 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.


Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Sunday, October 02, 2022 8:22:29 AM
Post#
518386
of 518439
LP controls Aracaris limited, toucan, and Advent, who better to guide us through the maze.
https://www.dnb.com/business-directory/company-profiles.aracaris_limited.72a0e054c6154ef4449c5cdabe679c0a.html
https://opengovuk.com/company/08717711
The more they dilute us at this price, it becomes evident that the management themselves are not confident in any near term catalysts moving our market value and share price in an upwards trajectory. Otherwise they wouldn’t be diluting us at these levels except to keep the lights on.
Forget about buyout or partnership in the near term!
Let’s see how much more they dilute us in the coming weeks.
Unreasonable? Even with $500k Davis at the helm? Makes it difficult to follow the money. How many projects are externalized?
Research and development:
Discovery and preclinical research and development expenses include costs for substantial external scientific personnel, technical and regulatory advisers, and others, costs of laboratory supplies used in our internal research and development projects, travel, regulatory compliance, and expenditures for preclinical and clinical trial operation and management when we are actively engaged in clinical trials.
Because we are a pre-revenue company, we do not allocate research and development costs on a project basis. We adopted this policy, in part, due to the unreasonable cost burden associated with accounting at such a level of detail and our limited number of financial and personnel resources.
Market doesn’t lie!
It's not the price now, but what it will become. The literal definition of investing.
This is one of the few times I’m having serious doubts, not so much about DC Vax per se, but about LP’s ability to execute a business plan within any meaningful length of time. Time equals dilution and uncertainty. And LP has placed common shareholders in a bad spot.
Given the length of time with no guidance or updates from management, added with the odd deployment of the Donut Eaters at LP’s Evil Georgetown Digital Media Company; and now this promotion of Hefner for some strange reason, this all ‘n all looks suspiciously like diversion and deflection. And gives a particular penny stock feel to everything.
We’re in flip’n October!
This is a poor attempt to claim I am short by association with a person I do not follow.
I am long. Why sell Cs here and when did they start negotiating for the Cs. I know you do not have the answer.
The Danish Dude
Re: None
Sunday, October 02, 2022 5:53:24 AM
Post#
518358
of 518432
I have compiled a "what has happened in 2022" guide or in other terms "Let's pump it" for those who haven't heard of the phenomenons of reason, rationality, logic, that makes it possible to put forth information and thesis that are qualified with regards to being either uncompromising facts, or very probable.
Let's take a stroll down the 2022 memory lane and sum up, why the NWBO stock currently is the best stock investment since Gamestop around new years eve 2020, at this ridicolous price level.
Facts
January 9th.
The use of the external control arms trial design gets thumbs up by FDA, as the article "External Control Arms in Oncology: Current Use and Future Directions", gets printed in Annals of Oncology. 12 co-authors, among these dr. Richard Pazdur, ALL affiliated with U.S. Food and Drug Administration, also known as FDA.
January 11th.
AdventBio announces their new Cryostore and Freezer facility at Sawston.
January 23rd.
It is found out, that dr. Roger Stupp, the man behind The Stupp protocol, which became standard of care for the treatment of glioblastoma (GBM) since its publication in 2005, became an advisor to NWBO BEFORE September 26th. 2020.
January 27th, February 17 and 26th.
3 articles in british newspapers specifying the NWBO and AdventBio connection, with the later dedicated to do NWBO's bidding as a CDMO in terms of manufactoring and production.
When reading, one is not in doubt of the "mother-child" setup and what is AdventBio's main purpose.
"Northwest Biotherapeutics has secured MHRA certification for its cancer vaccine trials in the Sawston Business Park, sparking delight for site developer Advent BioServices. Advent, which is based on the Park, has completed the laboratory facilities to UK regulatory standards on behalf of Northwest Biotherapeutics, which is headquartered in Bethesda, Maryland. NW Bio’s Sawston R&D team is working on a cancer vaccine for glioblastoma multiforme, the most aggressive type of brain cancer."
Article reveals that AdventBio are now 40 employees. Most hired within a year.
February 6th.
A Global Glioblastoma Multiforme Drug Forecast and Market Analysis expect DCvax-L to be one of three pipeline agents to have highest sales in the GBM market till 2030.
February 17th.
Advent Bioservices – NW Bio’s contract manufacturer in the UK – has been conducting the required post-approval re-validations and testing so that the facility is now ready for the manufacture of cell therapy products for clinical use.
The first vaccine production for compassionate use treatment is for a glioblastoma patient.
March 2nd.
Dr. Marnix Bosch speaks at the Brain Tumour North West Retreat, a yearly cancer symposium, which is attended by british gbm clinicians. It seems he gets registered late for a 2 hours session, where he is to speak of “Dendritic Vaccine”.
The news is not in any way published. A participant tries to delete his tweet revealing this and blocking anyone writing about it. In vain.
March 31st. 2022
Linda Liau speaks about “Therapy induced resistance in glioblastoma” at University of Miami. She talks about the UCLA Spore 1 project, which directly mentions the use of DCVax-L in conjunction with PD-1 inhibitors.
She also talks about the combo trial that started in 2010, that has run for 12 years, combo'ed with Resquimod and nt least Poly-ICLC:
"That’s actually another project, we’re working on getting collaboration with Mark Gilbert and NCI. We’re actually trying to collect all these people, because even in our immunotherapy trials, I think we have about 50 of them now, that are over 5 years going on 10 years"
“The group that got dendritic cell vaccination plus poly-ICLC had a 50% survival rate and now the majority of these patients are reaching 100 months and with not only survival but really no tumor recurrence.”
May.
Dr. Linda Liau is in the UK.
May 10th.
Results of the P3 DCvax-L trial is presented at NYAS. All endpoints met, statistic significance. Landmark results, the best seen in 3 decades.
June 5th.
Northwest Biotherapeutics Announces Presentations On DCVax®-L Personalized Vaccines, Manufacturing and Scale-Up, and DCVax®-L Clinical Program. They are now able to scale to 1.000 patients pr. month. 12.000 pr. year.
June 6th.
Professor Keyoumars Ashkan from Kings Hospital in London presents P3 DCvax-L results in a video.
June 8th.
Hugh Adams, Head of Stakeholders Releations from the british Brain Tumour Research organisation writes the following in an email:
"Thank you for your email, your information and your advice. We communicate directly with Linda Powers at NWBio and most recently facilitated her contributing to a meeting with UK politicians as part of an inquiry into the pathway to a cure for brain tumour patients."
May 16th.
NWBO submits annual OTCQB certification Michael Fox (new) and Sarah MacLeod (known) have been added as IR/PR service providers.
About Michael Fox:
With more than 25 years of experience in strategic communications at global PR agencies and in politics, Michael has advised leading global companies, promising start-ups, respected organizations and political candidates across the full range of communications, media and reputation management activities. He leads the Corporate Communications Group at ICR and specializes in corporate positioning, executive coaching, crisis, transactions and special situations.
Michael has provided communications counsel on more than 100 IPOs, scores of M&A transactions.
June 23rd.
Professor Keyoumars Ashkan yet again presents the P3 DCVax-L trial results at BNOS in Liverpool in England. At the presentation is Linda Powers CEO of NWBO. Mike Scott CEO of Advent Bioservices. Dr. Roger Stupp creator of the chemotherapy Standard-of-Care and now advisor to NWBO and Hugh Adams, the Head of Stakehold relations at british Brain Tumour Research organisation
July 1st.
Dr. Linda Liau presented the DCVax-L Phase III trial results in Prague, at The Society of University Neurosurgeons 2022 Annual Meeting.
July 6th.
Northwest Biotherapeutics Announces Filing of Application for License for Commercial Manufacturing at Sawston, UK Facility
August 17th.
Northwest Biotherapeutics receives final Approval of Pediatric Investigation Plan (PIP) by MHRA, green lighting the use of OS endpoint and external control arm trial design in the P3 Adult trial.
September 30th.
Advent Bioservices continues to hire and have now more than 60 employees. Their latest job roles includes a GMP Production Scientist in London, with the following job description (excerpt).
"The GMP Production Scientist will be responsible for performing batch manufacturing of the company’s contract manufacturing products to support the delivery, in the first instance, of Advanced Therapeutic Medicinal Products (ATMPs) as both ”Specials” and as Investigational Medicinal Products (IMPs). The post holder will work closely with GMP Production Scientists, Quality Assurance Scientists and facilitate the efficient delivery of cellular therapy products for clinical use."
Correlate that with NWBO press-release from 21st. December 2021, when they announced MHRA Approval Of License for GMP Manufacturing At Sawston, UK Facility and you can not miss how AdventBio are continually hiring people that fullfill NWBO's future plans.
"The MHRA license approval enables the manufacturing of DCVax-L products to get under way at the Sawston facility in addition to continuing at the smaller GMP facility in London. The license also permits the import and GMP manufacture of other cell therapy products under the UK’s supply of unlicensed medicinal products (‘Specials’) regime and for clinical trials under the Investigational Medicinal Products (IMP) Programme."
It's only to congratulate those diamond hands, that wonders what the talk about the management not doing their shareholders bidding is all about, who are patiently awaiting the inevitable and who use the extra time to continue to load up.
abeta
Member Level
Re: None
Saturday, October 01, 2022 5:51:55 PM
Post#
518324
of 518431
Sept 30 2022 - Glioblastoma recurrence reveals novel and targetable immunoregulatory drivers
NOTE: p means Primary
We, therefore, quantified the transcriptome and proteome of 134 patient-derived pGBM and rGBM samples, including 40 matched pGBM-rGBM pairs.
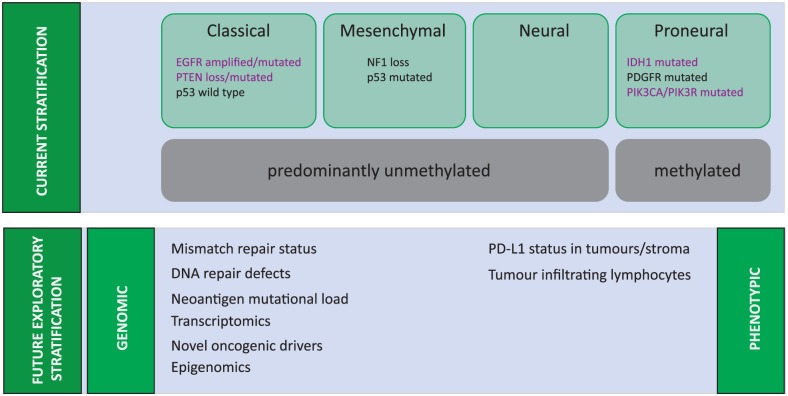
GBM subtypes transition from pGBM to rGBM towards a preferentially mesenchymal state at recurrence, consistent with the increasingly invasive nature of rGBM.
We identified immune regulatory/suppressive genes as important drivers of rGBM and in particular 2-5-oligoadenylate synthase 2 (OAS2) as an essential gene in recurrent disease.
Our data identify a new class of therapeutic targets that emerge from the adaptive response of pGBM to therapy, emerging specifically in recurrent disease and may provide new therapeutic opportunities absent at pGBM diagnosis.
https://pubmed.ncbi.nlm.nih.gov/36178522/
note - the above is the abstract and I don't know how to get to the whole article
other than paying about $40 bucks
Sidebar
2',5'-oligoadenylate synthase (OAS) is a class of enzymes induced by interferons and mainly encoded by the OAS1, OAS2, and OAS3 genes, which activate the potential RNA enzymes to degrade viral mRNA, inhibit viral protein synthesis and promote apoptosis in virus-infected cells. OAS3 is associated with breast cancer prognosis. However, the expression and prognosis of OAS3 and tumour-infiltrating lymphocytes in pan-cancer remain unknown. In the present study, we have systematically investigated and confirmed the role of OAS3 in tumour immune infiltration, immune escape, tumour progression, response to treatment, and prognosis of different cancer types using various bioinformatics methods. The findings suggest that OAS3 is aberrantly expressed in almost all TCGA cancer types and subtypes and is associated with tumour staging, metastasis, and prognostic deterioration in different tumours. In addition, OAS3 expression is associated with the prognosis and chemotherapeutic outcomes of various cancers. In terms of immune-infiltrating levels, OAS3 expression is positively associated with the infiltration of immunosuppressive cells. These findings suggest that OAS3 is correlated with prognosis and immune-infiltrating levels.
https://pubmed.ncbi.nlm.nih.gov/35592250/
LOL, more bullshit. Let me know how one is privy to the details of his trades or if this is all nonsense. I suspect more nonsensical narratives.
have a good one mav.
Then we wouldn’t be sitting here at 70 cents. He ought to be buying shit load here if we are so under valued and good news was coming. I’d get my billionaire friends join the party too. Either he is manipulating the SP or isn’t buying. Market doesn’t lie!
This is a poor attempt to claim I am short by association with a person I do not follow.
I am long. Why sell Cs here and when did they start negotiating for the Cs. I know you do not have the answer.
RE FLASKWORKS: "For instance, consider the trial that I’ve done for dendritic cell vaccines. For cellular therapies, I think what is lacking is a smooth, operational aspect. Let’s say, if there was a company that could make GMP-grade cells readily and basically, it’s almost like the manufacturing, production, distribution, and coordination of the treatment or clinical trial for approval for a treatment would go much more smoothly.
I think that’s what’s lacking. And the ideal company would be like, almost like an Uber or Amazon. Basically something that turns and existing industry upside down. I think we need something that turns the—not only the clinical trial to FDA approval process upside down, but also how to scale that up once something is approved or adopted.
That’s also a struggle, because a lot of things we develop in academia that are interesting, like the cellular therapies, are very hard to scale up. And you could develop less interesting things like single-target molecules, but so far those haven’t really been useful for GBM."
Q&A with Linda Liau
by Bill Malloy | Mar 17, 2020 | Data, Health, Medication, Scientists, Services, Technology
interview
As Chair of UCLA’s Department of Neurosurgery and the inventor of a personalized brain cancer vaccine, Dr. Linda Liau is widely recognized as one of the world’s most forward-thinking brain surgeons. Having spent more than 25 years on glioblastoma research, Dr. Liau developed the individualized treatment to work with a patient’s unique immune system to detect and attack cancer cells that remain after tumor removal.
Glioblastoma, the most aggressive type of cancerous brain tumor, usually results in death within 15 months of diagnosis. One of the biggest problems with finding a successful treatment? According to Dr. Liau, the fact that the disease is so heterogeneous – that it presents differently from patient to patient – means that the standard clinical trial approach has so far been less than helpful when it comes to identifying a cure.
So, what is the answer? Ever the pioneer, Dr. Liau thinks that comparative analysis may be a good start. Such an approach would allow physicians to treat patients individually, using real-word data to treat the patient according to what is best for them, rather than by strictly adhering to the protocols of a standard clinical trial.
I recently sat down with Dr. Linda Liau to discuss glioblastoma, the current state of clinical trials, and how a different approach is needed to eventually find a cure.
Q: What, in your opinion, is the big-picture problem with glioblastoma?
A: I’ve been working in this area for 25 years now, and one after another, these trials fail. AbbVie had a trial just a few months ago that failed and I think biotech caption was, “Glioblastoma takes another victim.” So, I think we’re going about this the wrong way, because I think everybody’s trying to find a cure but also have a company raise money and get their company launched. But glioblastoma is such a heterogenous disease. I don’t think you could go say, “Oh, I have one drug or one treatment, one molecule target or one drug, and I am going to patent this, license it and then do a startup company. And this is how I’m going to cure GBM.”
More and more, I do think you need to think about appropriation therapies, we need to think about timing of treatments and also the whole process of getting therapies adopted through the whole hurdle of FDA approval.
For instance, consider the trial that I’ve done for dendritic cell vaccines. For cellular therapies, I think what is lacking is a smooth, operational aspect. Let’s say, if there was a company that could make GMP-grade cells readily and basically, it’s almost like the manufacturing, production, distribution, and coordination of the treatment or clinical trial for approval for a treatment would go much more smoothly.
I think that’s what’s lacking. And the ideal company would be like, almost like an Uber or Amazon. Basically something that turns and existing industry upside down. I think we need something that turns the—not only the clinical trial to FDA approval process upside down, but also how to scale that up once something is approved or adopted.
That’s also a struggle, because a lot of things we develop in academia that are interesting, like the cellular therapies, are very hard to scale up. And you could develop less interesting things like single-target molecules, but so far those haven’t really been useful for GBM.
Q: How can we use software take everything that’s out there and make the trial process more efficient?
A: Right now, we’re starting up a trial, which personally I think would be very promising. It’s basically using vaccination in combination with a PD-1 inhibitor. We’re working with Merck on that in combination with Poly ICLC, which is a Toll-like receptor. That’s another company called Oncovir.
So, with a DC vaccine, like I said, we can just make it ourselves. We can’t scale up as an academic institution or a small company, but if that were part of the company we could scale up. To make the vaccine, you just need a manufacturing GMP facility. But the problem there is the autologous dendritic cells are hard to get patented. You could patent it, but it’s hard to defend that because it’s really the patient’s own tumor, right?
So, the patents really are process patents and we could file one that tweaks things a little bit, and that’s essentially that’s what Northwest Bio did. They filed multiple patents just on little tweaks of the cocktails that are used to make the cells.
The other drugs are already made by other companies and they’re just an agreement. How do you patent something that is actually part of a patient rather than just patenting the process? And that’s why people have gone on to patent just individual targets. We could do that, but I wouldn’t invest millions of dollars on a clinical trial to do a trial of a vaccine for an individual target. I just don’t think it can work. So, I think the conflict is you could patent some—you could say, “Oh, I discovered this one protein that we can make a vaccine to and we could license it.” But my gut feeling is that is not going to be what will cure GBM. In a way, what I think will cure GBM is unpatentable. So that’s the dilemma. Does that make sense?
Q: Do you feel that that in order to find the cure, we have to flip everything upside down and approach it differently?
A: Yeah, and so the problem is because of the financials, we get approached by VC’s that want to start a company. Obviously, there’s a way of doing this, right? You think of a way of doing it. Big Pharma does the same thing. It’s like, “What’s your drug? What could we do with it?”
It’s been successful in other areas. A lot of my colleagues here have done very well with prostate cancer drugs and breast cancer drugs. But so far glioblastoma and pancreatic cancer are both very formidable, and we haven’t gotten there with these small biotechs or Big Pharma companies coming to us and saying, “What do you have?”
And we give it. We either license it out or start your own little startup. Here at Stanford, it’s a very start-up environment. It depends on your goals. If your goal is to have a startup and then have a pharmaceutical company buy you out or get an IPO, you could do that. We could do the same thing Northwest Bio, Tocagen, Selbach, or any of these companies that have already done trials do.
But at the end of the day, it doesn’t really cure GBM unless there’s something a little bit broader. I guess in my heart of hearts, I think what’s going to cure the disease is going to be personalized. It’s going to be something that comes from the person or the tumor itself and I’m not sure how that can be patented other than the idea and the process by which that’s done.
Q: Why is it so difficult to find the cause of glioblastoma? Why can’t we find the cure?
A: Yeah, I think it’s just too heterogeneous of a tumor. The cause is not one thing and it’s not the same thing for each patient. And also, not for each patient at any point in time, because the tumor also changes over time. So, you’re really looking at four-dimensional variables that are changing.
To say, “oh, I have this one treatment that’s going to be able to deal with all that,” is unrealistic. And that’s why I think ultimately at least in terms of dealing with the heterogeneity from patient to patient, you have to come up with more patient-derived or patient-informed treatment. Not something that you just take off the shelf and give to everybody.
Because I think with all these little trials that we’ve done over the years, there are some people that responded, but the majority of the patients don’t. Then the trial fails, and we really don’t learn anything about it. It just needs to be a process involving finding mathematicians or bioinformaticists who are skilled in terms of how you deal with a problem where you have moving parts in four dimensions.
Q: How much is the blood-brain barrier a part of that four-dimensional moving part? Is that one of the four dimensions in your mind as you described it or is it just another impendent into the problem?
A: Yeah, I think it’s another impendent into the problem. Delivery is certainly an issue because of the location. It’s an issue for other things as well. Even in immunotherapy, the immune response is different in the brain. I remember when I first started, people used to say that you can’t get an immune response in the brain.
I think now people think otherwise. You can, but I think it’s different than the rest of the body. It’s just not the same type of response. So that plays into it, as well as getting drugs into the blood-brain barrier. I would say all of the above.
Q: Is there anything else in that big picture that people should know or be thinking about specifically around glioblastoma?
A: Yeah, I think people have to think about the patient when we design these trials. A lot of times, we design these trials and end-points based on the way we design the mast studies. We have a treatment group and we have a placebo group. Then, at the end we’ll see which group does better.
And I don’t think in patients you can do that. And honestly, if I were a patient, I’d hop from one trial to another depending on what sounds promising or what’s available at that time. A lot of patients do that, and then you really cannot necessarily control for that. Let’s say someone took TOPA and then went on another trial. Was there any effect from the virus that they had before?
So, I think that’s an issue in terms of when we design these trials, what should we have in mind? We have the patient more in mind. And I think, broadly speaking within the field of neurosurgery and neuroscience and not just brain cancer, a lot of people are advocating for what they call comparative analysis. Not necessary using randomized clinical trials as the gold standard but using real-world data.
For instance, how would you actually treat this patient? Not how would you treat this patient based on the protocol in the clinical trial. Because a lot of times, as a physician, what we want to do is what’s best for this patient. And sometimes, it’s not necessarily congruent with the strict protocol procedures that you have to abide by to keep a patient on the clinical trial.
And then it’s hard because patients have access to information on the Internet and shop around to get different things. For instance, I must get a dozen or more emails or calls every week from random people about how they can get the dendritic cell vaccine, DCVax. And personally, I can’t—one, I can’t do that on a clinical trial. But even if it was FDA-approved, unless it’s covered by insurance how do you pay for them?
So, how do we fix that problem? All of these trials fail because the treatments don’t work, but I think a larger part is we’re not designing the trials right. But part of it is that it’s difficult to provide these trials if you truly want to do what’s best for your patient.
Q: Can you explain more about the difficulties in designing the trials to do what’s best for the patient?
A: For instance, I’ll just take what happened with the DCVax. You really want to get clean data. We’ve never allowed for patients to get the vaccine once they failed, because they will. You enrolled in the trial. You had a recurrence, and now you’ll have to try something else.
I could tell you patients are fighting to get the vaccine. And even if you tell them, “Well, there’s no proof that this works. This is the whole reason we have to do the trial. I can’t tell you that there’s any benefit.” But I guess the counterargument that I hear quite often is, “well, the side-effects aren’t bad.” And they’re not. So, it’s like, “Well, if it’s not going to hurt me why can’t I have it? Why can’t I try it?”
Because of that it’s hard to prove something based on what the FDA requirements are without being a little cold-hearted and saying, “Well, no, you’re not allowed to try that.”
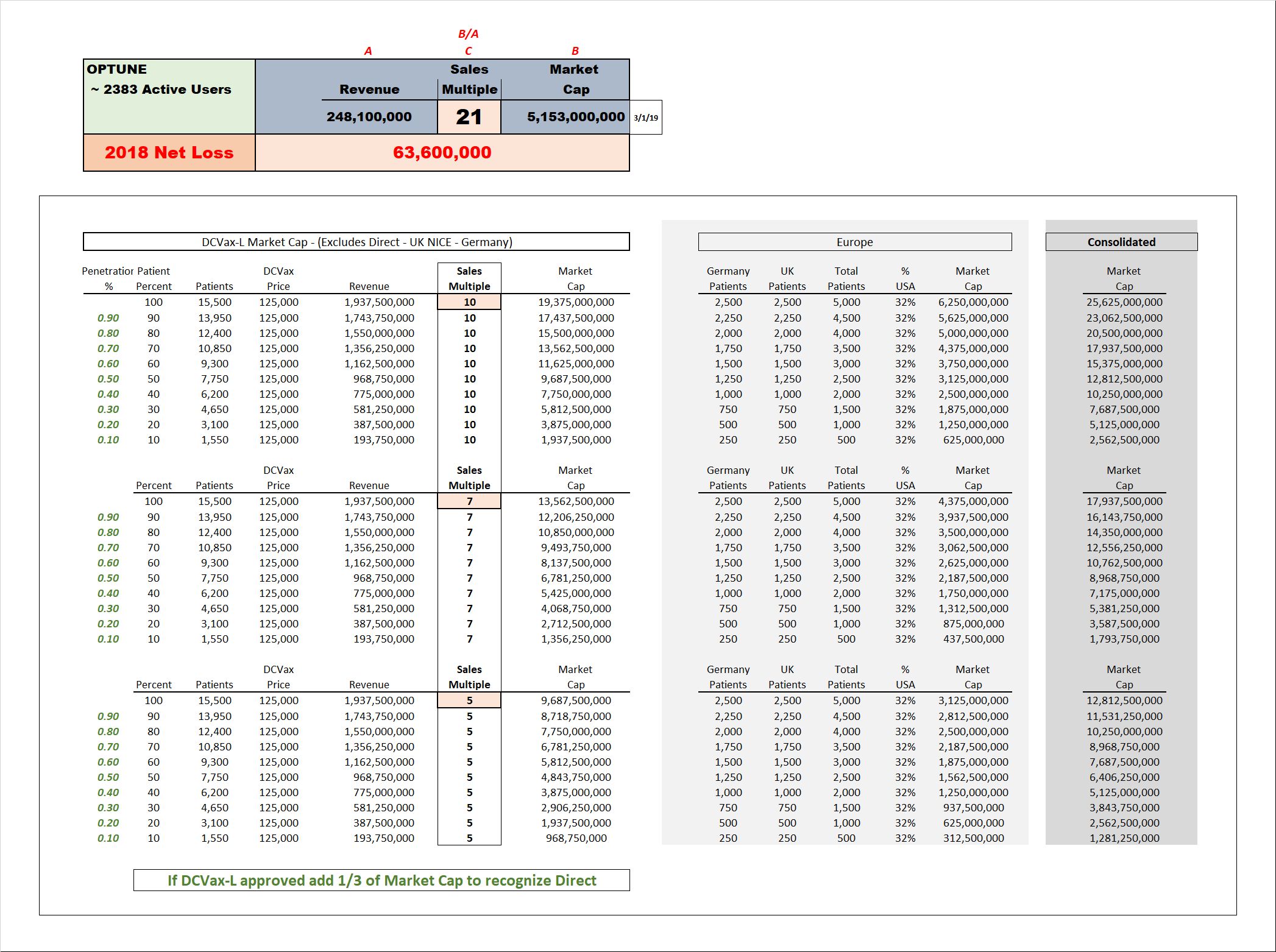
So, a part of it is having the FDA think a little bit differently about what constitutes approval. On the converse, like the Optune device, that Novocure device, is FDA-approved. But I must say a lot of patients are like, “Well, I don’t really like it.” And I think on the physician side, we just don’t understand how it works and there are a lot of problems with the clinical trial design.
There was no true placebo arm, but they did design it in a way that met the FDA checkboxes. So, it was approved, but a lot of us don’t really believe that it works. I think it’s one of these things where if your ultimate goal is to cure GBM, it’s hard to reconcile all these different factors; the regulatory factors, the financial factors, as well as the science and the biology of the tumor itself, which is very complex.
Q: Got it. Sounds like we have our work cut out for us.
A: Yeah, but if your smart people can figure this out, I think it could be done. It’s been done in other fields, but I think it just takes a different way of thinking about it, and it’s not the “Eureka!” moment of, “oh, I discovered something in the lab. I’m going to take it to clinical trial, launch my startup company, and charge ABM.”
David, I think you may be reading my analysis incorrectly. Can you quote where I’m saying we have already had the golden cross? The golden Cross happened on the 4 hour chart earlier this week.
I did give the bonus tip referencing the long term MACD setting of 65, 90, 12. I was stating that when that MacD crosses the centerline that very closely correlates to win the 50 will get above the 200. We are not there yet and I was forecasting there’s a possibility happens in October but more likely in November if we continue this trajectory
Most can tolerate at it. After ten years of promises made and not kept, it my right to point out their faults. I stayed silent a long time. The clown show roll out and share collapse was it for me. If it continues, others will join in.
It is the way of the world. People pick who to blame for inflation. I can do it with a stock I own.
jammy32,
Those who can not tolerate waiting out “the process” aka “the gauntlet” will be a victim of it whether a patient or an investor. I’m more concerned about how many patients have been sacrificed by “the process” than how many investors have been. Still, I am here to encourage and pray for both as many investors in this company have ulterior reasons due to cancer, and those opposed to providing a cure because of economic impact, making this fight personal. Best wishes.
Agree wholeheartedly CO. Eloquently stated.
But 70 cents a share is factual. Can we agree on this? Why would this big breakthrough that seems well documented be sitting at 70 cents. Something seems odd.
My dream came true target is 100 baggers extrooper. But I don’t mind if it could reach your target price which to me like 250 folds. :) :) I read a very old book written in 1974 by Thomas Phelps on 100 to 1, the concept is very simple. Sometime it is too simple. I think it is not outside the realms of every investor. Phelps said “Buy right and hold on”.
I learned something from Phelps that Patience is part of the key recipe in investing. I am practicing it now and hopefully I can be patient enough. I know it is not easy. It was difficult for investors in the 1930s, 1940s. It is still difficult now.
It's just another way of saying the same thing but in a funny context. Get out of the oven why would you be in an oven? It's funny at least to me. This is the way nwbo has been for the last 10 years at least because that's how long I've been around. Nothing changes nothing changes why would they start to do things differently now? Not to say that they shouldn't but to expect something different from someone who's done something the same way for years and years and years it's not looking at things realistically.
I didn’t get it and still do not. Sorry. Just looking for accountability. The only excuse for no ASM is talks with partners or buyout. Otherwise they have not been accountable. Also lack of quarterly calls is a lack of accountability. The BOD needs to perform or give the seats to people that can.
Nonsense. first, how do you know how much he has already invested? second, how do you know he isn't investing further?
LOL, why isn’t he investing more if it was so obvious and close? It’s all a game.
Billionaire Robert Hefner, the father of natural gas, knows your arguments are nothing but hot air!
Our Northwest Biotherapeutics (NWBO) investee “partner” likely has just made one of the biggest breakthroughs in the history of cancer. We know that is a really big statement so why do we at GHK believe that is possible? Because we believe the doors through which major cancer breakthroughs must pass are the human immune system, immunotherapies and personalized vaccines and NWBO has just leaped through those doors with its personalized DCVax vaccine made from your own cells.
You can argue about trial statistics until the cows come home but the bottom line is 1) people living longer 2) quality of life during treatments and 3) the cost of treatments.
During NWBO’s 16-year Phase III trial to treat glioblastoma (GBM), one of the most difficult and lethal of all solid tumor cancers 1) more people lived longer, 2) it is safe with virtually no side effects occurring and 3) NWBO estimates treatments will cost about half as much as Standard of Care chemotherapy and radiation treatments. So for the first time ever, GBM patients can have hope! And can hope like prayer increase the effectiveness and energy of the immune system? We think so.
We are aware we stuck our necks out when we said “possibly one of the biggest breakthroughs in the history of cancer”. So we have listed below our three principle reasons so you can decide for yourself:
After 417 failed GBM trials treating 31,952 patents over decades, DCVax-L is first treatment that gives GBM patients a meaningful chance to live longer, some now living 9 to as many as 19 years and counting.
DCVax was conceived and created not for glioblastoma alone but as a personalized tool of your own immune system to defeat all solid tumor cancers and that’s 90% of all cancers.
Since DCVax’s creation NWBO has amassed an enormous rich databank containing masses of information on patients, treatments, and DCVax’s use against 15 different solid tumor cancers that has not yet been analyzed by artificial intelligence (AI). We believe that in the near future when these vast amounts of data and information are teamed with AI and some of the world’s leading scientists and doctors that future generations of DCVax vaccines and protocols will experience great leaps forward in effectiveness at lower and lower costs for 90% of all cancers.
So to sum up, we believe NWBO with its DCVax immunotherapy personalized vaccines has leaped through the doors and will play a vital role in humanities great drive to defeat cancer once and for all.
Dr. Ashkan is the genius behind this viral vid of him performing brain surgery while his patient was awakened to play the violin…mid-surgery. He told me he champions DCVax-L bc of trial data along with what he’s seen first-hand from his patients. $NWBOhttps://t.co/XFTeSPFtH5
— Wade Kovash (@wkovash) June 6, 2022
Watch one of the world’s preeminent neurosurgeons explain the significance of $NWBO ‘s Phase III trial of DCVax-L. The results are groundbreaking and represent an enormous advancement in one of the most tragic cancers. https://t.co/eQw5tAsivK
— Wade Kovash (@wkovash) June 6, 2022

My posts in no way suggest anyone should sell. I am just stating there may be other reasons for a 70 cent share price other than shorts. As a shareholder have the right to complain as to how management has managed the company.
Science and truth makes people invest in NWBO. Ignorance leads to sellers, day traders and shorts .
I’m up 350% and refuse to sell until I hit 8000% , which could be any day.
Excellent. Sharing this.
For me, time to look elsewhere
I do not fault you for that.
The short narrative is wearing thin except for a very few. For me, time to look elsewhere. I sure haven’t bought into it for some time. Good luck converting people with the mantra.
stumble? bullshit. the 400+ failed trials stumbled. nwbo is on the verge of RA approvals. This is only a stumble for the short narrative.
I’d be happy with 10 bucks.
From my posts this morning you know I am not all sunshine and rainbows but I can easily come up with an over $100 per share price. As a platform for all cancer operable and inoperable you could get a million patients a year. You can do the math at $200K a pop.
But that dream keeps fading as I watch management stumble.
Aracaris limited is a whole owned subsidiary of NWBO. She might sign the papers but NWBO owns it along with the 13 acres in Sawston.
Losing money in stocks like NorthWest is not surprising
I got sucked into a hope and prayer stock
Yes, a federal court judge agrees with you. These bullshit negative narratives are only found online in fantasy land. Reality is a different story.
Have a great one HL.
Thanks Hspooner. I will take a look at your past posts for the companies working with Advent.
Photoshopping halos on to this management team does not make them Angels or Saints but they are lawyers which means that what they are doing is legal.
LP controls Aracaris limited, toucan, and Advent, who better to guide us through the maze.
https://www.dnb.com/business-directory/company-profiles.aracaris_limited.72a0e054c6154ef4449c5cdabe679c0a.html
https://opengovuk.com/company/08717711
LP is the managing partner of Toucan which owns Advent. LP is most likely one of many owners of Toucan. I think it is clear LP owns some percentage of Toucan but the exact ownership interests, no one knows. all imo
Linda powers owns advent, and established it as a UK company, I believe because the MHRA requires that a company be based in the UK for licensing purposes. I also believe the other companies they are contracting with are connect to LP, I posted the connections in the past if you want to dig through my old posts.
it takes 2 to tango. LP won't sell cheap. She also doesn't give up despite the years of false bullshit attacks and baseless lawsuits. LP and nwbo will have the last laugh.
I disagree with this false price ceiling. If I were short I'd be setting these sort of fake price ceilings.
SNO 2022 could be a bust for investors like NYAS and it will be if NWBO does not learn anything about effective public and investor communications and fixed lifelong bad habits in a handful of months is unlikely.
The last few months have proven to put charge in that spreading awareness among scientists has little impact for shareholders.
Furthermore SNO 2022 could well be another placeholder as we all learned the hard way back in 2020.
If something happens, great but slapping a bunch of logos up there does not counterbalance the historical cycle of hype and crushing disappointment here.
I'd agree with this nonsense narrative if I were a short. I'm long so I disagree.
have a great one HL!
Chris Brown and his hedge fund which is shorting nwbo would agree with this bullshit narrative!
LOL at this bullshit short narrative. I couldn't read past the first sentence.
have a good one Mav
|
Followers
|
1638
|
Posters
|
|
|
Posts (Today)
|
203
|
Posts (Total)
|
722837
|
|
Created
|
02/02/05
|
Type
|
Free
|
| Moderators flipper44 sentiment_stocks CaptainObvious Poor Man - Doc logic JerryCampbell | |||
![]()
“Now this is not the end. It is not even the beginning of the end. But it is, perhaps, the end of the beginning.”
~ Winston Churchill

Stylized Dendritic Cell featured on NWBO board since 2015

- Dr. Linda Liau, PhD, MBA, Professor and Chair, Department of Neurosurgery, David Geffen School of Medicine at UCLA
Clinical Trials
DCVax®-L to Treat Newly Diagnosed GBM Brain Cancer (NCT00045968) - Phase III (Double Blind)
UK (MHRA): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
DE (Germany - PEI): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
Expanded Access Protocol for GBM Patients with Already Manufactured DCVax®-L Who Have Screen-Failed Protocol 020221 (NCT02146066) (Expanded Access)
Safety and Efficacy Study of DCVax-Direct in Solid Tumors (NCT01882946) - Phase I/Phase II (Open Label)
UK Clinical Trials - Study of a Drug (DCVax®-L) to Treat Newly Diagnosed GBM Brain Cancer
EU Clinical Trials for DCVax-L - Phase III
Dendritic Cell Vaccine for Patients with Brain Tumors (NCT01204684) - Phase II - at UCLA - Randomized (Open Label) testing DCVaccine with Resiquimod and DC Vaccination with Adjuvant polyICLC
Pembrolizumab and a Vaccine (ATL-DC) for the treatment of Surgically Accessible Recurrent Glioblastoma - Phase 1 (NCT04201873)
Dendritic Cell-Autologous Lung Tumor Vaccine (DCVax-L) and Nivolumab in Treating Patients with Recurrent Glioblastoma - Phase 2 (NCT03014804)
Dendritic Cell Therapy for Brain Metastases From Breast or Lung Cancer (NCT0368765) - Phase 1 - Collaborator: Mayo Clinic
Announcement of DCVax-L and Anti-PD-1 Monoclonal Antibody (Pembrolizumab) for Patients with Liver Metastases of Primary Colorectal Carcinoma Phase 2 Trial - November 17, 2016 - University Medical Center (UMC) of the Johannes Gutenberg University of Mainz
Cognate Bioservices - Owned by Charles River Labs
Website
Company Contact Info
Investor Relations:
Les Goldman (Company) (202) 841-7909 lgoldman@nwbio.com
Sign up for Northwest email list here (hit the subscribe to email list button in the lower right)
Company Headquarters
4800 Montgomery Lane, Suite 800, Bethesda, MD 20814 (240) 497-9024
NW Bio is developing cancer vaccines designed to treat a broad range of solid tumor cancers more effectively than current treatments, and without the side effects of chemotherapy drugs. NW Bio’s proprietary manufacturing technology enables them to produce its personalized vaccine in an efficient, cost-effective manner. NW Bio has a broad platform technology for DCVax dendritic cell-based vaccines.
Their lead product, DCVax-L, is currently in a 331-patient Phase III trial for patients with newly diagnosed Glioblastoma multiforme (GBM), the most aggressive and lethal brain cancer. This trial is currently underway at 69 locations thoughout the United States, Germany and the United Kingdom. NW Bio has also conducted a Phase I/II trial with DCVax-L for late stage ovarian cancer together with the University of Pennsylvania.
