 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.


Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Anyone have any idea what this company is doing now?
With all that has been shown in the BETonMACE trial and them still holding out on the eGFR data,... I feel positive that once the Covid-19 pandemic has died down,.. they will announce a partner to go forward with the developement of Apabetalone.
I can't see the big investors in this just letting it go to zero with all that has been shown with the drug.
I think the only plan is survival. Apabetalone has failed two large heavily publicized trials (first one was in 2014). Not by much, but missed primary endpoints equal failure. IMO, they should sell to whoever will make an offer, if anyone comes forward. Otherwise this may go to zero. Where would the $ come from to fund another big trial?
The other related company, Zenith, still has significant value and buyout potential.
But what the heck do I know?
Any news about the future plans for this company?
69 cents. tempting, but holding off on everything for a while yet.
some will use this pop as an exit
Company still needs some sort of financial savior. Odds of getting one have increased with the BT designation.
Yes! Much quicker than expected!
BRIEF-Resverlogix Receives US FDA Breakthrough Therapy Designation For Apabetalone
But it doesn’t really matter what the analyst say. What matters is whether there’s a company willing to put up the money that will be required to do another phase 3
As far as I can tell so far it’s pretty much of a yawn
What do analysts say about the secondary analysis?
Seeing a "clear path to commercialization" at the end of the press release from the CEO is exciting news. Hopefully, this comes to fruition.
Interesting secondary analysis released today
The sad truth is that BetOnMace was a failure. Prospects are bleak. The planned raise by lowering the price of warrants to $1.33 Canadian no longer looks possible.
Too bad. BetOnMace was simply underpowered. Any savior that will fund the needed “bolt-on” will exact a heavy price, leaving shareholders in the dust. If no savior appears, it looks like the IP goes to the bond holders.
The statement in this release was optimistic to say the least
This one’s down about 40% the last couple weeks. In my view, it is like the head lower
Resverlogix Announces Change to its Board of Directors
CALGARY, Alberta, Dec. 11, 2019 (GLOBE NEWSWIRE) -- Resverlogix Corp. (“Resverlogix” or the "Company") (TSX: RVX) today announced that Dr. Eldon Smith has stepped down from the Board of Directors, effective today.
“We would like to thank Eldon for his many years of service and wish him all the best,” said Donald McCaffrey, President and CEO of the Company. “We appreciate Eldon’s many contributions and guidance over the years, helping to greatly advance our programs, and are excited to continue the development of apabetalone. The major opportunities in front of us are numerous. We continue to aggressively pursue a multi-point strategy that includes potential breakthrough status filings with regulators and strategic partnerships for multiple indications. All this on the heels of recent significant BETonMACE results which produced very encouraging data, particularly in the chronic kidney disease and cognitive decline patient groups. In addition, we uncovered positive surprise findings when apabetalone is combined with the new generation of diabetes drugs – SGLT2 inhibitors – in this CVD patient population. We look forward to providing further updates in the near future and look forward to a very prosperous 2020.”
cognitive results pres.
http://118009.choruscall.com/resverlogix/resverlogix20191206.pdf
ambiguous but holy cow!!!
CALGARY, Alberta, Dec. 05, 2019 (GLOBE NEWSWIRE) -- Resverlogix Corp. (“Resverlogix” or the "Company") (TSX: RVX) reminds stakeholders that the Company will hold a conference call and webcast on December 6th at 8:30 am ET to supplement the presentation of prespecified BETonMACE cognition results to be disclosed at the Clinical Trials on Alzheimer's Disease (“CtAD”) Congress 2019.
Among other findings, the Company will highlight that Apabetalone treatment illustrated statistically significant improvements compared to top standard of care placebo in cardiovascular disease patients with moderate to severe cognitive decline
Thanks. Time will tell.
Shop themselves to anyone with cash? If they can’t engineer a sale, they will have to raise funds for ckd and/or vascular dementia trials. Will know more after we get more results this week
Any ideas what their plans are for the next 3-4 months?
Not good. Here's hoping somebody buys them out.
They missed their primary endpoint and have to shift the goalposts to find the positive results. Same thing happened in 2014 and it took 5 years to get to this point. Now the goalposts have shifted again.
Oh yeah, and the Company has no cash!
Then why did the bottom fall out?
from another board
Total BETonMACE population (~2400 patients): Narrow miss on hitting the primary 3-point MACE endpoint: 18% Hazard Reduction (95% CI; 0.65-1.04) p=0.11. When excluding undetermined cause of death, there is a 21% Hazard Reduction (95% CI; 0.62-1.01) p=0.06. There was an early and sustained separation of the Kaplan-Meier survival curves. Breaking down the 3-point MACE composite, there was a 20% reduction in non-fatal MI (p=0.15) and 19% reduction in cardiovascular death (p=0.29). Forest plots show a trending improvements in hazard ratios for 11 out of 12 of pre-specified endpoints (no effect on stroke). Anticipated 7.5% 3-point MACE events per year in placebo, observed placebo rate was 5.8% per year (5.8 events per 100 patient years).
Congestive Heart Failure (CHF) in Total Population: In the total population, there was a 41% reduction for first hospitalization for CHF (95% CI; 0.38-0.94) p=0.03. Also 53% reduction for first and recurrent hospitalization for CHF. If stroke was replaced with first hospitalization for CHF in the 3-point MACE composite, there would have been a 24% reduction with p=0.02. DM mentioned that this is twice the effect of heart failure medication Entresto and that CHF market is twice that of the stroke market. An exploratory outcome composite of first hospitalization for CHF or cardiovascular death showed a 27% reduction (p=0.04). CHF partnering discussions ASAP, already initiated.
CKD population with baseline eGFR<60: In those patients with impaired renal function at baseline (eGFR<60; 124 patients apabetalone, 164 patients placebo), there was an incredible 50% Hazard Reduction in narrow 3-point MACE (95% CI; 0.26-0.96) p=0.03.
eGFR < 60 : 13/124 (10.4%) apabetalone vs. 35/164 (21.3%) placebo; HR 0.50 [95% CI (0.28 - 0.96)]
eGFR > 60: 112/1084 (10.3%) apabetalone vs. 114/1041 (11.0%) placebo; HR 0.94 (95% CI (0.73 – 1.22)]
This data is out of this world. You must view slides 21 to 29 for yourself to appreciate the robust and consistent effect on various cardiovascular outcomes in those patients with eGFR<60 compared to those with eGFR>60. It appears that the benefit is almost exclusively in those with eGFR <60 with little benefit in those with eGFR>60. All cardio data has an amplified benefit in this CKD sub-group! Renal partnering discussions planned ASAP.
Unfortunately, there was no mention of other CKD-substudy data (i.e. change in eGFR) other than the incredible MACE reduction. The only renal data shown is eGFR for the total population of ~2400 patients. At baseline, the apabetalone group had mean eGFR of 104.9 compared to 101.7 in the placebo group. At 100 weeks, the apbetalone group had mean eGFR of 104.3 compared to 105.2 in the placebo group. The data table indicates a -0.4 change in apabetalone group and a +2.1 change in placebo group, with p=0.03 for the group difference. These small changes in the total population seem clinically insignificant and in my opinion are nothing to worry about even though they are going in the wrong direction. The jury is still out on the CKD sub-study patients, who only represent ~10% of the total BETonMACE patients.
Below median LDL-C subgroup: Unexpected and yet to be understood and explained is the 40% Hazard Reduction for narrow 3-point MACE (95% CI; 0.42-0.86) p=0.02 in those with below median LDL-C at baseline. Similar to the data stratification for eGFR, it appears that most if not all of the benefit across various cardio endpoints is observed in those with below median LDL-C at baseline and little to no benefit in those with above median LDL-C at baseline. To be continued.....
Synergy with SGLT2 inhibitors: A critically important finding of apabetalone in BETonMACE is the synergy with the SGLT2 inhibitor class of diabetes drugs. ~12.3% of total patients (298 total patients; 150 apabetalone, 148 placebo) were on SGLT2 inhibitors. In this subgroup, there was a 60% Hazard Reduction in narrow 3-point MACE (95% CI; 0.16-1.00) p=0.05. Specifically in those patients taking Jardiance (Empagliflozin), there was a 66% Hazard Reduction (95% CI; 0.12-1.01) p=0.05. To put in perspective, SGLT2i by themselves in CANVAS and EMPA-REG elicited a 14% reduction in 3-point MACE. Importantly, this apabetalone effect is on top of the SGLT2i. Intellectual property has been filed, they now own IP on this moving forward. Additional patents in progress. SGLT2i partnering discussions have been initiated.
Safety: Safety is amazing. As expected, there were more patients with elevated liver enzymes in the apabetalone group; however, nothing else stands out. Amazing safety! 78/1212 apabetalone patients (6.4%) had ALT elevation of more than 3X above the upper limit of normal (ULN) compared to 18/1207 placebo patients (1.5%). Those with elevations 3X to 5X above ULN for ALT are sort of like a yellow caution flag. When specifically looking at those with greater elevations (>5X ULN), there were 40/1212 (3.3%) apabetalone patients compared to 9/1207 (0.9%) placebo patients. This rate is low and only 2.6% greater than placebo. Importanty, there was no Hy’s law cases reported indicated no liver damage. Lastly, only 35/1212 (2.9%) apabetalone patients had to discontinue due to liver enzyme elevations compared to 11/1207 (0.9%) of placebo patients. Overall, very good safety profile consistent with previous Phase 2 observations.
Cognition sub-study data: Under embargo and coming at CTAD Dec 5th. Will do webcast and update after this conference.
Near term commercialization steps: Breakthrough therapy status filings, both FDA and EMA, over the next 90-120 days. SGLT2i partnering discussions, one has already been initiated, key patent already filed. Renal partnering discussions ASAP. Congestive Heart Failure partnering discussions ASAP, already initiated. Orphan partnering discussions initially focused on PAH and HIV only at this time. PAH enrollment has already commenced. HIV funding being derived from a yet to be named US based organization.
hsCRP, apo-AI, triglyerides and other secondary endpoints: BETonMACE hsCRP data shown was only on a subset of patients at baseline and at 52 weeks. In this subset, there was no difference between placebo and apabetalone values at baseline or at 52 weeks. There was also no apo-AI data shown for baseline or on treatment. The lack of complete hsCRP data or any apo-AI data is very surprising to me. Baseline triglyceride values are shown (no difference between placebo and apabetalone); however, no on treatment triglyceride values are shown. I elaborated on these observations here. Additionally, there are some other secondary and exploratory endpoints mentioned in past trial design posters or publications that haven't been presented yet including fibrinogen, neutrophil to leukocyte ratio (NLR), platelet numbers, inflammatory cytokines, RNA profile in leukocytes. To be continued.....
Alkaline Phosphatase: In BETonMACE, AP went from 83.3 at baseline to 77.6 at 100 weeks in the apabetalone group (-4.8) compared to 81.9 at baseline to 84.2 at 100 weeks (+2.2) in the placebo group (p=0.003 apabetalone vs. placebo). Very interesting alkaline phosphatase (AP) story. They also presented a poster on AP today at AHA (see here) that is very similar to the poster at ASN earlier this month (see here). There were two other AP ASN posters too (see here and here). There is an interesting inter-relationship amongst AP, renal function, cognition, and cardiovascular disease. AP may end up being an incredibly useful biomarker. More on apabetalone and alkaline phosphatase here. Also, a new article recently came out Current Opinion in Nephrology and Hypertension from Resverlogix and members of the renal clinical advisory board: Pharmacologic epigenetic modulators of alkaline phosphatase in chronic kidney disease. AP is a hot topic!
That's all from me. Exciting stuff!
BDAZ
My concern is that there will need to be further phase three studies on the secondary end points. Listened to the archived October 31 presentation. Appears that a lot of promising information is to be presented at the AHA meeting with no FDA approval.
I fully expect all remaining data on endpoints to be released at AHA.
NR, so are you all out of RVX,... ?
Even after DM mentioned Data, Data, Data, and urged us all to wait for the AHA.
Why should any of the rumors be true? One explanation for the lack of urgency to release results is that the results aren’t good and they are looking for spin
Shorting onto news?
My concern with the dramatic drop in pps for rvx is that someone with knowledge of the announcement on October 31 knows it's not going to be good.
I'm worried that there is going to be a reverse split or another phase three study.
Anyone have any ideas why the shares are collapsing?
I am more looking forward to hearing about the two sub group's results,.. CD and CKD,.. both huge markets.
Thanks
arfxf
All the rumors of "just missed it" and wait until you see the Crestor subgroup, etc...are JUST THAT! Rumors.
NR,
While we are waiting for more Data from RVX,... any other interesting plays out there,...?
And the FDA did agree to the protocol. Look back about 3 years. This is why the stock isn’t at 5 cents. Of course there is no guarantee BetOnMace met any endpoints. More will be revealed.
Don't know what the protocol was for what you are saying but the FDA generally wants specific protocols already agreed upon before they will grant an indication.
I guess we'll all know on October 30.
not making any big bets on it, but that is the theory....
Hope you are right
Not necessarily as it is one of the pre-defined sub-group analyses in BetOnMace.
Would require a stage three clinical trial before FDA approval for combination therapy.
May work better with Crestor than Lipitor. That was the indication based on earlier trials.
Maybe to discuss the potential for this compound. Maybe to discuss the potential for combination therapy.
The 64k question is, why would AHA put the company on the agenda knowing they failed to meet primary end point. Believe me they knew. Facts are embargoed until then. The company has something positive to say. Whether it moves the pps substantially is the other question.
OTOH, there is much more information to come out. AHA in November and others
The facts are easy. It missed its primary endpoint. The balance sheet shoes little cash.
What facts and rumors?
Endpoint not met. Very little cash. Facts. Rumors abound
Why coming back so strong? Thought that the primary endpoints were not met. Thought that someone said that rvx has no money.
Fun times. Almost halfway back
|
Followers
|
21
|
Posters
|
|
|
Posts (Today)
|
0
|
Posts (Total)
|
1085
|
|
Created
|
10/12/12
|
Type
|
Free
|
| Moderators | |||

 |  |
 |  |
 |  |
The most abundant protein in HDL is ApoA-I and it serves as the building block for high-density lipoprotein (HDL or the "good cholesterol") particles. Increased production of ApoA-I protein will result in the synthesis of new HDL particles. These newly synthesized HDL particles are more' functional' because of their ample capacity to remove cholesterol from atherosclerotic plaques. The efflux of cholesterol from the plaque to HDL is called reverse cholesterol transport (RCT). The goal of enhanced RCT with newly synthesized HDL is to remove cholesterol from plaque in the arteries, subsequently regressing atherosclerosis. ApoA-I production therapeutics are the only technologies to date to efficiently remove and regress atherosclerotic plaque in high risk CVD patients.
Reverse cholesterol transport (RCT) is the natural process within the body that describes how HDL removes cholesterol from atherosclerotic plaques found in the wall of arteries. Cholesterol removed from the plaque is transported on the HDL particle to the liver for excretion from the body in the bile. Newly synthesized HDL particles are flat and empty and thus have the most function in mediating RCT.
RVX-208 is a first-in-class, small molecule that inhibits BET bromodomains. It is currently being evaluated in a phase 2b clinical trial for its ability to reverse and/or stabilize atherosclerotic disease. RVX-208 acts to increase the production of ApoA-I protein which in turn is used to make new high-density lipoprotein (HDL) particles. These functional HDL particles are flat and empty and can efficiently remove plaque via reverse cholesterol transport (RCT), the natural process through which atherosclerotic plaque is transported out of the arteries and removed from the body by the liver.

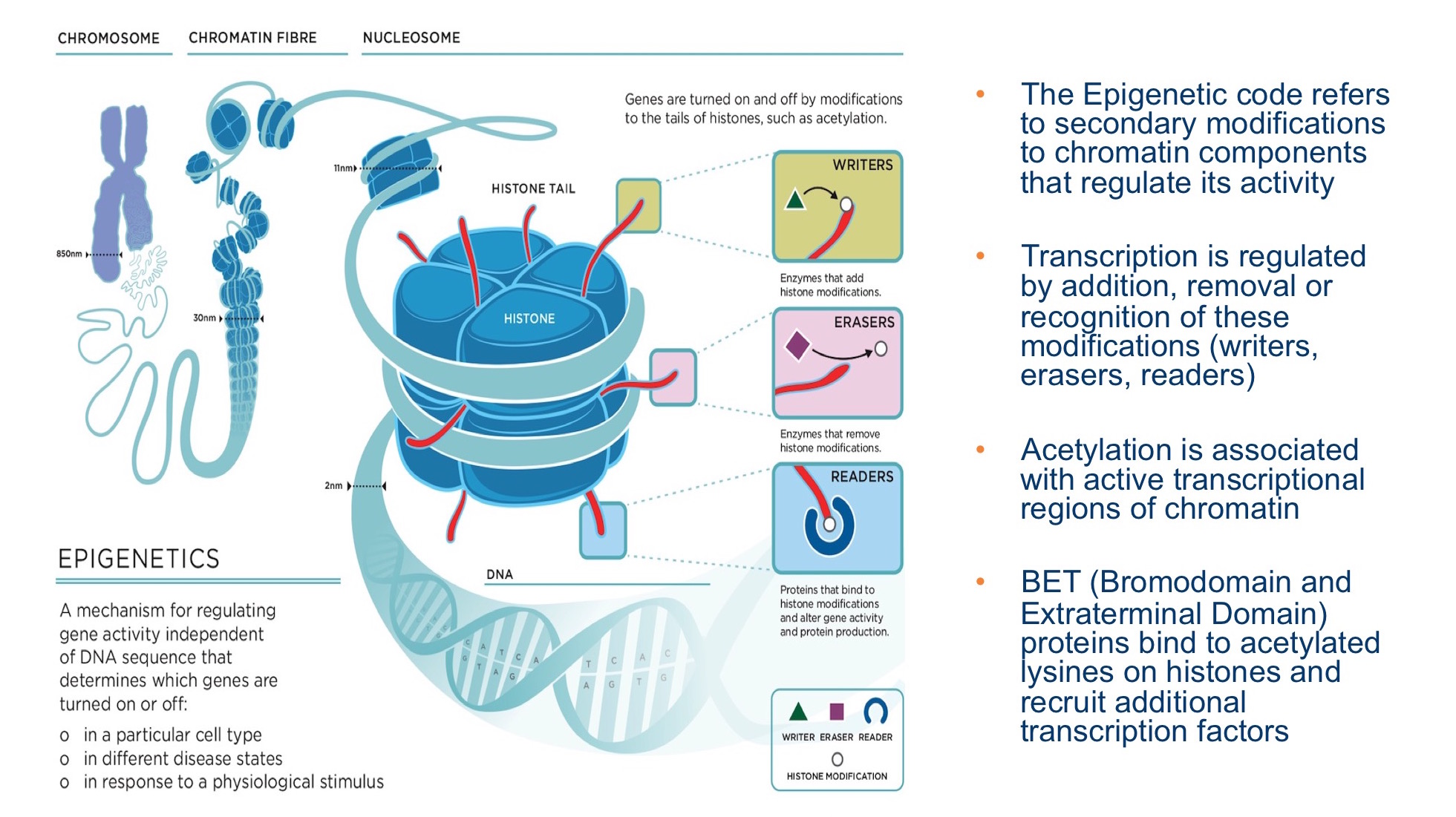
RVX-208 acts via an epigenetic mechanism leading to enhanced activity of the ApoA-I gene resulting in increased production of the protein. RVX-208 works by binding to a target called a BET protein. Within the BET protein there are two specialized regions known as bromodomains. Each bromodomain can recognize and bind to an acetylated lysine. This modified amino acid is found in histones bound to DNA. When a BET protein, through the actions of a bromodomain, finds an acetylated lysine and binds to it, this epigenetic process is called 'reading'. When RVX-208 binds to the BET protein, it triggers a cascade of events leading to increased ApoA-I gene transcription and eventually production of the protein. RVX-208 is the first in this class of compounds to enter into clinical development. Clinical experience with RVX-208 demonstrates that BET inhibitors can be both safe and efficacious when given chronically.
RVX-208 has successfully completed a Phase 2b clinical trial 'SUSTAIN' and a second Phase 2b trial 'ASSURE' is ongoing.

In this Phase 2b clinical trial of 176 patients with established atherosclerotic CVD, RVX-208 significantly increased HDL-C, the primary endpoint. SUSTAIN also successfully met secondary endpoints, showed increases in levels of Apo-AI and large HDL particles, both believed to be important factors in enhancing reverse cholesterol transport activity. The SUSTAIN trial also showed that RVX-208 was safe when given daily for 6 months and increases in alanine aminotransferase (ALT) reported in previous trials were infrequent and transient with no new increases observed beyond week 12 of the 24-week trial.
ASSURE is a Phase 2b clinical trial that will evaluate the ability of RVX-208, to regress atherosclerotic disease versus placebo using intravascular ultrasound (IVUS) technology in patients with high-risk CVD. ASSURE is a 26-week, multi-center, double-blind, randomized, parallel group, placebo-controlled clinical trial. The primary trial endpoint will be the change in percent atheroma volume from baseline to 26 weeks measured by IVUS. Secondary objectives for ASSURE are evaluating the safety and tolerability of RVX-208 and effects of RVX-208 on HDL and non-HDL lipid parameters. IVUS technology will also be used to evaluate the changes in plaque stability, an important factor affecting risk of myocardial infarction. Over 310 patients have been enrolled of which 25% will receive placebo and 75% given 100 mg of RVX-208 twice daily.
ASSURE enrollment was completed September 2012. Data is expected in the first half of 2013.
All clinical trials are led by the Cleveland Clinic.
Following the phase 2b program, phase 3 clinical outcomes trials are planned. They will encompass high risk patients with coronary artery disease and with low baseline HDL. In addition, these patients will have at least one more risk factor such as diabetes, smoking or high blood pressure. These trials are often designed with a certain number of events to be observed such as cardiovascular death, non-fatal myocardial infarction, stroke or re-vascularization.
