.advfn.com/boards/post_prvt.aspx?user=251916
*If the earnings date is in error please ignore error. I do my best.
|
Followers
|
6
|
Posters
|
|
|
Posts (Today)
|
0
|
Posts (Total)
|
155
|
|
Created
|
05/20/08
|
Type
|
Free
|
| Moderators | |||

http://www.alexionpharm.com/
http://finance.yahoo.com/q/ks?s=ALXN
Alexion Pharmaceuticals, Inc., a biotechnology company, develops and delivers life-changing drug therapies for patients with serious and life-threatening medical conditions. It primarily engages in the discovery, development, and commercialization of biologic therapeutic products for the treatment of severe disease states, including hematologic diseases, cancer, and autoimmune disorders. The company markets Soliris (eculizumab) for the treatment of paroxysmal nocturnal hemoglobinuria (PNH), a rare and life-threatening blood disorder in the United States and Europe. It also is evaluating other potential indications for Soliris, as well as other formulations of eculizumab for additional clinical indications. In addition, it is developing antibody product candidates targeting the treatment of patients with severe unmet medical needs. The company's drug programs comprise DC-SIGN Mab, a cancer Vaccine; Eculizumab (intravitreal) for age-related macular degeneration; and Eculizumab (intravenous) for myasthenia gravis and multifocal motor neuropathy, which are under preclinical development stage; CD200 Mab for the treatment of chronic lymphocytic leukemia and multiple myeloma under Phase I clinical trial; and Eculizumab (intravenous) under Phase I/II clinical trial for the treatment of asthma. . Alexion Pharmaceuticals was founded in 1992 and is headquartered in Cheshire, Connecticut.

Headquartered in Cheshire, Connecticut, Alexion employs more than 700 people around the world. In addition to our corporate headquarters, Alexion’s facilities include a manufacturing plant in Smithfield, Rhode Island, EMEA (Europe, Middle East & Africa) regional headquarters in Lausanne, Switzerland, a European shared service center in Paris, distribution and sales operations in major markets throughout Europe, and new operations in Tokyo, Japan, Sydney, Australia, São Paulo, Brazil, Ontario, Canada and other countries. The company is also expanding its reach in Latin America, the Middle East and Africa.
Alexion’s global presence reflects the approval of Soliris for the treatment of patients with PNH in the United States, 29 European countries, Australia, Canada and other countries. The company is working toward seeking regulatory approval in other countries of Asia and South America.

| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |