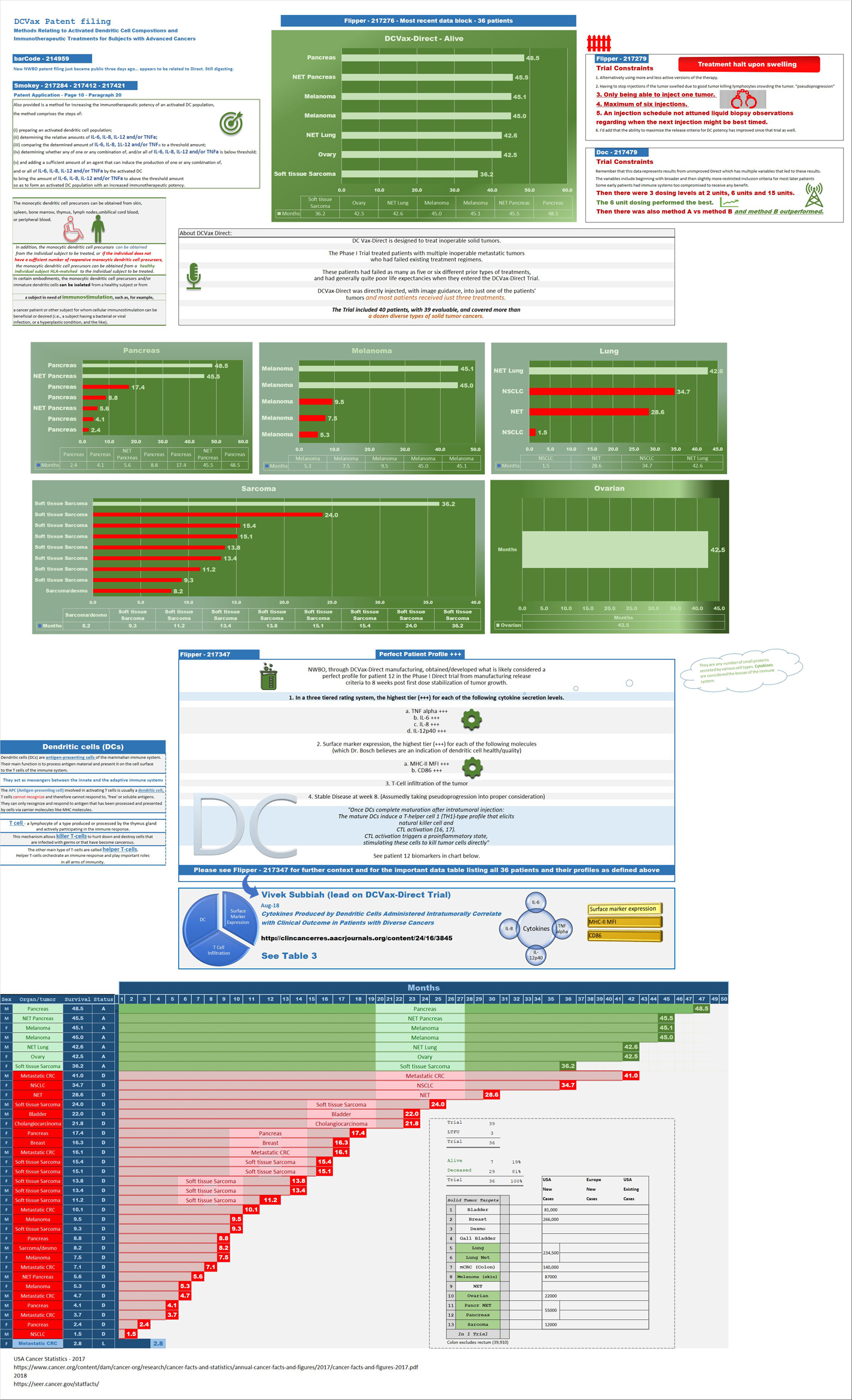
Their second product, DCVax-Direct, is currently in a 60-patient Phase I/II trial for direct injection into all types of inoperable solid tumor cancers, with trials currently being conducted at both MD Anderson Cancer Center in Texas, as well as Orlando Health in Florida.
They previously received clearance from the FDA for a 612-patient Phase III trial with its third product, DCVax-Prostate, for late stage prostate cancer.
DCVAX Survival Stories & Testimonials
Alice - Metastic Merkel Cell patient from Florida - ASCO 2018
Brad Silver - GBM patient from Huntington Beach, California - ASCO 2018
Sarah Rigby - GBM patient from Hong Kong - ASCO 2018
Kristyn Power - daughter of GBM patient from Canada - ASCO 2018
Kat Charles - GBM patients from UK - ASCO 2018 - as related by her husband Jason (Kat's Cure)
Prospective patients may contact NW Bio at patients@nwbio.com
UCLA Jamil Newirth DCVax-Patient Video - 2015
Allan Butler Video - National Geographic Vice President - DCVax-Direct patient from Phase 1 Trial with Pancreatic Cancer
NWBO - Patients Sunday Dennis and Jami Newirth - Enrolled at UCLA - Vimeo, Uploaded approx. May 2015
NWBO - Vaccine Helps Keep Brain Cancer Patient Alive (Jennifer Sugioka) - NBC Channel 4, Southern California, February 24, 2015
NWBO - National Geographic's Allan Butler Stage IV Pancreatic Patient using DCVax-Direct at MD Anderson
NWBO GBM Brain Cancer Survival Story of Mark Pace

Presentations

UCLA Agreements
Prostrate
DCVax-Phase II
DCVax-Booster
Upcoming Events
Videos
Linda M. Liau, MD, PhD, MBA - April 24, 2019 at University of Washington, Neurosciences Institute
| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |