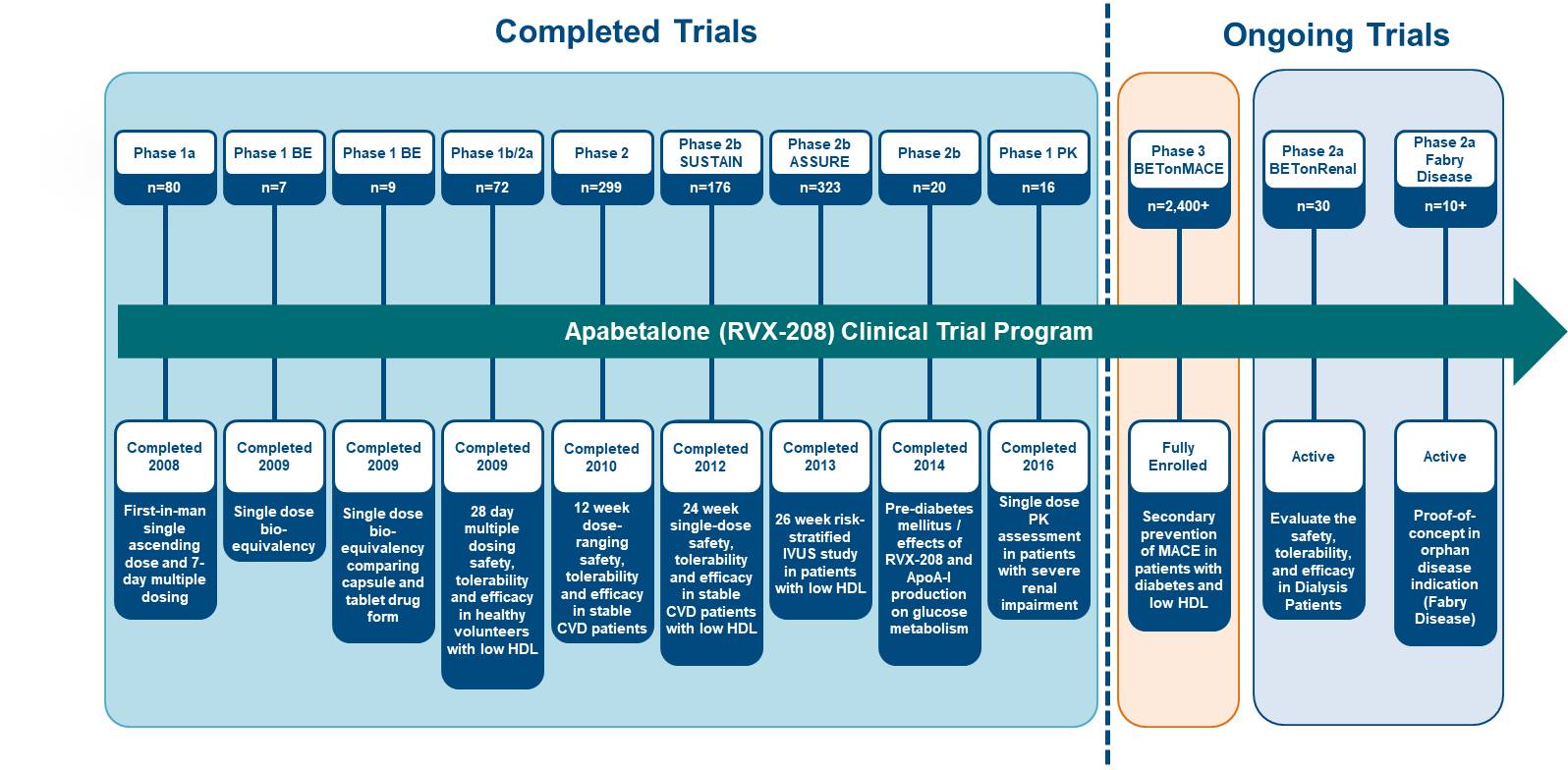
Apabetalone (RVX-208) is a first-in-class small molecule that inhibits BET bromodomain proteins. The Phase 3 clinical trial BETonMACE is advancing with a primary endpoint of time to first occurrence of Major Adverse Cardiac Events (MACE) in high-risk cardiovascular disease (CVD) patients with type 2 diabetes mellitus and low high-density lipoprotein (HDL).
| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |



